
Abstract
Background:
Tillaux-Chaput tubercle fractures in adults often go unnoticed on standard radiographs in the setting of other malleolar fractures. This study aimed to identify clinical and radiologic factors associated with these fractures to develop a decision aid for computed tomographic (CT) diagnosis.
Methods:
This case-control study included 72 patients with bimalleolar fractures who underwent both radiography and CT scans. The case group consisted of 28 patients with Tillaux-Chaput fractures, and 44 served as control. Sociodemographic, clinical data, and injury mechanisms were compared using univariate and multivariate analysis to identify predictive factors.
Results:
Tillaux-Chaput fractures were undetected on standard radiographs in 60% of cases. In multivariate analysis, only age >60 years and injury mechanisms with Lauge-Hansen pronation-external rotation stage III or IV injuries were found to be highly associated with Tillaux-Chaput tubercle fractures.
Conclusion:
We recommend routine CT scan evaluation for patients >60 years old with stage III or IV pronation-external rotation ankle fractures.
Level of Evidence:
Level III, case-control study.
This is a visual representation of the abstract.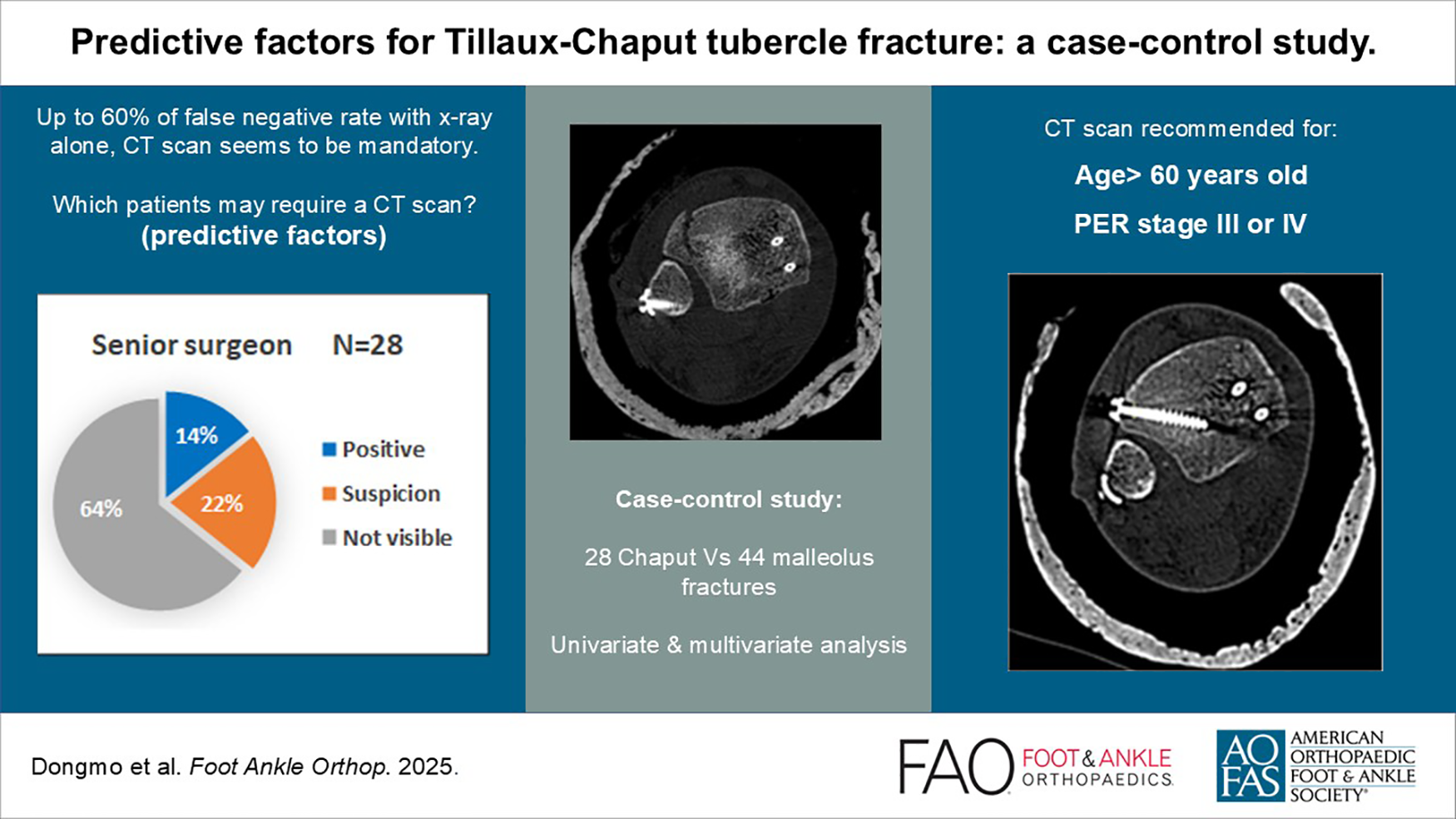
Keywords
Introduction
The Tillaux-Chaput tubercle, also known as the anterior malleolus, is an inferior anterolateral tibial bony prominence that serves as the insertion site for the anteroinferior tibiofibular ligament (AITFL). It was originally described by 2 French surgeons, P. Tillaux in the 19th century and V. Chaput in the 20th century, from whom it takes its name.3,26 Its fracture-avulsion is both a factor of ankle medio-lateral instability because it is equivalent to rupture of the anterior portion of the syndesmosis (AITFL), and an instability in the sagittal plane due to the loss of the mechanical abutment against anterior displacement of the talus (anterior malleolus). Additionally, depending on the size and displacement of the fragment, it can induce a loss of congruence of the tibiotalar joint space and the fibular incisura of the distal tibia.14,23
Tillaux-Chaput tubercle fractures are frequently unrecognized on conventional radiographs, accounting for up to 66.7% of “missed lesions” in ankle trauma. 24 This oversight complicates the development of precise operative strategies, often resulting in suboptimal outcomes characterized by persistent pain, chronic instability, and early joint degeneration. 29 Thus, some studies have reported unsatisfactory functional outcomes for malleolar fracture surgery ranging from 10% to 20% in the short term, and up to 40% to 60% in the long term.2,8 This is despite reductions that are considered acceptable, given that undetected lesions such as syndesmotic ligamentous or bony lesions like the Tillaux-Chaput tubercle fracture may require additional specific surgical steps such as fixation with anchors or transosseous sutures, tension band wiring, and screw or plate fixation depending on fragment size and morphology, performed via an anterolateral approach.10,15,18,27,28,30
Computed tomography (CT) scans, using cross-sectional or 3-dimensional images, provide a more exhaustive assessment of bone lesions. However, the routine use of CT scans for the assessment of malleolar fractures is not currently a standard practice and is typically reserved for complex fractures resulting from high-energy trauma or malleolar fractures involving the posterior malleolus.11,12,19,24,25
This study was designed to test the hypothesis that certain clinical and radiologic factors could predict the existence of a fracture of the Tillaux-Chaput tubercle. The objective was to contribute to the development of a diagnostic strategy for these lesions following malleolar fracture. The present study focuses on a series of patients admitted at a reference trauma center in order to assist in the decision-making process regarding the indication for CT scanning.
Materials and Methods
The university’s ethics committee (reference No. B403201523492) approved the study protocol.
From January 2020 to December 2023, a total of 457 patients aged ≥18 years were treated in our tertiary health care structure for ankle trauma, among which 161 whose imaging workup simultaneously included a radiograph and a CT scan on the PACS system (Picture Archiving and Communication System). Patients with tibial pilon, talus, or calcaneal fractures were excluded from this series, as well as patients with a medical history of fractures, infection, or osteoarthritis of the ankle and foot. Only malleolar fractures were included. A total of 72 patients were selected, 28 of whom were diagnosed as having a Tillaux-Chaput tubercle fracture, based on CT scans as the definitive diagnostic criterion. Sociodemographic characteristics, laterality (dominant side assessed by handiness), weight, body mass index (BMI), fracture classification according to Rammelt et al, and injury mechanisms according to the Lauge-Hansen classification were recorded by 2 independent surgeons from the foot and ankle team according to the simplified algorithm of Arimoto and Forester, with a concordance rate of 82.14%, that is, a Kappa-Cohen score of 0.685.1,17,22 For discordant cases, a third surgeon took the final decision.
In order to assess the contribution of conventional radiography (anteroposterior [AP], lateral and mortise views) to the diagnosis of these lesions, the radiographs of the 28 patients were submitted for interpretation to 3 independent and masked observers, members of the orthopaedic team of different grades and levels of experience (a junior trainee, a junior surgeon, and a senior surgeon). None of the observers had any knowledge of the patients’ medical files or CT scan results.
Clinical characteristics and injury mechanisms of these 28 patients were then compared with the other 44 patients whose ankle scans showed malleolus fractures without Tillaux-Chaput tubercle involvement, thus constituting the control group.
Our data set was analyzed sequentially using descriptive, univariate, and multivariate analyses. Descriptive data were presented as absolute and relative frequencies. Univariate analysis consisted of comparisons using χ2 or Fisher tests. Multivariate analyses involved a logistic regression model to identify risk factors of Tillaux-Chaput tubercle fracture. Included variables were selected based on univariate analyses. Absence of multicollinearity was verified by a variance inflation factor <5. The most accurate model was chosen based on its deviance and the likelihood ratio test (LRT). All tests were 2-sided and the statistical significance threshold was set for P values <.05. All analyses were performed using SigmaPlot software (v.13.0.0.83; Systat Software, Inc, Germany).
Results
Our population included 72 patients with ankle trauma who had simultaneously undergone an ankle radiography and CT scan as part of their imaging workup. Twenty-eight of these patients had a fracture of Tillaux-Chaput tubercle, that is, 9 men (32.14%) and 19 women (67.86%), for a sex ratio of 0.47.
All our patients had a dominant right side. Twenty fractures (71.43%) were on the right ankle and 8 (28.57%) on the left. The main injury mechanisms observed were domestic accidents (ground-level fall or fall down stairs) (21; 75%) and sports accidents (5; 17.86%), with energy levels ranging from low (10; 35.71%) to moderate (15; 53.57%) in the majority of cases. Fifteen patients (53.57%) were overweight (BMI ≥ 25) or obese (BMI ≥ 30).
Patterns of injury according to the Lauge-Hansen classification were dominated by external rotation, with 25 cases (89.29%) comprising 13 (46.43%) supination-external rotation (SER) and 12 (42.86%) pronation-external rotation (PER). In 3 cases (10.71%), the mechanism was pronation-abduction (PA).
According to Rammelt’s classification, 15 patients (53.57%) were classified as type 1, 5 (17.86%) as type 2, and 8 (28.57%) as type 3. Tillaux-Chaput tubercle fracture was associated with simultaneous fracture of the lateral, medial, and posterior malleoli in 13 patients (46.43%), with isolated fracture of the lateral malleolus in 6 (21.46%) patients, and fracture of the lateral and medial malleoli only in 5 (17.86%) patients, 4 patients had isolated Tillaux-Chaput fracture as a form of high ankle sprain (Table 1).
Clinical and Radiologic Characteristics of the Tillaux-Chaput Tubercle Fracture Population.

Abbreviations: BMI, body mass index; DA, domestic accident; F, female; L, left; M, male; PA, pronation-abduction; PER, pronation-external rotation; R, right; RTA, road traffic accident; SA, sport accident; SER, supination-external rotation.
Based on conventional radiograph analysis alone, all 3 observers had a false-negative rate of almost 60%. The diagnosis was certain in only 3 cases (11%) for the junior trainee and junior surgeon and in 4 cases (14.29%) for the senior surgeon (Figure 1). Overall, we did not find a significant association between the type of Tillaux-Chaput fracture and the false-negative rate, with the exception of the type 3 fracture in young surgeons (OR 0.143, 95% CI 0.022-0.922; P = .044) (Table 2).

Evaluation of the contribution of ankle radiography in the diagnosis of Tillaux-Chaput tubercle fracture.
Association Between Tillaux-Chaput Fracture Type and Rate of False-Negative Diagnosis.

Abbreviation: OR, odds ratio.
Boldface indicates significance (P < .05).
Comparing clinical and radiographic characteristics of patients with a Tillaux-Chaput tubercle fracture to those of the control group in a univariate model, we observed a significant association with the occurrence of Tillaux-Chaput tubercle fracture in patients aged ≥60 years (OR 4, 95% CI 1.45-11.01; P ≤ .01) and with trauma to the dominant side (OR 3, 95% CI 1.09- 8.25; P ≤ .05). With the numbers available, no significant difference was found between the 2 groups in terms of gender, BMI, or a particular trauma circumstance or energy levels.
However, we observed a significant difference in terms of injury mechanisms. More external rotation mechanisms (OR 4.66, 95% CI 1.14 -27.91; P = .026) were found in the Chaput fracture group and more specifically in stage III and IV PER (OR 15.08, 95% CI 2.89-153.37; P = .0001) according to the Lauge-Hansen classification (Table 3). The presence of associated lesions was not statistically different between both groups.
Comparison of the Tillaux-Chaput Tubercle Fracture Population With the Control Group (Univariate Analyses).

Abbreviations: BMI, body mass index; DA, domestic accident; F, female; L, left; LM, lateral malleolus; M, male; MM, medial malleolus; OR, odds ratio; PA, pronation-abduction; PER, pronation-external rotation; PM, posterior malleolus; R, right; RTA, road traffic accident; SA, sport accident; SER, supination-external rotation.
Boldface indicates significance (P < .05).
In multivariate analysis, however, only age >60 years and injury mechanisms in PER stage III or IV injuries were found to be predictive of Tillaux-Chaput tubercle fractures in our study (Table 4).
Multivariate Analysis.

Abbreviations: OR, odds ratio; PER, pronation-external rotation.
Boldface indicates significance (P < .05).
Discussion
Various cadaveric and clinical studies describe the functions of Tillaux-Chaput tubercle: it forms the anterior portion of the inferior fibular groove of the tibia and thus helps stabilizing the syndesmosis. Because of the insertion of the AITFL, it limits posterior translation and external rotation of the fibula and also prevents anterior translation of the talus, acting as an anterior malleolus.20,23 Its fracture is a major factor in ankle instability and can lead to incongruence of the tibiotalar joint and fibular groove of the distal tibia, which can lead to an inadequate closure of the syndesmosis and necessitate revision surgery in some cases.13,19,20,21 Diagnosing Tillaux-Chaput tubercle fractures is therefore essential for optimal treatment of malleolar fractures.7,18
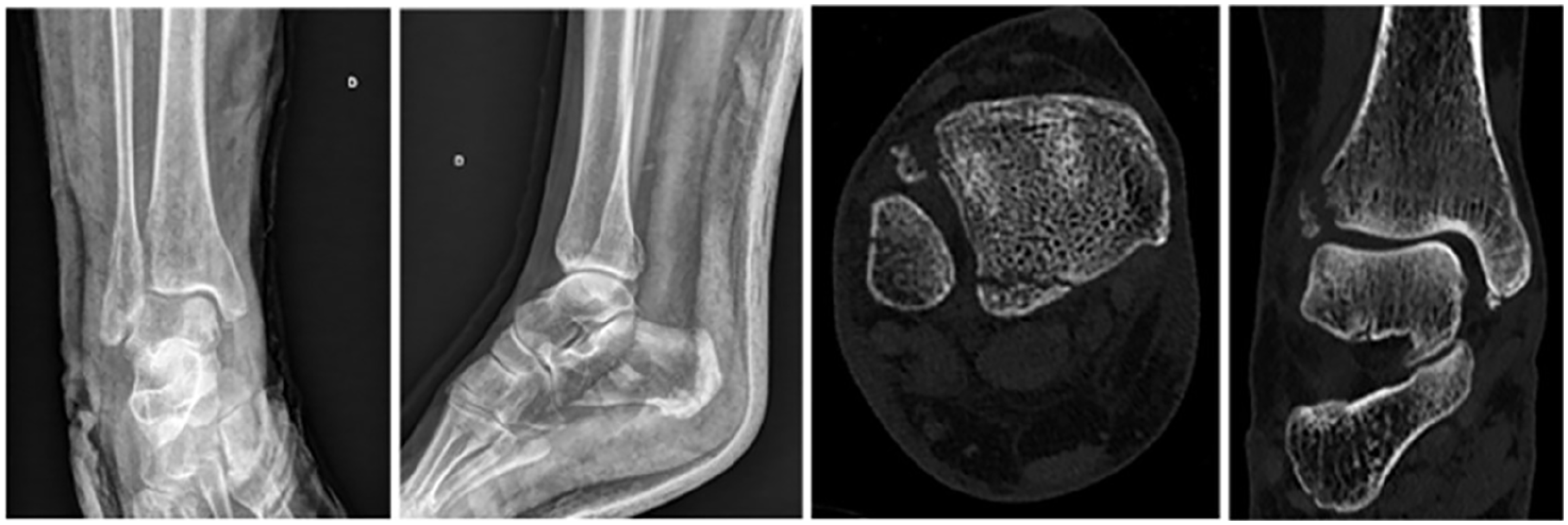
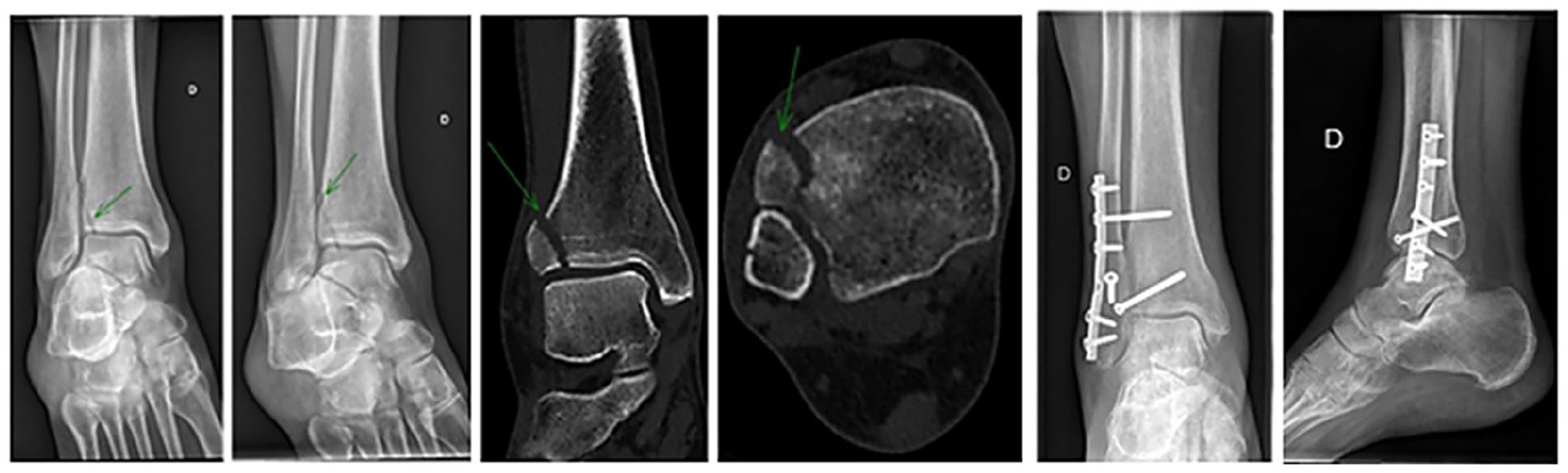
Standard radiography (AP, lateral, and mortise views) is routinely prescribed for initial exploration of ankle trauma.24,29 However, this imaging modality does not easily visualize the syndesmosis area or the Tillaux-Chaput tubercle because of its superposition to the posterior side of the fibular groove of the tibia (posterior malleolus) and the talar dome depending on the degree of ankle flexion on an AP view.4,6,11,14 This explains the almost 60% false-negative rate for all experience levels of examiners in our study and the 66.7% missed lesion rate (eg, Figures 2 and 3) in studies using CT to assess malleolar fractures. 24 Large fragments (Rammelt type 3) may be visualized as a discrete fracture line or impaction of the lateral side of the tibial articular surface, causing joint space discontinuity on AP and mortise views (Figure 4). 29 Smaller fragments (Rammelt 1 and 2) may occasionally be visible as irregular punctiform opacities projected onto the distal fibula or tibiofibular space (Figure 5).

Rammelt type 2 Tillaux-Chaput tubercle fracture found on postoperative computed tomographic scan (missed lesion) and fixed with 2 screws.
Tillaux-Chaput tubercle fracture unnoticed on radiographs, visible on preoperative computed tomographic scan.
Large Rammelt type 2 displaced Tillaux-Chaput tubercle fracture visible on radiographs and computed tomographic scan.

Rammelt type 2 Tillaux-Chaput tubercle fracture (green arrow) visible as a punctiform irregular opacity on a lateral radiographic view, confirmed by computed tomographic scan.
Numerous studies have highlighted the benefit of systematic CT scanning of ankle fractures to accurately map lesions and diagnose those easily missed on radiography.11,12,19,24,25 CT scans are now almost routinely used for most joint fractures but not yet for ankle fractures. Identifying patients at risk of Tillaux-Chaput tubercle fractures based on clinical and initial radiographic findings could aid in deciding to perform a CT scan.
Our study population showed a slight female predominance, with an average age of 60 years and a preferential involvement of the dominant side. Rammelt et al 17 found a similar population with an average age of 58 years and an equivalent sex distribution. The dominant lower limb is more prone to traumatic injury in the athletic population, but this constant does not appear to have been demonstrated in the general population. 5
The risk of fracture in subjects with obesity is site-specific, with a reduced risk of certain types of fracture (eg, hip, pelvis, and wrist) and an increased risk of fractures at other sites (eg, humerus, ankle, shoulder, vertebrae, and ribs). 13 In our study, obesity did not have a significant effect on the occurrence of Tillaux-Chaput tubercle fracture specifically.
The most common circumstances surrounding these fractures were domestic accidents and falls, with a few sports-related accidents in younger patients, typically involving low to moderate energy levels. No significant association was observed between any particular circumstance or energy level and the occurrence of these fractures.
The mechanisms of Tillaux-Chaput tubercle fractures remain to be fully clarified. Cadaveric and radiologic studies suggest they occur preferentially through external rotation or abduction mechanisms.9,16 The rupture of the AITFL is the first stage of Lauge-Hansen’s SER mechanism.4,22 In our study, external rotation mechanisms were identified as the primary cause of injury, accounting for nearly 90% of cases. Of these, PER mechanisms (stage III or IV) were found to be the most strongly associated with these fractures. Although SER mechanisms were also prevalent in our study population, they were not specific to Tillaux-Chaput tubercle fractures. No cases of supination-adduction mechanisms were observed. Various descriptive studies have also found SER or PER mechanisms to be associated with Tillaux-Chaput tubercle fractures.17,27,28
It is important to acknowledge several limitations of this study. First, the relatively small sample size is due to the nonroutine prescription of CT scans for ankle trauma. Additionally, the control group may be subject to selection bias because CT scans in our department are primarily indicated for complex fracture lines and trimalleolar fractures, which may not represent the entire source population. However, selecting patients with ankle CT scans for the control group was mandatory to ensure a negative diagnosis of Tillaux-Chaput tubercle fracture in that population.
Conclusion
Fractures of the Tillaux-Chaput tubercle are among the most poorly explored lesions in ankle trauma. Establishing a typical profile for patients likely to present this lesion based on clinical and radiographic interpretation alone is challenging because of small sample sizes in various studies. Based on our results, and pending larger studies, we recommend CT scanning for malleolar fractures in patients >60 years of age with the presentation of a stage III or IV PER injury.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251332940 – Supplemental material for Predictive Factors for Tillaux-Chaput Tubercle Fracture: A Case-Control Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114251332940 for Predictive Factors for Tillaux-Chaput Tubercle Fracture: A Case-Control Study by Cédric Dongmo Mayopa, David Ancelin, Pauline Despontin, Julie Manon, Gaspary Fodjeu, Randy Buzisa Mbuku, Maxime Masscheleyn, Olivier Cornu, Karim Tribak and Dan Putineanu in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Hospital and Faculty Ethics Committee of UCLouvain (Approval number: B403201523492).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Ancelin, MD, reports disclosures relevant to manuscript of royalties from FHOrtho and consultancy fees from FHOrtho, Orthofix, and Arthrex. Olivier Cornu, MD, PhD, reports disclosures relevant to manuscript from Zimmer-biomet (prospective study on Avenir cemented stem and biofilm-related implant infection), Fond National Recherche Scientifique, Stryker, Fondation Saint-Luc/Fond Prof Christian Delloye, Region Wallone Win2Wal, and Region Wallone Biowin. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.