
Abstract
This is a visual representation of the abstract.
Introduction
As with other parts of the body, eponyms have been commonly used to describe orthopaedic procedures. Several eponyms are used to describe procedures developed for the treatment of hallux valgus. Unfortunately, many orthopaedic surgeons are unaware of the individuals behind the eponym. The purpose of the following review is to describe the commonly used eponyms regarding surgical procedures for hallux valgus in anatomical order from proximal to distal.
Tarsometatarsal Joint
Lapidus procedure
Paul Lapidus (December 27, 1893–November 23, 1981) was born in Russia and from a young age was inspired to pursue a medical career by his father, who was also a physician (Figure 1). 5 Dr Lapidus obtained his medical degree from the University of Odessa Medical School in 1916. Soon after, he enrolled as a captain in the medical corps of the Russian army during World War I (WWI).17,19 He left Russia in 1919. Despite a minimal understanding of the English language, he arrived in New York in 1923 to continue his medical education. His first job was at the Flower-Fifth Avenue Hospital’s kitchen. He then applied for a job at the Hospital for Joint Diseases, where he became the first orthopaedic resident. After graduation, Dr Lapidus remained in New York City as a consultant orthopaedic surgeon for the Hotel Trades Health centre and New York Armed Forces Induction Centre during World War II (WWII). 5 He established the first orthopaedic foot clinic and service at the Hospital for Joint Diseases in 1954, and became a professor at New York Medical. He was one of the founding members of the American Orthopaedic Foot Society. Much of our current understanding of foot and ankle function, anatomy, and pathology is based on his writings. Despite retiring from active practice in 1963, Dr Lapidus continued to write and teach until his death on November 23, 1981.

Dr Paul W. Lapidus. Adapted from: Jahss MH. Dr Paul W. Lapidus. Bull Hosp Jt Dis. 1987;47(2):7-8.
The Lapidus procedure, as originally described, involves arthrodesis of the first tarsometatarsal joint and the bases of the first and second metatarsals for hallux valgus associated with metatarsus primus varus (Figure 2).5,36 Although Albrecht initially described the procedure in 1911, Lapidus popularized the technique in the subsequent years. 5 The original procedure was performed using wood-handled chisels to remove the cartilage and subchondral bone of the joint.19,36 Chromic catgut and postoperative immobilization involving a steel corset were used to stabilize the fusion construct. At the time, intraoperative fluoroscopy was not available, and he relied on direct visualization and his surgical expertise. Today, the Lapidus procedure remains a common procedure to treat hallux valgus in the setting of an elevated intermetatarsal angle.

Original drawing highlighting both joint surfaces undergoing arthrodesis for the correction of hallux valgus. Reproduced from Lapidus, J Am Coll Surg. 1934. Permission obtained from Wolters Kluwer.
Proximal Metatarsal Osteotomies
Ludloff osteotomy
Karl Rudolf Ludloff (June 7, 1864–September 25, 1945) was born in Thuringen, Germany. He studied in Jena, Wurzburg, Munich, and Strasburg. 21 He received his doctorate in Jena in 1894 and became an assistant at the Physiological Institute in Konigsberg and a physician at the Surgical Clinic in the same town and in Breslau. In 1900, he started his surgical training in Konigsberg, becoming titular professor in 1906 and honorary professor in 1913. Dr Ludloff became the director of the University Clinic for Orthopaedic Surgery in Frankfurt, where he was ultimately appointed professor in 1919. 21
His name has been present in various contributions to orthopaedic surgery, including his method for repairing damaged nerves and reestablishing muscular action in German soldiers suffering nerve injuries during WWI using bovine arterial xenograft. 38 Ludloff’s pelvic lesion refers to a vertical fracture through the os sacrum near the sacroiliac joint, whereas the Budinger-Ludloff-Lawen syndrome describes chondromalacia patellae, which is a knee fatigue syndrome seen in children and young adults, adding to his important contributions.15,32
One of Ludloff’s most important contributions to orthopaedic surgery is his technique for the correction of hallux valgus. The Ludloff osteotomy is indicated for moderate to severe hallux valgus deformity. 15 It consists of an oblique osteotomy of the first metatarsal oriented from dorsal-proximal to distal-plantar when viewed in the sagittal plane.3,15 Originally, the osteotomy was stabilized with only plaster of Paris. Further pitfalls and contraindications such as first metatarsocuneiform joint instability, symptomatic first metatarsophalangeal arthritis, severe osteopenia, abnormal distal metatarsal articulation angle, and difficulties maintaining the osteotomy with the use of plaster initially made the technique less popular.3,15
During the late 1900s, however, several surgeons such as Dr Mark Myerson brought new interest regarding this technique with modifications using advances in fixation. 30 The use of pins, screws, and low-profile plates specifically designed for fixation of the Ludloff osteotomy have improved outcomes with a low recurrence rate and the option for triplanar correction, leading to its increased use.3,34 In addition, the Ludloff osteotomy has been reported to have favorable outcomes for the correction of a bunionette deformity. 37
Mau Osteotomy
Carl Mau (July 31, 1880–July 26, 1958) was born in Flensburg, Germany, and studied medicine in Tubingen, Munich, and Kiel from 1908 to 1913. 26 After finishing his studies, he served as a troop and battalion doctor in the 12th Bavarian Infantry Regiment during WWI. He then began his specialist training as an orthopaedic surgeon at the Kiel Surgical University. In 1934, he was appointed the first director of the University Orthopaedic Clinic at Hamburg-Eppendorf. During the following years, he worked to transform his Hamburg workplace, which initially consisted of 4 beds, into a modern European clinic. This was destroyed during a bombing in WWII. It was rebuilt in 1955 and became one of the most modern orthopaedic surgery institutions of the time. Dr Mau was a consulting orthopaedic surgeon for the navy and military, twice chairman of the German Orthopaedic Society, and chaired the war conference in Vienna in 1944. He died in a car accident in 1958.
Dr Mau was particularly concerned with adolescent kyphosis and paralytic scoliosis following the polio epidemic. 26 Regarding foot and ankle, his first interest was clubfoot deformities, on which he performed anatomical studies based on Richard Volkmann and genetic research, which promoted insights about the etiology and pathogenesis of the disease. 26
The Mau osteotomy was first performed in 1915, and has been used in modern times as an alternative to the closing base wedge osteotomy for the metatarsus primus varus component of hallux valgus. 22 This technique consists of an oblique diaphyseal osteotomy that is directed proximal-plantar to distal-dorsal. 33 As originally described, intermetatarsal angle (IMA) correction is less when compared to other more proximal osteotomies because of its relatively distal center of correction. The advantage of the Mau osteotomy is that it is intrinsically stable to dorsal displacement because of its geometry with a long dorsal shelf of bone supporting the distal segment.
Juvara Osteotomy
Ernest Juvara (May 14, 1870–May 5, 1933) was born in Barlad, Romania, and grew up in a farming family (Figure 3). 29 He showed remarkable mechanical skills since childhood and a shy behavior at the same time. These personality traits eventually worked in his favor as his isolation led toward impressive activities for his age, such as disassembling and reassembling a mechanical watch with ease. He finished high school at Saint Sava College in Romania and, in 1888, was accepted at the Paris Medical School. His mentors here were Paul Poirier and Thoma Ionescu. He showed great skills in anatomical drawing as a result of his artistic passion as a young child and was inspired since the beginning of medical school by the drawings of his anatomy professor Louis Hubert Farabeuf.
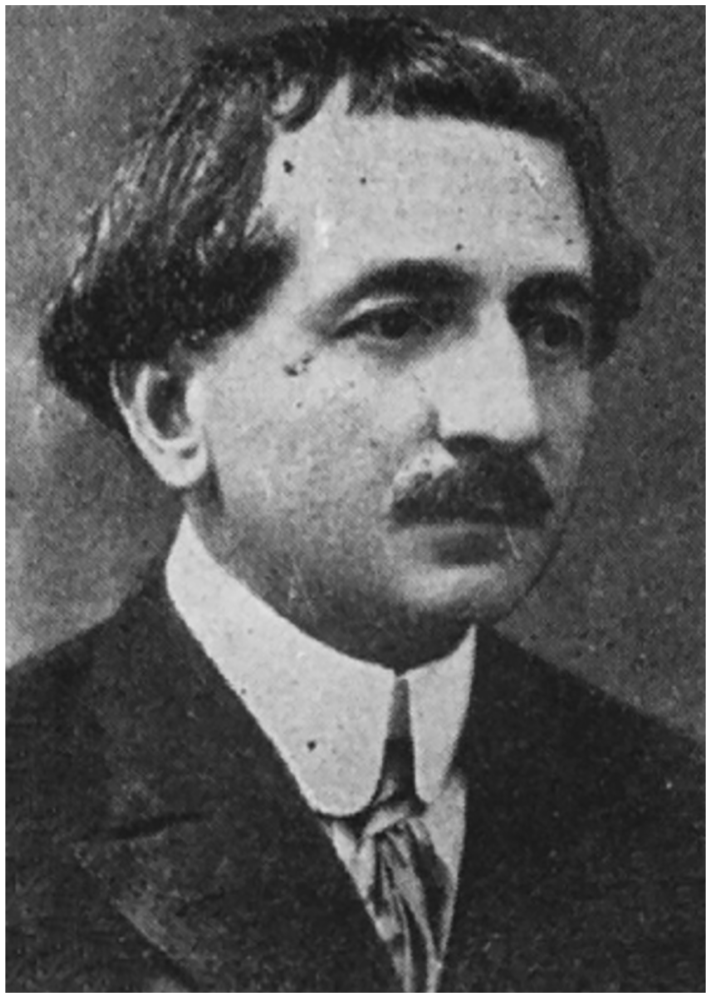
Portrait of Ernest Juvara (1870-1933). Reproduced from Peonaru, Int Orthop. 2018. Permission obtained from Springer Nature.
In 1895, he presented his doctoral thesis in medicine and surgery, which was “extremely well received” by the Paris Medical School. 29 That same year, he returned to Romania with Ionescu and began his surgical and university career. During his time in Paris, he published a successful anatomy book and drew more than 100 anatomy illustrations. His exceptional surgical skills and scientific activity led him to the position of tenured professor of topographic anatomy and clinical surgery at the Iasi Faculty of Medicine at the age of 29 years. Here, he was also the first to introduce spinal anesthesia.
His interest in orthopaedics began during WWI. 29 He put his time into perfecting the spinal anesthesia and developing new surgical treatments for fractures. He invented useful orthopaedic devices described in his landmark paper, Surgical Treatment of Diaphyseal Fractures by External Fixator Method. 29 After the war, his passion remained in orthopaedics, specifically in osteosynthesis. More than a third of his 230 published works and more than 3000 anatomical drawings were dedicated to osteoarticular pathologies. For hallux valgus associated with metatarsal primus varus, he presented the external oblique cuneiform osteotomy performed in the medial third of the first metatarsal diaphysis fixed with metallic pins. 31 Initially coined by M. Loison, Juvara made modifications by performing more vertical cuts, creating greater contact surface area and achieving a more stable fixation (Figure 4). 11

Juvara external oblique cuneiform osteotomy longer cuts allowing for greater surface area for a more stable fixation. Reproduced from Peonaru, Int Orthop. 2018. Permission obtained from Springer Nature.
Distal Metatarsal Osteotomies
Mitchell Osteotomy
Leslie Mitchell was born in Victoria, British Columbia, in 1901 (Figure 5). 28 In 1925, he graduated from the University of Toronto and started his medical internship at Henry Ford Hospital in Detroit. During his rotation with Dr Charles Peabody, who oversaw the orthopaedics service, his interest in orthopaedics grew. At the time, orthopaedics was still a branch of general surgery. General surgeons dealt with closed fractures, while the orthopaedics service handled open fractures that became infected. At that time, no more than 200 operations were performed yearly, and most orthopaedic physicians would spend time making casts in the plaster room. In 1927, Dr Mitchell moved to Portland, Oregon, where he trained for a year in pediatric orthopaedics at Shriner’s. He returned to Detroit and was offered an orthopaedic position at Henry Ford Hospital. At the age of 31 years, he was made head of the division of Orthopaedics. In 1957, the department was separated from General Surgery, and his title was changed to Chair. He held that position until 1967, when he was appointed as a consultant to the department and retired in 1969. Along the way, Dr Mitchell made many contributions of his own and is probably most widely known for the popular bunion surgery that bears his name.

Portrait of Leslie Mitchell D. Reproduced from Mitchell, Henry Ford Hosp Med J. 1987. Figure out of copyright.
Mitchell’s original description of the procedure included an osteotomy of the distal portion of the first metatarsal, lateral displacement and angulation of the head of the metatarsal, and exostectomy with capsulorrhaphy (Figure 6).12,14,27 He highlighted that only correcting the toe deformity without considering correction of the metatarsus primus varus when it was greater than 10 degrees would end in recurrent deformity.

Mitchell osteotomy operative technique demonstrating (A) lateral displacement metatarsal, suture stabilization, and capsular repair. (B) Application of the dressing with tongue depressors. Reproduced from Mitchell L, J Bone Joint Surg Am. 1958. Permission obtained from Wolters Kluwer.
Fixation as described by Mitchell used sutures, reporting adequate results. However, dorsal displacement of the distal fragment causing lesser toe metatarsalgia and hallux rigidus was the main complication. With the advances in fixation, this technique has yielded better results.
Reverdin osteotomy
Jaques-Louis Reverdin (August 28, 1842–January 9, 1929) was born in Cologny, Switzerland. 23 He studied at the University of Paris, becoming an intern in 1865. In 1869, he became assistant to Jean Casimir Felix Guyon, the “Father of Urology” at Necker Hospital in Paris. 2 Afterward, he moved to Geneva, where he eventually became chief surgeon at the Hôpital Cantonal de Geneve, and a professor at the University of Geneva.
In 1869, Reverdin performed the first “fresh skin” allograft. 13 The eponymous “Reverdin graft,” also known as a “pinch graft,” is a procedure for removing small pieces of skin from a healthy area of the body and relocating them to another location that needs coverage. His name is also associated with a specialized surgical instrument known as a “Reverdin needle.” 13 In 1882, with his cousin and assistant Auguste Reverdin (1848-1908), he observed that myxedema occurred as a delayed complication when the thyroid gland was surgically removed. He documented his findings in an article titled Note sur vingt-deux opérations de goitre. He retired in 1910 and dedicated himself to the study of butterflies. He died in Pregny on January 9, 1929.
In 1881, Reverdin first described his osteotomy technique that consisted of the partial resection of the medial exostosis of the first metatarsal head and, in addition, a medially based closing wedge of the distal first metatarsal (Figure 7). This procedure addresses an elevated distal metatarsal articular angle (DMAA). The first cut is performed perpendicular to the long axis of the metatarsal and the second parallel to the articular cartilage, resulting in realignment of the joint surface such that it is perpendicular to the metatarsal shaft. Fixation may be performed with Kirschner wires. Although this procedure and other distal osteotomies were able to realign the first ray, avascular necrosis has been reported to be as high as 20%, likely due to the combination of a lateral release that can damage the plantar-lateral vessels combined with an osteotomy that disturbs intraosseous perfusion. 25 Kuhn et al, 18 using an intraoperative Doppler probe, demonstrated that a lateral release or distal osteotomy alone reduced blood flow minimally; however, when performed together, they reduced it by more than 70%.

Original Reverdin technique consisting of 2 osteotomies, the first perpendicular to the long axis of the metatarsal and the last parallel to the articular cartilage. Reproduced from Salvi, J Foot Ankle Surg. 2011. Permission obtained from The Journal of Foot & Ankle Surgery.
Proximal Phalanx
Akin Osteotomy
Otis Franklin Akin (January 5, 1872–December 28, 1949) was born in Portland, Oregon (Figure 8)9,10 He married Mabel Akin and had one child. 7

Portrait of Otis Franklin Akin. Accessed on June 7, 2024. Figure out of copyright.
The Akin osteotomy was first described in 1925. 1 The procedure captured the scientific community’s attention in the 1960s when Colloff and Weitz published their clinical outcomes with it. 4 Akin described a closing wedge osteotomy of the first proximal phalanx. The original technique was combined with a medial eminence resection of the metatarsal head in line with the medial border of the proximal phalanx. In modern times, an Akin osteotomy is typically used to describe the medial closing wedge osteotomy of the proximal phalanx. 6 It is typically indicated for hallux valgus interphalangeus or an elevated distal metatarsal articular angle (DMAA).
The original osteotomy described by Akin did not include any fixation. However, over the years different fixation techniques have been described, including both suture fixation and fixation with metallic implants (staples, screws, plates, Kirschner wires, intraosseous wire).
Soft Tissue Procedures
Silver Procedure
David Silver (March 16, 1873–March 22, 1946) was born in Ohio (Figure 9). 8 He spent most of his life in Pittsburgh, Pennsylvania, where he married Elizabeth Roadman Silver. He was a WWI veteran and orthopaedic surgeon who performed his bunion correction procedures with Dr Paul Steele at the Allegheny General Hospital. 35 He had a deep understanding of the anatomy and biomechanics of the first metatarsophalangeal joint and was the first to consider soft-tissue procedures for the surgical treatment of hallux valgus. His work was the basis for the McBride procedure. 39 Before Silver’s contribution, only ablational procedures such as the Keller and Mayo resections were available to treat hallux valgus. 24

Portrait of David Silver (1973-1946). Reproduced from Gudi, N N Priorov J Traumatol Orthop. 2019. Figure out of copyright.
First described in 1923, Silver’s procedure has 3 main components. 35 Specifically, the medial eminence of the first metatarsal is removed. In addition, the contracted lateral capsule of the metatarsophalangeal joint is released while the medial capsule is imbricated (Figure 10A). His first clinical report consisted of 49 operations in 39 patients, with good clinical and radiologic results after 2 years of follow-up (Figure 10B). Although he described a lateral capsular release, the Silver procedure is now commonly used to describe a simple medial eminence resection.

Silver operative planning and radiographic outcomes. (A) Capsular approach and repair. (B) Preoperative and postoperative radiologic outcomes. Reproduced from Silver, J Bone Joint Surg Am. 1923. Figure out of copyright.
McBride Procedure
Earl Duwain McBride (1891-1975) grew up in Kansas and Oklahoma (Figure 11). 16 He graduated in 1910 from Epworth University (now Oklahoma City University), and thereafter enrolled at the University of Oklahoma College of Medicine. In 1912, after 2 years in medical school, he transferred to Columbia University in New York where he finished his medical training. He was drafted for military service during WWI and was discharged from the United States Army in 1919. He then started his practice as a general surgeon in Oklahoma City. Soon after, his colleagues encouraged him to take over an orthopaedic practice belonging to Dr Robert Hull at the Hospital for Ruptured and Crippled, today known as the Hospital for Special Surgery (HSS). 20 He focused his training in pediatrics under the tutelage of Dr Royal Whitman and Dr Vigil Gibney. He subsequently returned to Oklahoma in 1920 and realized the need across the state to serve disabled children. He founded the McBride Clinic in 1923, which expanded by connecting with the Reconstruction Hospital, later renamed the Bone & Joint Hospital. In 1943, he obtained approval to establish his hospital as a training institution for residents. He officially retired in 1957.

Portrait of Earl McBride (1891-1975). Reproduced from Gudi, N N Priorov J Traumatol Orthop. 2019. Figure out of copyright.
McBride’s procedure achieves anatomic alignment of the first metatarsophalangeal joint without joint destruction. 24 His technique consisted of releasing the adductor tendon from the base of the proximal phalanx and reattaching it to the head of the first metatarsal to correct the metatarsal varus deformity, excision of the lateral sesamoid if eroded, abnormal in shape or dislocated, and removal of the medial eminence and any associated bursa.24,39 Excision of the lateral sesamoid was abandoned in further modifications. Coughlin and Mann reported hallux varus complication rates of 11%, which led them to cease lateral sesamoidectomy. 39 They stated that hallux varus is mainly due to muscle imbalance, which causes dislocation of the lateral sesamoid.
One of the major contributions of his technique was identifying the importance of contracted muscles whose tendons insert onto the base of the lateral aspect of the proximal phalanx. In contrast to Dr Silver’s procedure, McBride released the conjoined tendon at the base of the phalanx and reattached it to the head of the first metatarsal, in addition to resecting the lateral sesamoid. Interestingly, McBride’s original description did not describe lateral capsular release, nor did it describe medial capsular imbrication.
Conclusion
This review registers the work of orthopaedic surgeons who have expanded our understanding and treatment of hallux valgus deformity. With technological advancements, our management of hallux valgus continues to improve. That said, the essence of the procedures described above remains, and understanding their original descriptions may facilitate surgical execution and future modifications.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251341297 – Supplemental material for A Historical Perspective of Surgical Procedures Used in the Treatment of Hallux Valgus: A Contemporary Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114251341297 for A Historical Perspective of Surgical Procedures Used in the Treatment of Hallux Valgus: A Contemporary Review by Hugo A. Ubillus, Andrew S. Bi, Nina D. Fisher, Thelma R. Jimenez Mosquea and Raymond J. Walls in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.