
Abstract
Background:
Deltoid repair (DR) in ankle fracture surgery remains controversial. This study aims to determine whether DR reduces complications and improves outcomes measured by Patient Reported Outcomes Measurement Information System (PROMIS) computerized adaptive tests (CATs) of physical function (PF) and pain interference (PI). We hypothesized that DR would reduce complications and improve PROMIS scores.
Methods:
This was a retrospective study of 782 patients at a single institution who underwent ankle fracture surgery between January 2016 and December 2021. Two fellowship-trained foot and ankle orthopaedic surgeons independently reviewed all radiographs and assessed reduction quality and complications at final follow-up. Multiple extremity injuries, open fractures, and pilon variants were excluded. A total of 345 patients with deltoid ruptures were sent PROMIS CATs. Of those, 265 patients with minimum 1-year follow-up were analyzed for complications. Finally, 112 patients who completed CATs were analyzed for PROMIS. Wilcoxon rank-sum test compared PROMIS between groups. Linear regression modeled DR effect on PROMIS adjusted for relevant covariates and propensity scores.
Results:
Fifty of the 265 patients (18.9%) underwent DR. The incidence of radiographic evident complications among 215 patients (81.1%) without repair (NDR) was 14.42%: 7 (3.26%) degenerative joint disease, 3 (1.40%) ankle joint malreduction, 4 (1.86%) syndesmotic malreduction, and 8 (3.72%) malleolar malunion. The DR group had no radiographic complications. Among patients who completed CATs (n = 112), DR (n = 21) was not significantly different for mean PF (54.31±9.83 vs 52.79±10.42, P = .71) or mean PI (47.21±7.82 vs 48.53±8.37, P = .59) than NDR (n=91). Adjusted regression models estimated a 1.89-point increase in PF and a 1.67-point decrease in PI for DR vs NDR. When adjusted for propensity scores, DR had PF 2.17 higher and PI 1.73 lower compared to NDR. Neither of these reach minimal clinically important difference criteria.
Conclusion:
DR was associated with reduced radiographically evident complications following ankle fracture surgery. This study was underpowered to detect small effect sizes in PROMIS, and we remain uncertain if DR meaningfully improved patient-reported outcomes.
Level of Evidence:
Level IV, retrospective case series study.
This is a visual representation of the abstract.
Introduction
The deltoid ligament complex serves as the primary stabilizer of the axially loaded ankle: the superficial deltoid resists hindfoot eversion, whereas the deep deltoid counters external rotation of the talus relative to tibia. 23 Ten percent to 58% of ankle fractures have associated deltoid injury.16,24,41
Despite the high incidence of deltoid ruptures in ankle fractures, operative repair remains controversial.6,23,26,37,41 Several studies suggest that deltoid repair (DR) reduces complications including syndesmotic malreduction, improving overall joint alignment.2,25,32,33,40,42,44 Other literature argues DR is not necessary and increases operative time.1,10,36,38 Similarly, mixed data exist on whether DR improves function and postoperative pain. Several studies support improvement in functional outcomes, pain scores, and return to activity following DR,3,11,14,18,31 whereas others reveal no significant differences in functional outcomes as measured by American Orthopaedic Foot & Ankle Society (AOFAS) scores between DR and no deltoid repair (NDR).1,10,23,32,33,38,40,42,44
There exists a patient-centered shift in orthopaedic literature toward using patient-reported outcome measures (PROMs) to evaluate what patients view as successful treatment. However, the most commonly used legacy instruments in foot and ankle surgery (Foot and Ankle Ability Measure, Foot Function Index, AOFAS, and visual analog scale) do not consistently demonstrate validity, reliability, or standardizability. 35 This shift has led to the development of the Patient-Reported Outcomes Measurement Information System (PROMIS). The responsiveness, validity, decreased floor and ceiling effects, time efficiency, and T score–based scoring system are all contributing factors to the adoption of PROMIS by health care systems nationwide. 5
Limited data exist comparing outcomes as measured by validated PROMIS computerized adaptive tests (CATs) of physical function (PF) and pain interference (PI) between patients who undergo DR and those treated without deltoid fixation. Rigby et al 31 found significant improvements in PROMIS following DR, although this study did not compare differences in PROMIS between DR and NDR.
Because PROMIS demonstrates substantial reliability in detecting clinically meaningful differences in outcomes following ankle fracture surgery, further understanding of the impact of DR on PROMIS would provide clearer insight into the role of DR in ankle fracture surgery.8,19,21 This study aims to determine whether DR reduces complications and improves PROMIS scores. To our knowledge, this investigation is the largest retrospective study in the published literature comparing PROMIS scores of patients who underwent DR to those who underwent operative fixation NDR. We hypothesized that DR would reduce complications and improve PROMIS scores compared to NDR.
Methods
Population
This study was an institutional review board (IRB)–approved retrospective review of 782 patients at a single institution who underwent ankle fracture surgery between January 2016 and December 2021. All surgeries were performed by fellowship-trained orthopaedic surgeons in either foot and ankle (n=4) or trauma (n=3). Two fellowship-trained foot and ankle orthopaedic surgeons independently reviewed all radiographs and assessed reduction quality and radiographic complications at final follow-up. Multiple extremity injuries, open fractures, and pilon variants were excluded. Of 703 patients remaining, 345 had concomitant deltoid rupture and were sent postoperative questionnaires via REDCap containing PROMIS CATs and surveys querying activity limitations due to fear of reinjury (FORI) with a binary yes/no answer choice. 15 Deltoid ligament rupture was radiographically identified by injury films, defined as a ≥2-mm difference between the superior clear space and the medial clear space, or stress positive with same criteria. Patients with a concomitant posterior malleolus fracture underwent additional anatomic reduction and fixation. Patients with concomitant syndesmotic rupture underwent stabilization via the Syndesmosis TightRope XP (Arthrex, Naples, FL). Surgeon preference determined choice of DR (direct end-to-end repair, suture anchors) based on the above criteria. The traumatology department does not believe in DR. The foot and ankle colleagues believe in DR based on literature and biomechanical understanding of fractures. Of the 365 patients identified, 265 with a minimum 1-year radiographic follow-up were included in the final analysis. Fifty of those 265 underwent fixation with DR and 215 underwent fixation NDR. Finally, 112 of the 345 patients who completed postoperative surveys containing PROMIS CATs were analyzed for functional outcomes. Patients completed CATs at minimum 1-year follow-up, but were necessarily at different time points postoperatively.
Surgical Technique
When repaired, deltoid is fixed after open reduction and internal fixation (ORIF) of the fibula prior to syndesmosis evaluation and stabilization. A 4- to 5-cm incision is made over the anterior one-third of the medial malleolus, deep dissection carried down to the deltoid, with care taken to identify and protect the saphenous neurovascular bundle. If transligamentous disruption of the deltoid is visualized—and there is still sufficient ligament attached to the medial malleolus—suture repair is performed consisting of end-to-end repair and imbrication of the deltoid with heavy absorbable suture (No. 0 Vicryl). If the deltoid is avulsed proximally with a coinciding bare area on the medial malleolus, repair is performed using a DX FiberTak all-suture anchor (Arthrex, Naples, FL). Careful positioning maintains the foot in neutral dorsiflexion and inversion during repair.
Outcomes
The primary outcome was postoperative PROMIS PF and PI. Secondary outcomes included radiographic and surgical complications. Postoperative radiographic complications were defined as: degenerative joint disease (DJD), end-stage arthritis (ESA), malleolar malreduction, syndesmotic malreduction, malleolar malunion, nonunion, deltoid calcification, and synostosis. Surgical complications were collected from chart review and were defined as: venous thromboembolism (deep vein thrombosis and pulmonary embolism), deep wound complications, and reoperation within 1 year.
PROMIS was developed for scores of 50 referring to the US population mean. 20 Higher PF scores indicate better physical function. Higher PI scores mean more pain interference with activity. The minimal clinically important difference (MCID) for PROMIS is a change of 3 to 30 in T scores.19,28 The MCID was initially determined comparing scores among individuals but can be used to compare differences in scores cross-sectionally. Hung et al. concluded that reporting an MCID range is more valuable than providing a single value, which can be misleading in clinical practice. The lower-end range may be useful for screening tasks (such as patient ability to perform activities, as evaluated in our study), while the higher-end range may be more helpful for higher-stake decisions (returning to high-intensity athletics or need for surgery, which were not evaluated in our study). The interquartile range (IQR) may be the most helpful for making decisions. 20
Statistical Analysis
Hypothesis-driven testing (whether DR improves PROMIS scores) analyzed with R Version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria) was used. Wilcoxon rank-sum test was used to compare post-operative PROMIS scores between groups. This study had 80% power to detect a large difference (Cohen’s d=0.68) in mean PROMIS scores between groups, translating to a minimum detectable difference of 5.6 in mean PI and 6.9 in mean PF. Multivariable linear regression was used to assess the effect of DR on PROMIS adjusting for clinically relevant covariates. To address imbalances in baseline characteristics, we conducted both covariate-adjusted and propensity score–adjusted linear regression analyses to assess potential residual confounding. Propensity scores were estimated using logistic regression, representing each patient's probability of receiving treatment based on baseline characteristics. Both propensity score–adjusted and covariate-adjusted models were further adjusted for FORI. Results from both approaches were comparable. In adjusted regression models, this study had 80% power to detect a minimum difference of 3.1 in PROMIS PI and 3.8 in PROMIS PF (alpha level 0.05).
Prior literature demonstrated that FORI limits patients’ outcomes following ankle fracture surgery. 12 Fear was thus included as binary covariate in regression models based on survey responses.
Subgroup analyses were conducted to evaluate outcomes by fracture subtype, including both number of malleoli involved (isolated lateral malleolus vs lateral malleolus and posterior malleolus) and Weber classification (Weber B [WB] vs Weber C [WC]).
Perfect separation in data limited reliability of statistical tests to assess incidence of complications by DR.
Clinical follow-up was defined as time from surgery to last contact. Radiographic follow-up was defined as time from surgery to last ankle radiographs.
Results
Table 1 displays baseline characteristics. Table 2 demonstrates no significant differences in characteristics of survey responders vs nonresponders. Of 265 included patients who underwent operative ankle fracture fixation with concomitant deltoid rupture, 50 (18.9%) underwent DR and 215 (81.1%) were NDR. 11.70% (31/265) had postoperative radiographic complications. 5.66% (15/265) had postoperative surgical complications. There were 199 isolated fibula fractures and 61 lateral malleolus and posterior malleolus fractures. A total of 206 were WB (161/206 isolated fibula) and 59 were WC (38/59 isolated fibula).
Patient Characteristics. a

Abbreviations: CAT, computerized adaptive test; PROMIS, Patient Reported Outcomes Measurement Information System.
Data are expressed as n (%).
Characteristics by Response to PROMIS Survey. a

Abbreviation: PROMIS, Patient Reported Outcomes Measurement Information System.
Data are expressed as n (%).
Among 215 NDR patients, overall radiographic complication rate (Supplementary Table S1) was 14.42%: 7 DJD (3.26%), 1 ESA (0.47%), 3 ankle joint malreduction (1.40%), 4 syndesmotic malreduction (1.86%), 8 malleolar malunion (3.72%), 2 deltoid calcification (0.93%), and 7 synostosis (3.26%). A total of 202 patients (93.95%) demonstrated anatomic reduction of the ankle at final follow-up.
Among 50 DR patients, no postoperative radiographic complications were observed (Supplementary Table S1). All (100%) of the DR patients achieved anatomic reduction at final follow-up.
Table 3 displays complications by fracture subtype. In subgroup analysis of isolated fibula fractures (n=199), the overall complication rate in the NDR group (n=161) was 11.18% (18/161): 6 DJD (3.73%), 1 ankle malreduction (0.62%), 2 syndesmotic malreduction (1.24%), 1 syndesmotic calcification (0.62%), 4 malleolar malunion (2.48%), 5 synostosis (3.11%), and 2 deltoid calcification (1.24%). There were no radiographic complications in the DR group (n=38). All (100%) of the DR patients achieved anatomic reduction at final follow-up compared with 95.65% (154/161) of NDR patients.
Incidence of Complications by Fracture Subtype. a

Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
Of the 265 patients, only n=5 had a bimalleolar fracture. None of these 5 had a radiographic complication and 1 had a wound complication. All data are expressed as n (%).
Overall incidence of postoperative complications was similar between groups both overall (Supplementary Table S1) and in subgroup analyses (Table 3). In NDR, the overall incidence of postoperative complications was 5.12%: 8 venous thromboembolism (3.72%) and 4 deep wound infections (1.86%). Overall, 37 patients (17.21%) underwent reoperation (see Supplementary Materials for reoperation reasons). Among DR patients, the overall incidence was 8.0%: 2 venous thromboembolism (4.0%), 1 deep wound infection (2.0%), and 7 reoperation (14%) (Supplementary Materials).
Among patients who completed postoperative survey CATs (n=112), DR (n=21) was not significantly different for mean PF (54.31±9.83 vs 52.79±10.42, P = .71) or mean PI (47.21±7.82 vs 48.53±8.37, P = .59) than NDR (n=91) (Figures 1 and 2). No significant differences existed in ability to return to preinjury levels of activity between groups (Figure 3). There was no significant difference in reported FORI between groups (Figure 3). In the subgroup of isolated fibula fractures (n=83), NDR (n=68) had a mean PF of 53.3±10.6 and a PI of 48.0±8.5. DR (n=15) had a mean PF of 55.5±11.0 and a PI of 46.9±7.9 (P=.69 and P=.75, respectively, Figures 1 and 2).

PROMIS physical function by receipt of deltoid repair. PROMIS, Patient Reported Outcomes Measurement Information System.
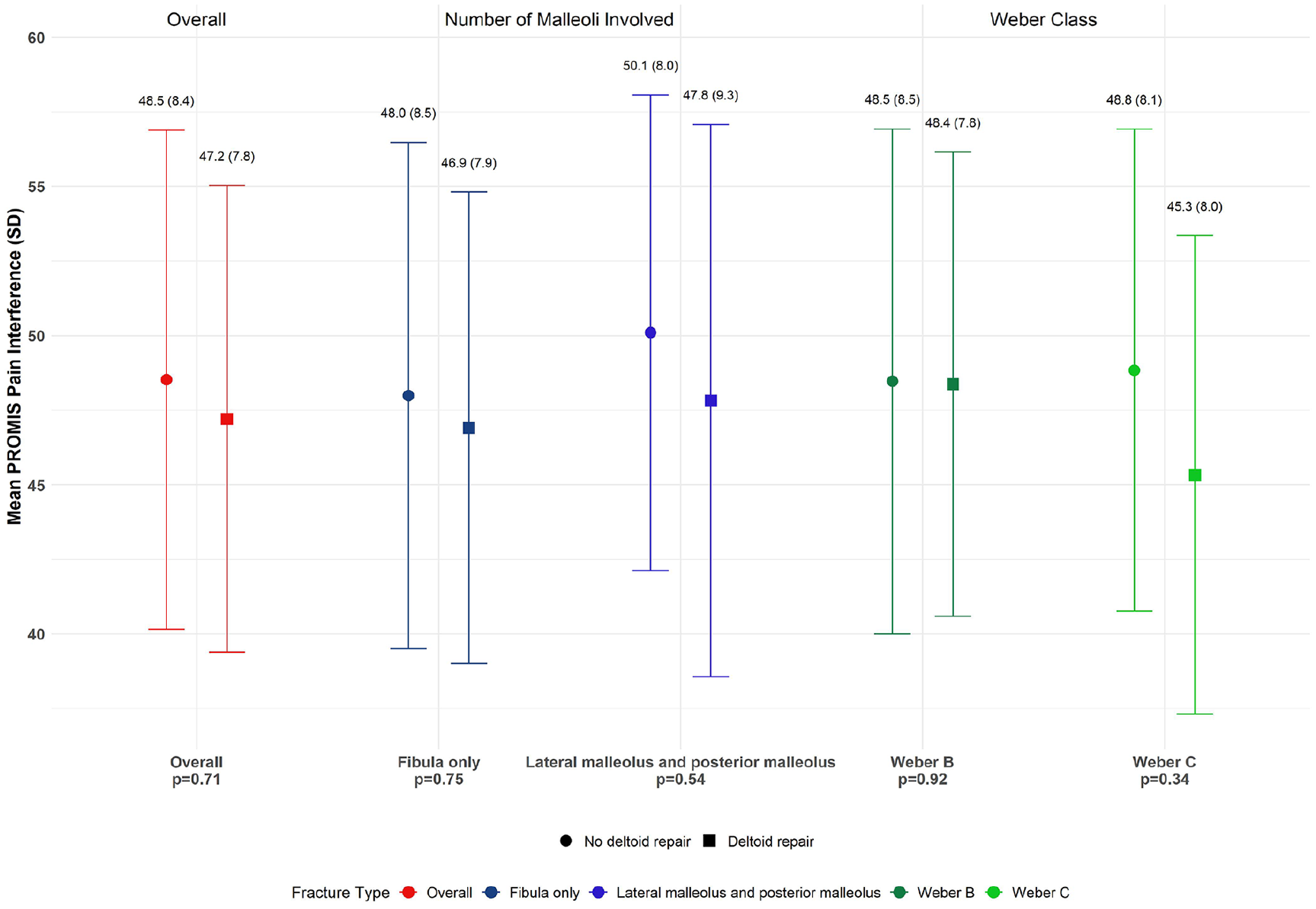
PROMIS pain interference by receipt of deltoid repair. PROMIS, Patient Reported Outcomes Measurement Information System.
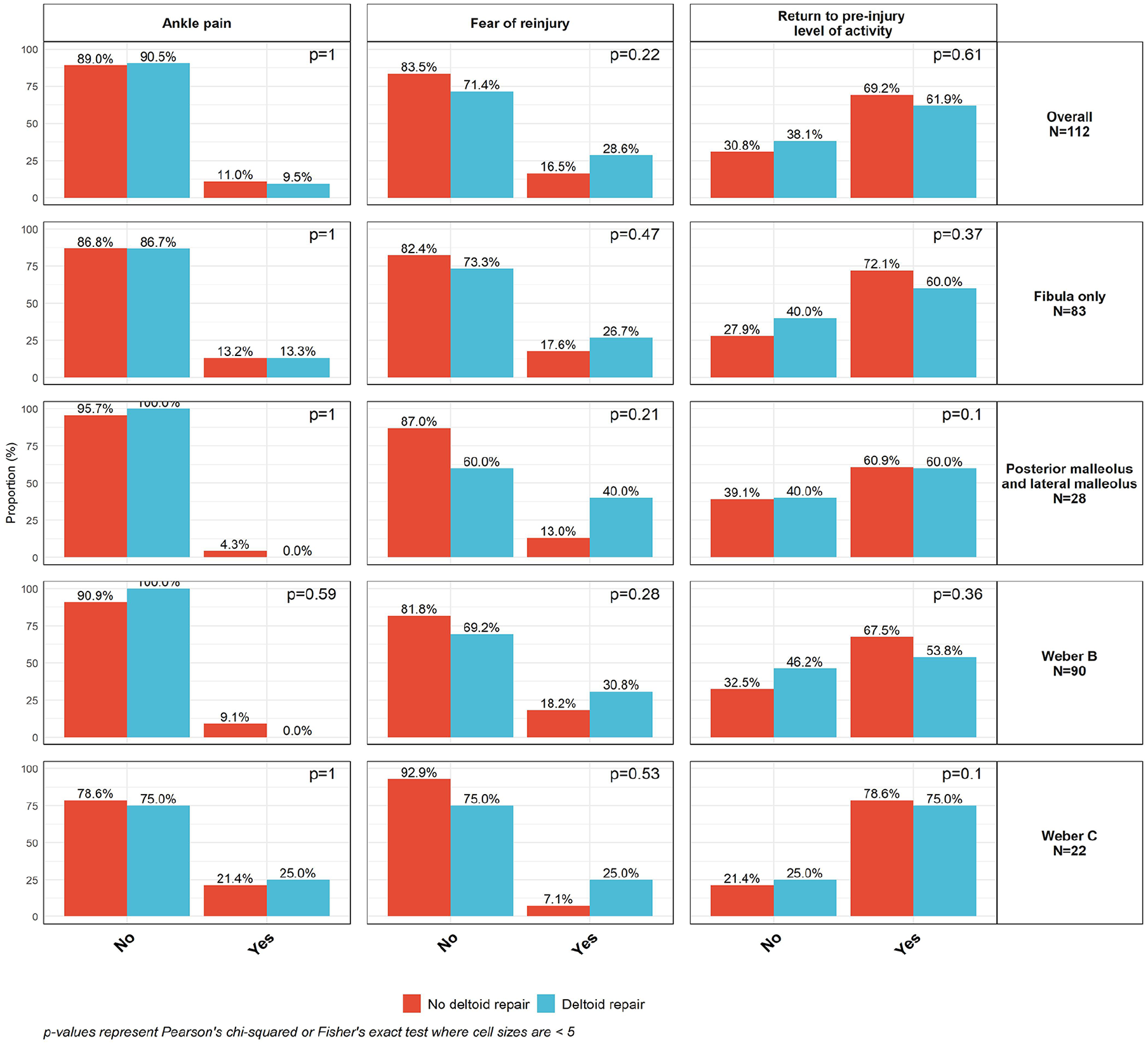
Self-reported ankle pain, return to preinjury level of activity, and fear of reinjury by receipt of deltoid repair.
When analyzing by Weber classification (Figures 1 and 2), scores were similar between DR and NDR patients with WB fractures (n=90). For WC fractures (n=22), DR (n=8) had higher mean PF (58.8±12.1 vs 50.6±7.7, P=.15) and lower mean PI (45.3±8.0 vs 48.8±8.1, P=.34) compared to NDR (n=14).
Twenty-eight of 112 patients had posterior malleolus involvement. Among posterior malleolus fractures fixed intraoperatively (n=16), 13 were NDR and 3 underwent DR. Within this cohort, DR mean PF was 46.93±4.66 and NDR was 46.73±5.48. The mean PI between NDR and DR was similar: DR 53.90±7.74 and NDR 52.65±7.07. In patients with posterior malleolus fracture treated nonoperatively (n=12), DR (n=2) had a PF of 55.40±2.55 and a PI of 38.70±0.00. NDR (n=10) had a PF of 57.49±11.71 and a PI of 46.78±8.19.
Linear regression analysis revealed that DR was associated with a 1.89 higher PF than NDR. The model estimated DR PI 1.67 points lower than that of NDR. When adjusted for propensity scores, DR had PF 2.17 higher and PI 1.73 lower than NDR. (Table 4).
Effect of Deltoid Repair on PROMIS Scores Evaluated with Propensity Score vs Covariate Adjusted Linear Regression. a

Abbreviations: CI, confidence interval; PROMIS, Patient Reported Outcomes Measurement Information System.
Estimate for deltoid repair (reference: did not repair deltoid). Propensity scores for deltoid repair were calculated using logistic regression models adjusted for age, body mass index, syndesmosis rupture, sex, posterior malleolar fracture. Propensity scores (PS) were included as a term in linear regression models, which were additionally adjusted for fear of reinjury.
In the subgroup of isolated fibula fractures, DR resulted in PF 2.28 points higher compared with that of NDR (Table 4). DR resulted in estimated PI 1.04 points lower compared to that of NDR (Table 4). When adjusting for propensity scores, DR had a PF score 2.32 points higher and PI 0.96 lower than NDR.
Fracture subtype, syndesmotic involvement, and posterior malleolus involvement did not significantly impact PROMIS scores in regression models (P > .05) and were adjusted for with propensity scores. FORI, sex, and age had significant effects on PF. FORI and sex had significant effects on PI (see Supplementary Tables). These variables were accounted for in adjusted models.
Median (IQR) clinical follow-up was 45 (37) months in NDR and 29 (25) in DR (P=.06). Median (IQR) radiographic follow-up was 12.0 (4.0) months for DR and 13.5 (6.5) months for NDR (P=.07).
Discussion
Deltoid rupture incidence was 49%, which is consistent with reported rates.16,24,41 DR resulted in no radiographic complications compared to NDR complication rates of 14.42% overall and 11.18% among isolated fibula fractures. Lower complication rates are likely attributed to improved stability and maintained alignment of the ankle after anatomic repair of the deltoid complex.2,27 A cadaveric study found that DR results in improved reduction and stabilization of the tibiotalar joint compared to ORIF of the ankle alone. 2
The present study corroborates literature demonstrating reduced postoperative complications with DR—including notably lower rates of syndesmotic malreduction.23,40,43,44 In a systematic review, Wang et al 40 described that DR significantly reduced the incidence of syndesmotic malreduction compared with NDR (0%-9% vs 20%-35%). Zhao et al 44 similarly revealed a syndesmotic malreduction rate of 0% in DR and 20.4% in NDR. Similarly, prior studies demonstrate that DR results in decreased medial clear space widening, a radiographic indicator of syndesmotic malreduction.10,23,32,42,44 Although our study did not quantify degree of syndesmotic malreduction, no patients who underwent DR in our cohort were diagnosed with postoperative syndesmotic malreduction; conversely, syndesmotic malunion occurred in 1.86% of all NDR patients and 1.24% of all NDR fibula only patients, which suggests DR reduces syndesmotic widening and thus helps restore ankle mortise stability and alignment.
No DR patients developed either DJD or ESA. In contrast, NDR patients had a DJD rate of 3.26% and an ESA rate of 0.47% overall and 3.73% and 0% in isolated fibulas. Only one other study documented that DR decreases the incidence of DJD; Sogbein et al 34 found 15% of patients with DR vs 52% of NDR patients developed posttraumatic ankle arthritis. Although arthritis incidence was higher in this study compared with our study, Sogbein et al only evaluated logsplitter ankle fracture-dislocations. Nevertheless, our results suggest that DR improves alignment of the ankle, which may reduce arthritis incidence. Several studies support that malreduction of the ankle joint—especially syndesmotic malreduction—are crucial risk factors for the development of ankle arthritis.4,17,29,30,39 Therefore, the lower syndesmotic malreduction rates in our study may explain why DR has a 0% incidence of DJD compared with 3.26% incidence of DJD found in NDR (3.73% when only evaluating isolated fibulas). Low DJD rates in our study also could be explained by patients included with only minimum 1-year follow-up, as posttraumatic osteoarthritis may occur at later postoperative time intervals.
Incidence of each postoperative complication, particularly deep wound complications, was similar between groups, which is consistent with prior literature and accentuates the safety of DR. 32
This study was not adequately powered to detect small to moderate effect sizes among PROMIS score differences. Although differences between groups did not meet the MCID range (change of 3-30), larger sample sizes are needed to investigate this comparison.19,28 The DR group exhibited better PROMIS scores compared with NDR patients, although these values did not reach statistical significance. Regression models, especially when adjusting for propensity scores, estimated greater increases in PF and greater decreases in PI for DR compared to NDR. The estimated PF for DR compared with NDR was even higher in both adjusted models for isolated fibula fractures compared with the overall cohort. Therefore, although DR may improve PF in patients regardless of fracture subtype, subgroup analysis of isolated fibula fractures suggests that DR may benefit patient function postoperatively, especially because we postulate that analysis of isolated fibular fractures minimizes confounders. These findings revealing modest improvements in PROMIS scores with DR therefore suggest that DR may improve functional outcomes compared to NDR.
Given that WC fractures typically have higher rates of syndesmotic injury, the effect of DR on syndesmotic reduction may account for the clinically relevant difference in PF between DR and NDR in WC fractures (58.8 vs 50.6). Larger sample sizes may reveal clinically and statistically significant differences that exceed lower-end range of the MCID for WC fractures. 19
Subgroup analysis of posterior malleolus involvement also suggests that DR may improve function, though small sample sizes in our study resulted in lack of statistical power. Regardless, based on model estimates, posterior malleolus involvement did not significantly impact PROMIS.
Because this study was underpowered, we cannot conclude definitively whether DR improves functional outcomes. Although the results suggest DR may result in improved PROMIS scores compared with NDR, larger samples are needed to evaluate whether DR results in clinically and statistically significant improvements in PROMIS.
Regardless of DR status, patients achieved postoperative population mean functional outcomes, irrespective of fracture subtype, syndesmotic involvement, and posterior malleolus involvement, thereby confirming prior research that argues anatomic fixation of ankle fractures enables satisfactory outcomes, resulting in most patients achieving population mean outcomes.7,9,13
Ultimately, our findings support DR due to reduced radiographically evident complication rates. Although our findings suggest that DR may improve functional outcomes, larger sample sizes are needed to determine definitively whether repair improves PROMs.
This study was limited by its retrospective design and small sample of DR patients who responded to surveys. Future investigations require larger samples (we needed 130) and prospective, randomized controlled design. The low rate of survey follow-up (32%) may have introduced selection bias; however, this rate is similar to the response rate reported by the Orthopaedic Foot and Ankle Outcomes Research Network for PROMIS survey. 22 Although patients completed CATs at minimum 1-year follow-up, patients were necessarily at different time points in their recovery on survey completion.
Regardless of these limitations, this study offers crucial insight into the importance of DR in maximizing function for patients who undergo ankle fracture surgery.
Conclusion
DR was associated with reduced radiographically evident complications following ankle fracture surgery. Postoperative complication rates were similar between groups, indicating the safety of DR. This study was underpowered to detect small effect sizes in PROMIS, and we remain uncertain if DR meaningfully improved patient-reported outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251330879 – Supplemental material for Does Deltoid Ligament Repair Reduce Complications and Improve Functional Outcomes Measured by PROMIS Scores Following Ankle Fracture Surgery?
Supplemental material, sj-pdf-1-fao-10.1177_24730114251330879 for Does Deltoid Ligament Repair Reduce Complications and Improve Functional Outcomes Measured by PROMIS Scores Following Ankle Fracture Surgery? by Steven M. Hadley, Rachel Bergman, John J. Peabody, Sarah J. Westvold, Ryan Filler, Milap Patel and Anish R. Kadakia in Foot & Ankle Orthopaedics
Footnotes
Appendix
Unadjusted and Adjusted Effect of Deltoid Repair on PROMIS Physical Function and Pain Interference Scores in Patients with Isolated Fibula Fractures Only.

| PROMIS Physical Function | PROMIS Pain Interference | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | |||||||||
| Estimate | Standardized Coefficient (95% CI) | P Value | Estimate | Standardized Coefficient (95% CI) | P Value | Estimate | Standardized Coefficient (95% CI) | P Value | Estimate | Standardized Coefficient (95% CI) | P Value | |
| Deltoid repair status (reference: no deltoid repair) | .46 | .39 | .65 | .66 | ||||||||
| Deltoid repair | 2.27 | 0.21 (–0.35, 0.77) | 2.28 | 0.21 (–0.27, 0.70) | –1.09 | –0.13 (–0.69, 0.43) | –1.04 | –0.12 (–0.68, 0.44) | ||||
| Syndesmotic involvement (reference: deltoid only) | .96 | .54 | .93 | .42 | ||||||||
| Deltoid + syndesmosis | –0.13 | 0.01 (–0.42, 0.45) | –1.33 | –0.12 (–0.52, 0.27) | 0.17 | 0.02 (–0.41, 0.46) | 1.56 | 0.19 (–0.27, 0.64) | ||||
| Age (continuous) | –0.16 | –0.21 (–0.42, 0.00) | .06 | –0.15 | –0.19 (–0.38, 0.00) | .05 | 0.1 | 0.16 (–0.06, 0.37) | .15 | 0.09 | 0.15 (–0.07, 0.37) | .19 |
| Weber subtype (reference: Weber B) | .19 | .59 | .13 | .29 | ||||||||
| Weber C | 4.13 | 0.39 (–0.18, 0.96) | 1.59 | 0.15 (–0.40, 0.70) | –3.72 | –0.44 (–1.01, 0.12) | –2.89 | –0.35 (–0.98, 0.29) | ||||
| Fear of reinjury (reference: no) | <.001 | <.001 | .01 | .03 | ||||||||
| Yes | –10.89 | –1.03 (–1.53, –0.53) | –9.21 | –0.87 (–1.35, –0.38) | 5.76 | 0.69 (0.16, 1.22) | 5.14 | 0.62 (0.06, 1.17) | ||||
| Sex (reference: female) | <.001 | <.001 | .03 | .21 | ||||||||
| Male | 10.00 | 0.94 (0.56, 1.33) | 7.39 | 0.70 (0.31, 1.08) | –3.92 | –0.47 (–0.89, –0.04) | –2.37 | –0.28 (–0.72, 0.16) | ||||
Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information System.
Ethical Approval
This study received ethical approval from the Northwestern University IRB (STU00218343) on 11/29/2022.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steven M. Hadley, Jr., BA, reports disclosures relevant to manuscript from HydroCision, Inc., consultant. Anish R. Kadakia, MD, reports disclosures relevant to manuscript from Arthrex: consultant, royalties, speakers bureau; DePuy Synthes: royalties; and Elsevier: royalties. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.