
Abstract
Background:
There is a lack of consensus on how deltoid injuries should be addressed in the setting of acute ankle fractures. This study aims to evaluate whether deltoid repair during lateral malleolar fracture fixation leads to improved clinical outcomes compared to fixation without deltoid repair.
Methods:
This was a single-center retrospective study involving 13 surgeons. Inclusion criteria were patients aged 18 years or older who underwent open fixation for a supination external rotation type IV (SER IV) equivalent ankle fracture. SER IV fractures were confirmed with stress radiographs. Deltoid injury was confirmed with an intraoperative external rotation stress test. A total of 146 patients were included. Eighty patients received a deltoid repair (DR), and 66 patients did not receive a deltoid repair (NDR). Patient-reported outcomes via PROMIS scores were collected preoperatively and at least 1 year postoperatively for all patients. Preoperative and postoperative medial clear space (MCS) were reviewed for all patients.
Results:
There were no significant differences in preoperative and postoperative PROMIS domains between the 2 cohorts. There were also no significant differences in preoperative MCS and postoperative MCS between the 2 cohorts. There were no significant differences in the incidence of subsequent procedures for removal of painful hardware, revisions, infections, progression to arthritis, and persistent pain.
Conclusion:
This study compares short- to medium-term outcomes and complications of SER IV–equivalent ankle fractures with and without deltoid repair. No significant differences between PROMIS scores, postoperative MCS, and complication rates were observed between groups.
Level of Evidence:
Level III, retrospective case control study.
Introduction
Lateral malleolar ankle fractures often present with concomitant injury to the deltoid ligament, occurring in up to 40% of cases as revealed by arthroscopic examination.1,12 The deltoid ligament is divided into 2 layers. The superficial layer consists of the tibionavicular, tibiocalcaneal, superficial posterior tibiotalar, and tibiospring ligaments and functions primarily to resist external rotation and valgus stress. The superficial layer contributes minimally to ankle stability. The deep layer consists of the deep posterior tibiotalar ligament and the deep anterior tibiotalar ligament and integrates with the joint capsule of the tibiotalar joint and attaches to the medial aspect of the talus. The deep layer is crucial in preventing excessive lateral movement of the talus and serves as the principal restraint against rotational stress on the talus.
Therefore, rupture of the deltoid ligament, with subsequent retraction and healing outside of its anatomical position, could disrupt the biomechanics of the medial ankle, leading to increased instability as it allows for anterior and lateral translation of the talus out of the mortise. Lateral malleolar ankle fractures where the deltoid ligament ruptures but the medial malleolus remains intact are referred to as “bimalleolar equivalent” ankle fractures.1,12 In these cases, loss of deltoid integrity allows the talus to sublux laterally, rendering the ankle functionally unstable.
As a result of this instability, bimalleolar equivalent ankle fractures often require surgical intervention, typically with open reduction and internal fixation (ORIF) of the fibula, and occasional fixation of the syndesmosis in cases with residual instability of the mortise.1,12 However, there is no clear consensus on whether or not fixation of the deltoid is warranted in these cases. Many physicians believe that repairing the deltoid ligament is not necessary if internal fixation of the fibula alone is enough to achieve reduction of the talus within the ankle mortise.1,2,12,13,15,17 Proponents against fixation of the deltoid cite concerns of increased postoperative complications as a result of longer operative time and the potential for medial-sided infection. A medial clear space (MCS) of >4 mm on stress radiographs is considered to be a diagnostic hallmark for deltoid rupture 3 and has been found to be a reliable predictor of deep deltoid injury. 6 In Maynou et al’s 8 study on bimalleolar ankle fractures, they report that deltoid ligament injuries should be repaired only if there is a medial incongruence of greater than 3 mm on intraoperative radiographs.
However, it is also believed that the presence of positive intraoperative stress tests despite ORIF and syndesmotic fixation predisposes patients with ankle fractures to instability even after fixation. 4 In Johnson and Hill’s 3 study of 30 patients who underwent ORIF of the fibula without repair of the deltoid for treatment of bimalleolar equivalent fractures, 41% of patients experienced poor functional and symptomatic outcomes at the 15-month follow-up, and in 34% of patients, it was determined that their symptoms were a consequence of chronic overuse of the attenuated deltoid ligament as opposed to ankle instability. Similarly, in Zhao et al’s 18 study of the same nature, they found similar results with patients receiving repair of the deltoid, showing superior results with significantly lower malreduction rates compared to patients not receiving repair of the deltoid. Furthermore, many authors report significant reductions in MCS following deltoid repair.4,11,18 Of note, however, the indications for deltoid repair in these studies were determined by set preoperative MCS criteria.
In this study, we aim to compare the clinical and radiographic outcomes of supination external rotation type IV (SER IV) fibular fractures with and without deltoid repair. Our primary indication for repairing the deltoid was presence of a positive intraoperative stress test, indicating medial instability, rather than the degree of MCS widening observed on preoperative radiographs. We hypothesize that patients in both treatment groups will have similar clinical and radiographic outcomes and postoperative complication rates.
Methods
This was a single-center retrospective study conducted from the institutional review board–approved Foot and Ankle Registry data, and the protocol was approved by the steering committee at the investigators’ institution. Cases from 13 surgeons performed between 2016 and 2022 were identified and reviewed. Inclusion criteria included patients aged 18 years or older who underwent open fixation for a SER IV fibular fracture with a deltoid injury and had preoperative PROMIS scores. To accurately differentiate between stable SER II and unstable SER IV–equivalent fractures where the distinction was not clear on plain film radiographs, stress radiographs were used. Excluded were patients with syndesmotic disruption identified by significant widening in the tibiofibular joint space during intraoperative external rotation stress testing, patients with open fractures, patients without preoperative radiographs, and patients with histories of previous ipsilateral ankle surgeries, rheumatoid arthritis, or gout. Retrospective review of the registry was performed, and 368 patients were identified. Chart notes were reviewed to ensure eligibility, and 144 patients qualified for inclusion. Seventy-eight patients received a deltoid repair (DR), and 66 patients did not receive a deltoid repair (NDR). Treatment algorithm was based entirely on surgeon preference. In all patients, deltoid repair was performed after the fibular ORIF. Preoperative and postoperative medial clear space (MCS) were reviewed for all patients by the senior author. Patient-reported outcomes via PROMIS scores were collected preoperatively and at least 1 year postoperatively for all patients.
Surgical Procedure
Given that there were 13 surgeons included in this patient cohort, there may have been some variability in the repair approach. However, all surgeons followed the treatment algorithm as follows, barring the decision to repair the deltoid based on surgeon preference. First, the lateral malleolar fractures were treated with ORIF with plate and screws. After fracture fixation, intraoperative external rotation stress test was performed routinely in all patients to assess for ligament instability. If indicated, attention was then turned to repair of the deltoid. Our primary indication for operative repair of the deltoid was positive intraoperative stress test, indicating persistent medial instability despite fibular fixation and/or evidence of lateral talar subluxation, which suggests complete rupture of the deltoid complex after fibular fixation..
The following is a more detailed description of surgical technique of one of the authors’ approach to repairing the deltoid: A longitudinal incision of approximately 3 cm is made at the central aspect of the medial malleolus. Caution should be taken to protect the saphenous nerve and veins. Subsequently, the posterior tibial tendon sheath is incised longitudinally to facilitate posterior retraction of the tibialis posterior tendon, enhancing visualization of the deltoid ligament complex. An anteromedial capsulotomy is then performed along the anterior border of the superficial deltoid layer, enabling assessment of deltoid ligament injury, identification of osteochondral injuries within the medial gutter, joint reduction, and detection of loose bodies.
Following deltoid ligament injury identification, a deeper surgical approach is initiated. Loose bodies and tissue in the medial gutter that could preclude anterior reduction are debrided after adequate exposure, with caution to delineate the deltoid ligament beforehand to prevent inadvertent damage.
A suture anchor is then inserted into the tibia at the deep deltoid ligament’s tibial origin, typically aligned with the talar body’s center when viewed from a true lateral fluoroscopic image with the ankle in near-neutral dorsiflexion (Figure 1, A and B). Subsequently, if reconstruction is warranted, the ligament is detached from the medial malleolus and sutured using a Brostrom-type advancement technique. In most cases, the origin of the deltoid on the medial malleolus is bald as a result of rupture, negating the need of surgical detachment.
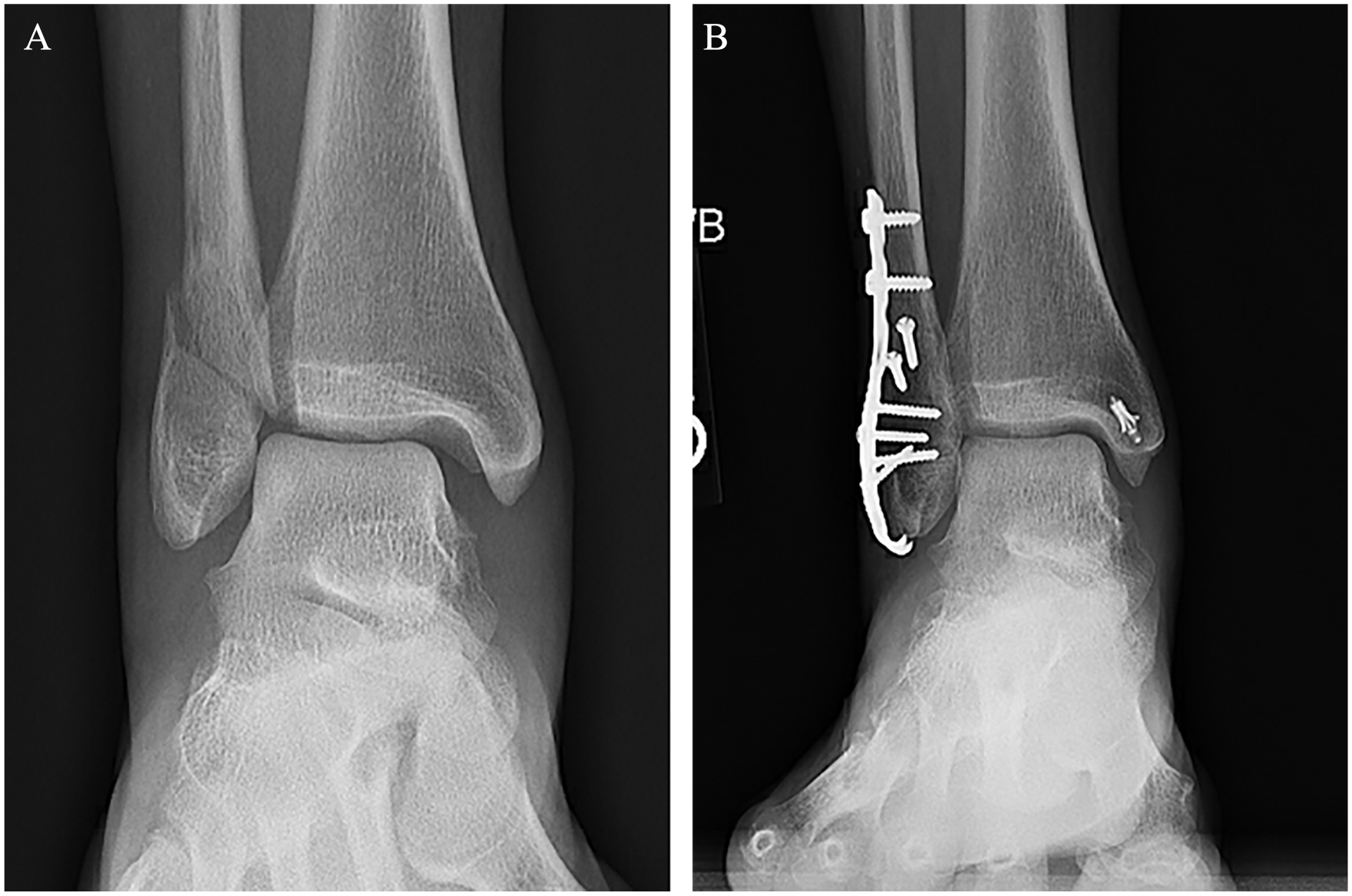
(A) A 40-year-old patient presented with a SER IV lateral ankle fracture and deltoid injury. (B) Fibular fixation with deltoid repair demonstrated satisfactory ankle joint alignment without acute osseous complication at 6 months postoperation.
Ankle mortise reduction is achieved with the ankle in neutral dorsiflexion and mild inversion. In cases where the deltoid injury is at the medial malleolar origin or midsubstance, 1 or 2 suture anchors are passed through the intercollicular groove in an extraosseous manner and secured around the medial malleolar periosteum. Fluoroscopic and direct visualization via the anteromedial capsulotomy are employed to confirm anatomical ankle reduction. Subsequently, the suture limbs, now affixed to the medial malleolar post, are arranged in a fanlike pattern and integrated into the deltoid ligament, encompassing both superficial and deep components, and approximated to the medial malleolus.
In the rare scenario of deltoid disruption near its talar insertion, a single anchor is used to reattach the deep deltoid using a horizontal mattress technique. Optimal alignment is achieved initially with an anchor, followed by passage of sutures through the intercollicular groove and tying over the post.
On completion of repair, the tibialis posterior tendon is returned to its sheath and secured with 2 interrupted 2-0 absorbable sutures to prevent tendon subluxation.
Statistical Analysis
Descriptive statistics were reported as means and SDs for continuous variables and counts and percentages for categorical variables. An a priori power analysis found that a minimum of 24 patients for each cohort was needed to achieve 80% power, given a minimum detectable difference on the PROMIS physical function scale of 5.8 points and an SD of 8 points. These values were taken from previous literature on clinically important differences in foot and ankle patients for PROMIS scores. Listwise deletion was conducted for patients with missing data. Differences in postoperative outcomes between the deltoid-repaired and the non–deltoid repaired groups were assessed with sample t tests. Correlation between postoperative MCS and postoperative clinical outcomes was assessed with linear regression analysis. Alpha of .05 was established as statistically significant for this study. The analysis was conducted on R: A language and Environment for Statistical Computing (R Core Team 2021, Vienna, Austria).
Results
Demographics
In total, 144 patients were eligible for inclusion. Seventy-eight were treated with deltoid repair (DR) plus ORIF of the fibula while the remaining 66 were treated with ORIF of the fibula alone (NDR). Demographic comparisons are shown in Table 1. No significant differences were noted between each group.
Demographic summaries between DR and NDR cohorts.

Abbreviations: DR, deltoid repair group; NDR, non–deltoid repair group.
No significant differences were noted between age, sex, BMI, and time from injury to surgery. (Significance was noted at a P value <.05.)
Clinical and Radiographic Outcomes
Preoperative and postoperative radiographic outcomes, as determined by medial clear space (MCS) widening, were available for all 144 patients included in the study. Average preoperative MCS for the DR group was 5.47 mm (range: 2.00-14.20 mm, SD = 2.6) compared with 4.77 mm (range: 2.00-14.80 mm, SD = 2.3) for the NDR group (P = .12) (Figure 2). Average postoperative MCS for the DR group was 2.98 mm (range: 1.30-6.30 mm, SD = 0.8) compared to 2.91 mm (range: 1.40-4.00 mm, SD = 0.6) for the NDR group (P = .56). Both groups showed significant reduction in final postoperative MCS (P < .05). Linear regression analysis showed that the final follow-up MCS did not show any significant influence on postoperative PROMIS outcomes (physical function, P > .69, r = 0.04; pain interference, P > .15, r = −0.14; pain intensity, P > .25, r = −0.12; global physical health, P > .92, r = 0.01; global mental health, P > .21, r = −0.1; depression, P > .41, r = −0.08).

Comparison of preoperative and postoperative MCS widening based on deltoid repair. No significant differences in MCS were observed between study groups. However, both groups demonstrated significant reduction in MCS before and after fixation.
Forty-four preoperative PROMIS scores were available for the NDR group, and 51 were available for the DR group. Fifty postoperative PROMIS scores were available for the NDR group with an average follow-up of 3.38 (range, 1-7.59) years compared with 54 for the DR group with an average follow-up of 2.82 (range, 1-7.07) years. Both DR and NDR cohorts demonstrated significant improvement in all PROMIS domains except for Global Mental Health. No significant differences were noted in preoperative and postoperative PROMIS domains between the 2 cohorts. PROMIS outcomes are shown in Table 2.
Comparison of Postoperative PROMIS Scores Between DR and NDR groups.

Abbreviations: DR, deltoid repair group; NDR, non–deltoid repair group.
At a final follow-up of 3.04 (range, 1.02-7.59) years, no significant differences were observed between the DR and NDR groups. (Significance was noted at a P value <.05.).
Complications
The overall complication rate for the DR group was 10%, with 8 patients requiring return to the OR, 2 for postoperative infection, and 6 for removal of hardware. Of the 2 patients experiencing postoperative infection, 1 had a medial incision and the other had a lateral incision. No nerve complications were observed in the DR group. The total complication rate for the NDR group was 7.7%, with 5 patients requiring return to the OR for removal of hardware and one of those 5 patients also experiencing a postoperative infection for a total of 6 complications. There were no significant differences noted between complication rates nor the incidence of subsequent procedures for both groups (P = .79). In addition, no revisions nor postoperative malalignments were observed in either cohort.
Discussion
Early research initially suggested that exploring the medial ankle and repairing the deltoid ligament might not offer significant benefits over managing it conservatively as both approaches showed similar clinical outcomes in terms of range of motion, length of hospital stay, and symptoms.14,16 However, subsequent studies have challenged that notion, indicating that leaving the deltoid ligament unrepaired could lead to persistent pain or deformities related to pronation, as well as inferior clinical and radiographic outcomes as evidenced by increased postoperative MCS and malreduction rates.4,5,7 –9,11
Recent studies have highlighted potential advantages of surgically repairing the deltoid ligament, such as improved restoration of the MCS postoperatively for a specific injury pattern. For instance, Sogbein et al1,12 observed significant reductions in medial clear space and tibiofibular clear space in patients who underwent deltoid ligament repair following bimalleolar ankle fractures. Similarly, studies by Little et al 6 and Wu et al 16 reported lower rates of syndesmotic malreduction and decreased need for secondary surgeries in patients who received deltoid ligament repair along with fibular fixation.
Our current study did not find any significant differences in postoperative clinical outcomes between the DR and NDR groups. Nor did we report any significant differences in postoperative MCS between the groups. Of our 78 patients treated with deltoid repair, 21 (26.9%) had a preoperative MCS <4 mm. However, our decision to repair the deltoid was due to the presence of positive intraoperative external rotation stress tests in these patients, indicating persistent medial instability despite fibular fixation. Of note, patients were manually reduced before operation, which may have resulted in our lower reported findings of MCS (2 mm lower limits in both DR and NDR groups). However, in cases where the MCS was below the 5-mm cutoff, deltoid injury was confirmed intraoperatively via the external rotation stress test and noted in the operative notes.
Additionally, recent studies indicate that the deltoid ligament is an indirect stabilizer of the syndesmosis. 10 Many of the studies cited in the literature showing significantly inferior outcomes in patients not receiving deltoid repair for bimalleolar equivalent ankle fractures4,6,10,11 used MCS measurements as their primary indication for repair. These results lead us to believe that MCS >4 mm may not alone be an adequate indication for deltoid repair and that other factors, such as degree of medial instability as assessed by the external rotation test, may be necessary to get a better indication of whether the patient would benefit from deltoid repair. In Salameh et al’s 10 systematic review on deltoid ligament repair in ankle fracture, the authors support the idea that repair of the deltoid may be beneficial in patients with residual valgus instability following ORIF of the fibula in bimalleolar equivalent ankle fractures. However, to our knowledge, there have been no studies using valgus instability following ORIF as one of the primary indicators for deltoid repair. In addition, valgus instability may be indicative of a pronation external rotation as opposed to an SER fracture. Thus, further research is warranted.
This study faced several limitations that should be considered when interpreting the results. First, the retrospective nature of the study may introduce biases related to selection and data collection, potentially affecting the validity of the outcomes. Although our sample size of 144 patients provides a substantial basis for analysis, it may still limit the statistical power to detect subtle differences in clinical and radiographic outcomes between the DR and NDR groups. A larger sample size could perhaps provide us with greater statistical power to perform subgroup analyses defined by preoperative MCS measurements within each group. Additionally, variations in the surgical techniques employed by 13 different surgeons could introduce inconsistencies in treatment protocols and outcomes. The reliance on subjective clinical assessments and radiographic interpretations also poses a risk of variability and measurement error. Finally, the follow-up duration, although set at a minimum of 1 year postoperatively and adequate for assessing early outcomes, may not capture long-term complications or functional performance, suggesting the need for further studies with longer follow-up periods to fully evaluate the implications of deltoid repair in this patient population.
Conclusion
Our study demonstrated similar radiographic and clinical postoperative outcomes with short- to medium-term follow-up between SER IV ankle fractures with deltoid injury treated with and without ankle repair. Consistent with much of the recent literature advocating for repair of the deltoid in the setting of bimalleolar equivalent ankle fractures, our study did not report any significant differences in complication rates. The decision to repair the deltoid ligament involves weighing these potential benefits against the risks such as increased surgical complexity, longer operative times, and injury to nearby nerves and blood vessels, and the potential for overtightening medial ligamentous structures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251329333 – Supplemental material for Comparison of Clinical and Radiographic Outcomes of Supination External Rotation Type IV Equivalent Ankle Fractures With and Without Deltoid Repair
Supplemental material, sj-pdf-1-fao-10.1177_24730114251329333 for Comparison of Clinical and Radiographic Outcomes of Supination External Rotation Type IV Equivalent Ankle Fractures With and Without Deltoid Repair by Saanchi Kukadia, David Cho, Stephanie Eble, Prashanth Kumar, Alan Shamrock and Mark Drakos in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval to pursue this study was granted by our institution’s Foot and Ankle steering committee.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mark Drakos, MD, is an extremity consultant for Arthrex. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.