
Abstract
Background:
This study aimed to determine whether prophylactic celecoxib reduces the prevalence of radiographic heterotopic ossification (HO) following total ankle arthroplasty (TAA). Secondary aims included evaluating its effect on the severity of radiographic HO and its association with patient-reported outcome measures (PROMs).
Methods:
This retrospective cohort study included all patients who underwent a primary TAA between April 2019 to May 2023 at a single academic institution. The intervention group was composed of patients prescribed 4 weeks of celecoxib postoperatively and was compared to controls who received no celecoxib. Radiographs at ≥8 months were reviewed and graded using the modified Brooker classification for severity of HO. Ankle Osteoarthritis Score pain and disability, 36-Item Short Form Health Survey physical function and mental health were assessed at follow-up.
Results:
One hundred seventy-nine patients, 95 males (53.1%) and 84 females (46.9%), were included. The mean age was 65.8 ± 9.6 years. Ninety patients (50.3%) received celecoxib and 89 (49.7%) did not. The prevalence of HO at the time of follow-up (1.2 ± 0.4 years) was 53 (29.6%) with grade 0, 78 (43.6%) with grade 1, 21 (11.7%) with grade 2, 21 (11.7%) with grade 3, and 6 (3.4%) with grade 4. Patients who did not receive celecoxib were significantly more likely to develop HO and experience greater severity of HO, with odds ratios of 2.19 (95% CI 1.10-4.33, P < .05) and 2.51 (95% CI 1.43-4.44, P < .05), respectively. No significant differences in patient-reported outcomes were observed between groups.
Conclusion:
Celecoxib for 4 weeks postoperatively may reduce the risk and severity of HO after TAA without affecting patient-reported outcomes. HO prophylaxis did not have a statistically significant impact on PROMs. Celecoxib for HO prophylaxis can be considered following primary TAA while balancing the risks of side effects.
This is a visual representation of the abstract.
Keywords
Introduction
Ankle arthritis is a source of significant pain and disability for 1% to 2% of the population.6,18,43 Over the last 20 years, total ankle arthroplasty (TAA) has established itself as an efficacious procedure for patients with ankle degeneration. 38 TAA has demonstrated significant improvements in ankle pain while maintaining a functional range of motion. 38
Heterotopic ossification (HO) is a known sequela of total joint arthroplasty. 29 In the setting of TAA, the rate of postoperative HO has been reported to be as low as 22% and as high as 100% at 3 years postoperatively.19,26 The mean overall rate of HO is 66% at 3.6 years postoperatively. 3 Studies have yet to demonstrate significant association between HO and patient-reported outcome measures (PROMs), but this research was either conducted on older-generation implants or on newer-generation implants with small sample sizes. However, more severe HO can have considerable impacts on postoperative range of motion and pain and lead to revision surgery in some patients.2,3,8,12,16,25,29,32,41 Most studies stratify HO using the modified Brooker classification (mBC), similar to hip and knee arthroplasty studies. 29
Patient-specific risk factors for developing HO anywhere in the body include male sex, advanced age, and posttraumatic arthritis.4,12 These are all factors that are commonly seen within the TAA population, which underscores the importance of having effective prophylaxis. Nonsteroidal antiinflammatory drugs (NSAIDs) have been a mainstay in providing prophylaxis against HO. 24 Most literature covers acetabular trauma and HO after total hip arthroplasty (THA).17,24 These studies have demonstrated that celecoxib can be an effective agent in providing prophylaxis against postoperative HO.17,24
To date, no such interventional investigations have been reported in the setting of TAA. Given its success in the THA population, celecoxib was prescribed as HO prophylaxis by the treating surgeon in attempts to reduce the development of symptomatic HO. The goal of this study was to determine whether celecoxib provides effective prophylaxis against HO after TAA. The primary outcome was presence or absence of HO. The secondary outcome of interest was the severity of HO in each cohort, as identified by the mBC. Lastly, we aimed to determine whether 4 weeks of celecoxib postoperatively results in improvement of PROMs. These results should aid in forming standardized postoperative guidelines preventing this known sequela of TAA.
Methods
Study Design
This is a retrospective cohort study of all patients who underwent a primary TAA from April 2019 to May 2023 in a large urban academic hospital. All patients consented to surgery and to enrollment in a Prospective Ankle Reconstruction Registry. Ethics approval was obtained from the hospital research ethics board (REB 14-250). Patients whose index surgeries required take-down fusion, and conversion to TAA or revision TAA were excluded. Additionally, patients who were seen by the preoperative anesthesia clinic and deemed unsafe to take celecoxib due to medical comorbidities were excluded. Patients with a contraindication to NSAIDs were also excluded. The treating surgeon (T.D.) prescribed celecoxib in the form of 200 mg of oral celecoxib daily (100 mg twice daily) for 4 weeks in patients undergoing TAA from March 2021 onward. The treating surgeon (T.D.) detailed the purpose (ie, for HO prophylaxis and not analgesia) and side effects of the celecoxib to each patient at a clinic visit conducted ≤4 weeks before surgery. These patients were than compared to controls; those who were not prescribed celecoxib or any other NSAID were treated before this change in postoperative protocol. No additional NSAIDs were prescribed in the treatment arm, nor were NSAIDs given intravenously perioperatively. Patients were advised not to start any of their arthritis medication until 3 months after their surgery date.
Surgical Procedures
All surgeries were performed by a single foot and ankle (F&A) fellowship-trained surgeon (T.D.) using an extensile anteromedial approach to the ankle 1 with the CADENCE (Smith & Nephew, Memphis, TN) fixed-bearing implant system. They were implanted per the standard operating technique with surgical decision making (including concomitant ancillary procedures) at the discretion of the treating surgeon. The same postoperative analgesic and DVT prophylaxis protocol were prescribed to patients in both groups. No biologic agents were used intraoperatively.
Clinical Outcomes
Baseline preoperative demographics including age, body mass index (BMI), sex, laterality of procedure, and arthritis etiology were collected. Patient-reported outcomes were measured by the Ankle Osteoarthritis Score (AOS) pain and disability subscales, which has been validated for end-stage ankle arthritis and TAA, and the 36-Item Short Form Health Survey (SF-36) physical component summary (PCS) and mental component summary (MCS) scores.9,15,30 The AOS and SF-36 outcome measures were completed concurrently pre- and postoperatively.
Radiographical Outcomes
The presence of HO was determined using postoperative anterior-posterior (AP) and lateral radiographs at the first annual follow-up in both groups. Only bone formed postoperatively was regarded. Radiographs were analyzed for prevalence of HO and classification using the mBC outlined by Lee et al 29 and shown in Table 1 and graphically in Figure 1. These radiographs were reviewed by one senior orthopaedic surgery resident (C.C.) and one fellowship-trained F&A surgeon (M.A.). They were masked to the treatment arm of the study and to the analysis of the other surgeon. Any discrepancies were then rectified by a fellowship-trained F&A surgeon at the treating institution with no prior involvement in the study (M.H.).
Modified Brooker Classification. a
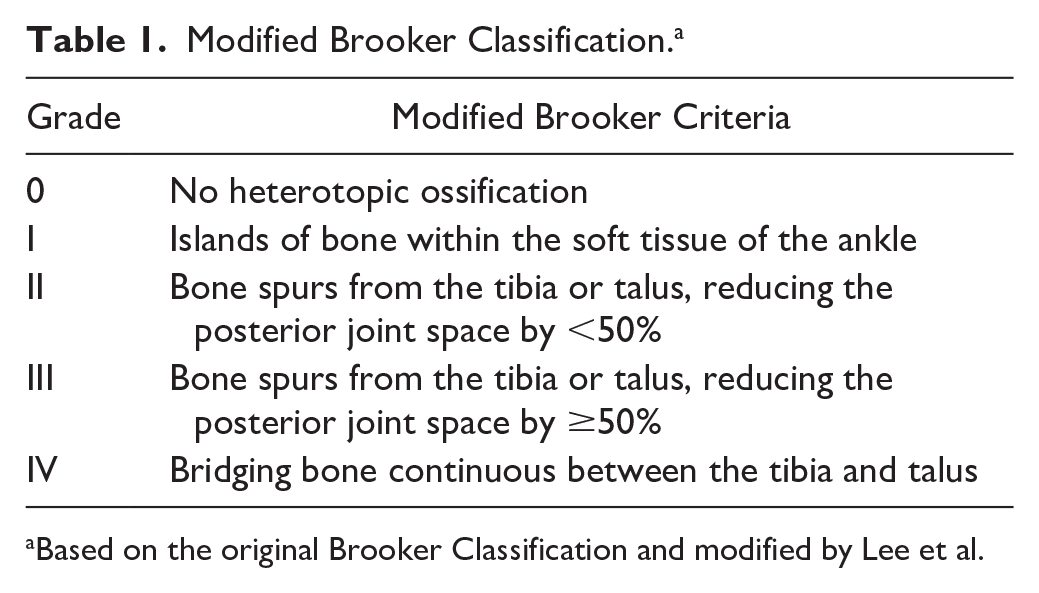
Based on the original Brooker Classification and modified by Lee et al.

Statistical Analysis
Univariate statistics were used to summarize the features of the data set, including mean, SD, and frequency. The independent variable was celecoxib treatment. Dependent variables were radiographic presence of HO, severity of HO (categorical, mBC), postoperative AOS pain, AOS disability, SF-36 PCS, and SF-36 MCS scores. Covariates included age, sex, and BMI.
Logistic and ordinal logistic regression were used to assess the impact of the independent variable on the dependent variables, presence, and severity of HO, respectively, while adjusting for covariates. Lastly, independent samples t tests (or Mann-Whitney U test) were used to determine whether there were statistically significant differences between the PROMs (AOS pain and disability, SF-36 PCS and MCS) of the control and celecoxib groups.
The κ statistic was calculated to evaluate the interrater reliability of both raters for presence and absence of HO as well as severity grading.
Statistical analyses were performed with SPSS (version 28.0; IBM Corp, Armonk, NY), and the level of significance was set at P <.05.
Sample Size Calculation
The prevalence of nonunion in patients who underwent a midfoot arthrodesis for Charcot midfoot arthropathy has been reported to be up to 20%. We considered a 15% difference in the probability of patients developing nonunion to be clinically meaningful. Based on the specified parameters and assuming a 2-tailed t test, a total sample size of 150 was required to achieve a power of 95% to detect a significant difference in the probability of developing nonunion between the 2 groups with a significance level of .05.
Results
One hundred seventy-nine primary total ankles in 179 patients were enrolled between April 2019 and May 2023 at a single large urban academic center who met the inclusion criteria. There were 95 (53.1%) male patients with 97 (54.2%) right TAAs. The mean age of the cohort was 65.8 ± 9.6 years. BMI was 29.5 ± 5.6. The etiology of ankle arthritis was most commonly posttraumatic (n = 126, 70.4%).
A total of 89 patients (49.7%) were in the control group, before celecoxib being added to the postoperative protocol, and a subsequent 90 patients (50.3%) were treated with 4 weeks of celecoxib in the intervention group. One patient had comorbidities precluding the use of celecoxib and was therefore enrolled in the control group. Follow-up radiographs were a mean of 1.2 ± 0.4 years following surgery. Eighteen patients underwent reoperation: 7 in the celecoxib group and 11 in the control group. The most common cause for reoperation in the control group was for symptomatic HO (n = 3, 3.4%), whereas the most common cause for revision surgery in the intervention group was aseptic loosening (n = 2, 2.2%) and symptomatic HO (n = 2, 2.2%). Posterior HO was debrided through a posterolateral incision, whereas anterior HO was debrided arthroscopically. The clinical and demographic characteristics of the intervention and control groups are summarized in Table 2. One patient reported a rash that was believed to be attributed to the celecoxib; however, it was relatively mild and the patient was subsequently advised to complete their 4-week course. No other side effects or adverse events related to celecoxib were reported in postoperative notes.
Demographic Description of Study Cohort.

Abbreviation: PROM, patient-reported outcome measure.
Includes hemochromatosis, postpoliomyelitis, avascular necrosis, and postinfectious etiologies.
The proportion and severity of patients by mBC are summarized in Table 3. The intervention group had 56 (62.2%) with presence of HO (mBC of 1 or higher) compared with 70 (78.7%) in the control group. There was a similar proportion of patients with mBC of 1 HO in the intervention group (n = 41, 45.6%) and the control group (n = 37, 41.6%). Whereas mBCs of 2, 3, and 4 were more common in the control group than in the intervention group (n = 14, 15.7% vs n = 7, 7.8%; n = 14, 15.7% vs n = 7, 7.8%; and n = 5, 5.6% vs n = 1, 1.1%, respectively).
Measures of Heterotopic Ossification.

P values are derived from the logistic regression model, adjusting for age, sex, and body mass index.
The κ statistic was 0.97 for agreement between raters on presence or absence of HO on postoperative radiographs. The κ statistic was 0.90 for HO severity grading using mBC, indicating near perfect agreement.
Logistic regression, using presence or absence of HO as the outcome, demonstrated that the odds of having HO were 2.19 (95% CI 1.10-4.33) times greater for control patients in comparison to patients treated with celecoxib when adjusted for covariates (age, sex, and BMI) (P = .03). There was no statistically significant impact of age (P = .54), sex (P = .07), or BMI (P = 0.10) on the presence of absence of HO.
Ordinal logistic regression to assess the impact of celecoxib on the severity of Brooker HO grade demonstrated that the odds of developing more severe HO were 2.51 (95% CI, 1.43-4.44) times greater for control patients compared with those treated with celecoxib (P = .001). There was no statistically significant impact of age (P = .76) or BMI (P = .07) on the severity of HO. The odds of developing more severe HO were 1.78 times greater for males than females (P = .05).
No statistically significant associations were demonstrated between the control and intervention group with regard to PROMs (AOS pain, AOS disability, SF-36 PCS, and SF-36 MCS). These results are summarized in Table 4.
Measures of Patient-Reported Outcome.
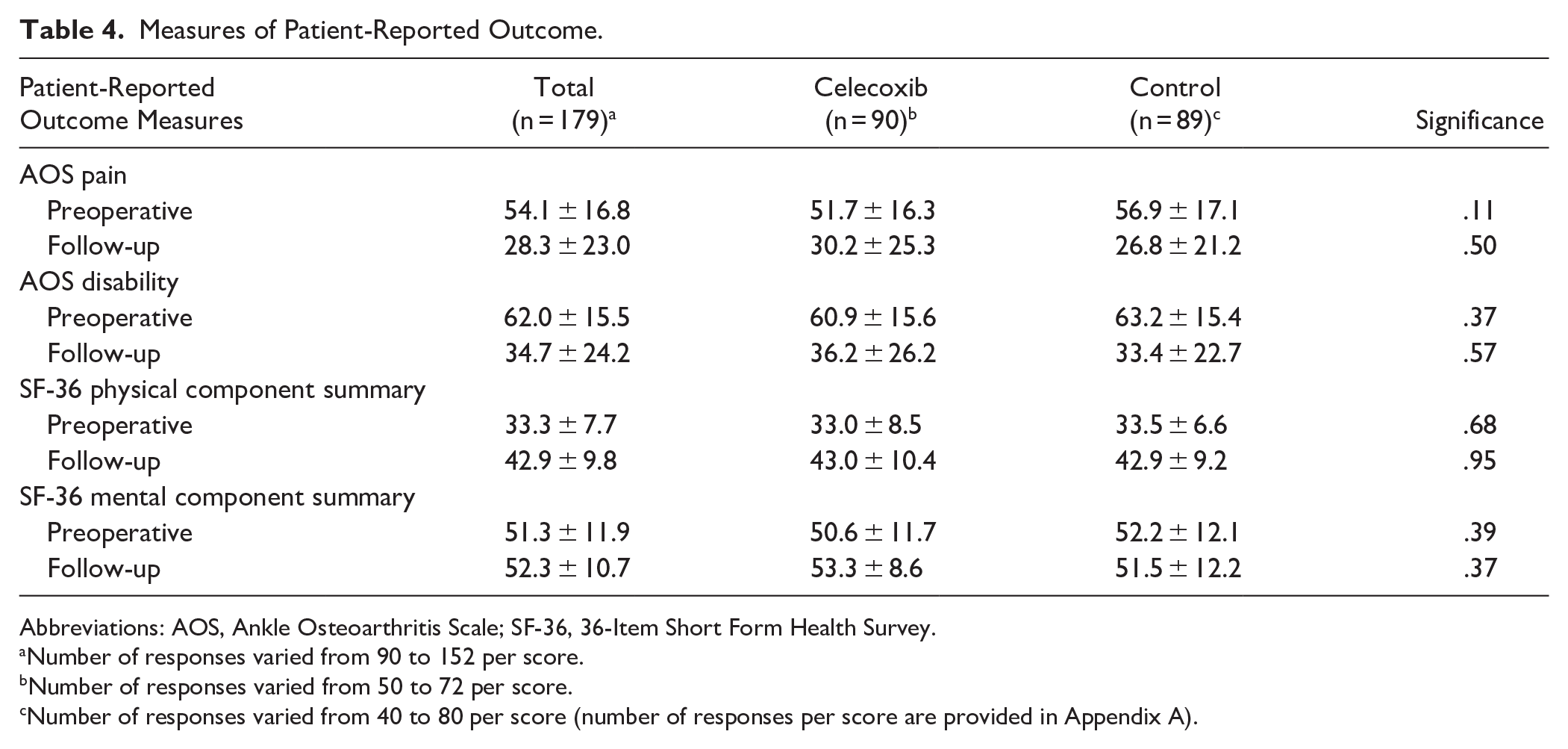
Abbreviations: AOS, Ankle Osteoarthritis Scale; SF-36, 36-Item Short Form Health Survey.
Number of responses varied from 90 to 152 per score.
Number of responses varied from 50 to 72 per score.
Number of responses varied from 40 to 80 per score (number of responses per score are provided in Appendix A).
Discussion
The odds of developing HO following primary TAA at 1-year follow-up were 2.19 (95% CI, 1.10-4.33) times less in patients who had been prescribed 4 weeks of celecoxib (100 mg twice daily) postoperatively (P = .03). The odds of having more severe HO were 2.51 (95% CI, 1.43-4.44) times less in patients treated with 4 weeks of celecoxib postoperatively (P = .001). This is a significant finding given that there are no studies to date evaluating the efficacy of any HO prophylaxis against controls in TAA patients. 3
The prevalence rates of HO for mBC 1, 2, 3, and 4 in TAA in the literature are 39.3%, 14.2%, 19.2%, and 5.6%, respectively. 3 These proportions were relatively in keeping with our study population with HO for grades 1, 2, 3, and 4, which were 43.6%, 11.7%, 11.7%, and 3.4% at a mean follow-up of 1.2 ± 0.5 years, respectively. Although the original Brooker classification is well known and relatively simple to use, it has received criticism. It was originally developed by Brooker et al 5 for use following THA. 21 It has been found to have poor intra- and interobserver reliability in subsequent validation studies.21,45 However, the original classification was based on a single AP projection of the hip joint. The authors for this study used both AP and lateral ankle projections to classify each patient as is suggested in the mBC, which has been demonstrated to increase the intra- and interobserver reliability.21,45
Our results did not demonstrate a significant impact of age or BMI on the presence or severity of HO following TAA at a mean of 1.2 years. This is in keeping with most of the limited literature regarding HO following TAA.2,3,12,29 However, our results did demonstrate that male sex was a significant patient-related risk factor on the severity, but not presence, of HO when compared to females. This is in keeping with the literature in the hip and knee arthroplasty patient population. 46 However, previous studies conducted in the TAA patient population have not demonstrated an association between male sex and development of HO.2,12,29
There is variable evidence for the effect of HO on PROMs and functional outcomes. Valderrabano et al 42 found a statistically significant correlation between presence of HO and measured range of motion in their 68 TAAs using the STAR system. Ten patients required debridement of the HO with or without other indications for revision. 42 Similarly, Lee and colleagues 29 found the rate of HO to be 25% in their retrospective cohort of 80 patients who underwent a TAA using the cementless mobile-bearing HINTEGRA system. Mean ankle range of motion was significantly less in patients with HO compared to those without. 29 Our findings that presence of HO is not associated with poorer PROMs is in keeping with the majority of published literature.2,7,11 -14,19,25 -28,32,36 However, the authors acknowledge that there is a high proportion of missing data for PROMs in this study, which may affect the results.
Although the reported revision rate for HO is <10%, complications rates with revision TAA are high and can have a significant impact. 20 The revision rate of 10.1% presented in this study is relatively in keeping with the literature. The number of reoperations for symptomatic HO was less in the celecoxib group (n = 2) than in the control group (n = 3), but this did not reach statistical significance (P = .31).
There has been concern around the risk of cardiovascular events in patients who take Cox-2 inhibitors leading to rofecoxib to be withdrawn from the market by the Food and Drug Administration in 2004. 10 However, when celecoxib was subsequently compared to naproxen and ibuprofen for risk of cardiovascular events (ie, myocardial infarction, stroke), it was found to be noninferior to both drugs. 35 Celecoxib was also found to have a significantly lower risk of renal and gastrointestinal events when compared to ibuprofen. 40 The known risks attributed to celecoxib must be discussed with the patient and preoperative anesthesia team to ensure the patient does not have any preexisting contraindications. Side effects were not recorded systematically at follow-up within our study, and it therefore is not possible to comment on patient adverse events from celecoxib within this cohort.
NSAIDs have also previously been linked to reduced bony union rates in the trauma literature. 44 However, there remains conflicting evidence on whether NSAID use is associated with decreased osteointegration of arthroplasty implants.31,33,37,44 One study using celecoxib 200 mg twice daily (double the dose used in the current study) for 3 weeks was not associated with increased rates of aseptic loosening 2 years following total knee arthroplasty. 33 Our results demonstrated similar rates of revision for aseptic loosening in our intervention and control groups (n = 2, 2.2%). The impact of celecoxib on osteointegration of TAA has not yet been studied and should be considered as an area for future research.
There are several limitations in this study. There is limited evidence that prosthesis alignment has been associated with specific HO patterns. 32 Namely, varus alignment and anterior tibial tray offset are weakly correlated with HO formation in the ventral and lateral gutters, and the posterior gutter, respectively. Hindfoot alignment and tibial tray position were not radiographically assessed in this present study. Additionally, the surgeon who performed all operations in this study completes approximately 100 TAAs annually and has more than 20 years of experience with TAAs. This could potentially influence PROMs as well as overall postoperative implant alignment and therefore proportion of HO. Ancillary procedures performed alongside the TAA were not accounted for within the regression models and, although there are no data on the degree of correction or number and type of corrective procedures being associated with HO formation, these may have had an effect on HO presence and/or severity. Additionally, these results may not be generalizable to patients with different implants and/or surgical approach than that used in this study. A degree of measurement bias will likely also be present given the variability of grading with the mBC; however, the κ statistic for both presence and severity of HO grading were high (≥0.90), and this is in keeping with the literature.5,45
Arthritis etiology was not used as a confounding variable within the multivariable linear regression model as etiology did not significantly differ between the control and treatment groups and there is no evidence to suggest that this affects the risk of developing HO postoperatively in TAA.29,32 In the hip and elbow, an injury with a traumatic etiology correlates with increased HO, which continues to be an issue following THA or total elbow arthroplasty.4,39 However, this is nearly always due to arthroplasty done acutely in the trauma setting or HO present prior to arthroplasty, which was specifically excluded in the mBC for this study.
Another potential limitation in this study is that because of the consecutive nature of this retrospective study, only the patients enrolled later in the study were prescribed celecoxib, with patients in the control group enrolled earlier in the study because of the addition of celecoxib to the standard postoperative protocol. The authors believe that this would be unlikely to impact the results given that the other postoperative care, surgical approach, implant type, and general standard of care did not change significantly during this time. Additionally, HO takes between 6 and 12 months to “mature” or “stabilize”; therefore, the follow-up periods for each group (mean 1.0 and 1.3 years, respectively) should be reflective of patients’ final postoperative HO severity as per the literature.22,34 However, given that some patients had radiographs performed before 12 months postoperatively, particularly in the celecoxib group, this may underestimate the presence and/or severity of HO. Additionally, the authors were unable to thoroughly assess compliance with the celecoxib prescription in the intervention group given the heterogeneity of clinic note content. However, the treating surgeon met with each patient included in the study within 4 weeks of their surgery and explained the purpose of the celecoxib prescription to minimize nonadherence. Lastly, the cost of celecoxib was not factored in our study. Four weeks of celecoxib would incur an additional cost to patients, given this indication is not covered under the provincial limited use code and thus patients have to pay out of pocket.
There are currently no guidelines for routine TAA HO prophylaxis that exist. Much of the literature supporting NSAID use has been in the total hip arthroplasty and total knee arthroplasty population.4,23,24,46 Valderrabano et al published the only study to date reporting on the rate of HO in TAA in patients with HO prophylaxis using oral indomethacin for 6 weeks postoperatively. They found the rate of HO overall to be 63% but did not have a comparator group. 42 Much of the literature reporting on patients undergoing TAA do not use routine HO prophylaxis.3,11,12,29,32 This is the first study to the authors’ knowledge reporting on the prevalence and severity of HO in patients prescribed celecoxib compared with a control group. This is also the largest cohort of patients with a primary TAA to be assessed for presence and severity of HO in the literature. There is evidence that celecoxib can be an effective agent in providing prophylaxis against postoperative HO. Here celecoxib decreases the incidence and severity of HO after TAA. However, the known side effects of celecoxib such as cardiovascular events, gastrointestinal ulceration, and bleeding also warrant consideration.
Conclusion
The results of this retrospective cohort study of 179 individuals who underwent a primary TAA have demonstrated that HO prophylaxis with 4 weeks of celecoxib (100 mg twice daily) decreases the risk of developing HO and is associated with reduced HO severity. However, no association between HO and PROMs was observed. These results suggest that celecoxib may be effective postoperatively as HO prophylaxis in patients who can tolerate NSAIDs. However, further robust studies are required to compare the efficacy of HO prophylaxis, its impact on clinical outcomes, including revision surgery, and NSAID-related complications.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251337748 – Supplemental material for Celecoxib as Heterotopic Ossification Prophylaxis in Total Ankle Arthroplasty: A Retrospective Cohort Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114251337748 for Celecoxib as Heterotopic Ossification Prophylaxis in Total Ankle Arthroplasty: A Retrospective Cohort Study by Caroline Cristofaro, Mohammad Athar, Ellie B. Pinsker, Brad Meulenkamp, Timothy R. Daniels and Mansur M. Halai in Foot & Ankle Orthopaedics
Footnotes
Appendix
Number of Completed Responses for Each Patient-Reported Outcome Score.

| Total |
Celecoxib |
Control |
|
|---|---|---|---|
| AOS pain | |||
| Preoperation | 107 | 57 | 50 |
| Postoperation | 90 | 40 | 50 |
| AOS disability | |||
| Preoperation | 138 | 73 | 65 |
| Postoperation | 98 | 43 | 55 |
| SF-36 PCS | |||
| Preoperation | 152 | 80 | 72 |
| Postoperation | 114 | 52 | 62 |
| SF-36 MCS | |||
| Preoperation | 152 | 80 | 72 |
| Postoperation | 114 | 52 | 62 |
Abbreviations: AOS, Ankle Osteoarthritis Scale; MCS, mental component summary; PCS, physical component summary; SF-36, 36-Item Short Form Health Survey.
Acknowledgements
The authors thank Ryan Khan and Adam Awoke for assistance with data collection.
Ethical Approval
Ethical approval was obtained from the hospital research ethics board (REB 14-250).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Timothy R. Daniels, MD, FRCSC, reports royalties from Smith & Nephew and has received consulting fees of greater than $10,000 from both Smith & Nephew and Stryker; he received research support from Smith & Nephew, and nonindustry affiliated funds from a Foot & Ankle Research Chair, which supports the salary of Ellie B. Pinsker, PhD. These should not be relevant to the specific manuscript submitted. Mansur M. Halai, BSc(Hons), MBCBhB, MRCA, MRCS, FRCS(Tr&Orth), reports educational fees for less than $5000 from Smith & Nephew and Bonesupport. This should not be relevant to the submitted manuscript. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to participate
All patients consented to surgery and to enrollment in a Prospective Ankle Reconstruction Registry.
ORCID iDs
Data Availability Statement
The data set generated and analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request and discussion with the hospital research ethics board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.