
Abstract
Background:
Female representation among residents and practicing surgeons in orthopaedics remains disproportionately low at 19.3% and 7.4%, respectively. This study investigates female representation in speaker roles at American Orthopaedic Foot & Ankle Society (AOFAS) meetings over time.
Methods:
The annual AOFAS meeting programs for 2012 to 2024 were reviewed by 3 independent raters. Each speaker, moderator, and panelist was classified based on gender and role; data were cross-checked using Fleiss multirater κ validation. Sessions discussing surgical or biomedical topics were categorized as “technical,” and all other sessions were categorized as “nontechnical.” Yearly odds ratios (ORs) and CIs evaluating gender vs session status, as well as gender vs speaker role, are provided.
Results:
A total of 2396 speaking sessions were analyzed; 11.5% of sessions were led by female speakers. Over time, female speaker representation ranged from 5.61% in 2014 to 18.75% in 2022. Female speakers led only 10.8% of the 2088 technical sessions. On average, female speakers were significantly more likely than males to assume nontechnical speaking roles across all years combined (OR 1.5111, 95% CI 1.0792-2.1158, P = .0162). For individual year ORs, female speakers were significantly more likely to assume nontechnical speaking roles in 2020 (OR 12.24, 95% CI 4.082-36.67, P < .001); however, the differences were not statistically significant for other years. Females also comprised 10.10% and 12.00% of moderator and panelist roles, respectively.
Conclusion:
Female speaker involvement was representative of AOFAS female membership and the national population of female orthopaedic surgeons. Additionally, our study revealed an increasing trend in female speakers, panelists, and moderators from 2012 to 2024. However, there is a need for a shift in the distribution of speaker roles to prevent professional marginalization. Continued efforts to support female representation as role models at national conferences increases visibility and may help to address the lack of women within orthopaedics.
Level of Evidence:
Level III, retrospective cross-sectional study.
Introduction
Although female students comprise 58% of undergraduate enrollment 25 and 54% of medical students in the United States, 37 their representation in orthopaedic surgery is disproportionately low. Only 19.3% of orthopaedic surgery residents, 40 approximately 14% of American Academy of Orthopaedic Surgery fellows, 24 and 7.4% of practicing orthopaedic surgeons are female, 28 according to statistics from 2021 to 2023 (Figure 1). 23 Notably, a recent study found that match rates of female candidates are reflective of their application rates. 40 These data suggest that there is a barrier preventing female medical students from applying to orthopaedic surgery residencies. Addressing this disparity necessitates a detailed examination into the underlying factors that contribute to the lack of female representation and the efficacy of interventions aimed at supporting women to pursue a career in orthopaedics.

Female representation at different levels of orthopaedic surgery training. Data demonstrate latest reported statistics, with the year reported in parentheses from 2021 to 2023.
Diversity is a critical component of team dynamics that benefits organizations at all levels. 33 Supporting a diverse workforce has been shown to foster creativity and innovation, leading to improved outcomes across metrics, from financial performance to patient care.1,5,18,19,35,39 Within medicine, recruiting a health care team that reflects the patient population improves patient access, perceptions of care quality, and health outcomes.3,7,13,22,31
Multiple social science studies have outlined that 30% representation within a population establishes a critical mass threshold at which a minority population becomes incorporated and represented in the institutional culture.16,21,38 Given that 7.4% of practicing orthopaedic surgeons are female, 28 reaching this threshold would require years to achieve without active awareness and effort to improve sex and gender diversity. 38 Foot and ankle surgery is an orthopaedic subspeciality with one of the highest rates of female surgeons, with 14.4% of American Orthopaedic Foot & Ankle Society (AOFAS) members being female in 2023 and 15.2% in 2024, respectively (Table 1).6,29 Thus, the goal of this study was to examine the representation of female orthopaedic surgeons at the AOFAS Annual Meetings over time. We hypothesized a trend of increased female representation over the past 12 years, and that the proportion of female participants across session categories and speaker roles would be proportional to the rate of female society membership.
American Orthopaedic Foot & Ankle Society Membership Information. a

The overall 12-year trend demonstrates increasing female membership; however, female members remain a minority within the society. This information was collected from the American Orthopaedic Foot & Ankle Society.
Methods
The study analyzed 3 measures: the proportion of female speakers over time, the distribution of technical and nontechnical sessions by gender, and the gender distribution of moderators and panelists. Annual meeting programs and AOFAS membership data for the years 2012, 2017, and 2022 were obtained from society leadership as well as recent literature. 6 These years were selected to represent a temporal cross-section of a 10-year span, providing insight into trends of female representation in these professional forums.
Gender Classification of Conference Speakers
In this study, the term gender is used primarily in reference to the roles and identities that individuals occupy, recognizing that it may not always align with biological sex. The reviewers used a recognized approach to categorize the gender of every speaker, using practices that have been implemented in prior research to assign gender based on speaker name.26,30 If the speaker's name was unclear, neutral, or not an English name, the reviewers used online profiles to determine gender. 2
Session Categorization
Sessions within the conference programs were categorized into 2 distinct types: “technical” and “nontechnical.” Technical sessions included those discussing surgical technique, biomedical science, basic science, or clinical research topics. Nontechnical sessions encompassed all other sessions, such as welcome sessions, keynote addresses, disparities research, social drivers of health, or medical education topics. 26
Statistical Methods
Interrater reliability for gender classification was assessed using Fleiss multirater κ, 14 where 20 data points were cross-checked among all 3 raters. Given an expected agreement rate above 80%, an acceptable sample size was determined based on prior statistical recommendations. 10 Once interrater reliability was confirmed, each reviewer completed data collection for their assigned years. Any discrepancies were resolved through group consensus.
This statistical measure was used to quantify the level of agreement among the 3 raters and to validate the consistency of the classification process. To evaluate changes in female representation over time, odds ratios (ORs) and 95% CIs were calculated for each year, examining the association between sex and session type (technical vs nontechnical) as well as sex and speaker role (moderator vs panelist). When zero females were present in a category, the Haldane-Anscombe correction was applied to ensure stable OR estimation.
A χ2 test for independence was conducted to compare the proportion of female speakers at the annual meeting with the overall proportion of female AOFAS members in the corresponding years.
Regarding temoral changes, a logistic regression model was used to analyze trends in female representation over time, with speaker sex as the dependent variable and year (continuous), session type, and speaker role as independent variables. ORs with 95% CIs were reported to quantify the likelihood of female participation across these categories.
A Cochran-Mantel-Haenszel (CMH) test was also conducted to obtain a pooled OR across years while stratifying by year to control for temporal variability in female representation. Year was treated as a nominal (categorical) variable in this analysis, and pairwise comparisons between years were not performed.
All statistical analyses were conducted using JMP Pro (SAS Institute, Cary, NC), with statistical significance defined as P < .05.
Results
Speaker Representation
Interrater reliability of speaker sex classification was 0.982, demonstrating excellent agreement between raters. 10
The AOFAS annual meeting programs for the years 2012-2024 included a total of 2396 speaking sessions. Of these, 11.5% (n = 276) were led by female speakers, and 88.5% (n = 2120) were led by male speakers (Table 2). Across the 13 years, female representation at the AOFAS annual meeting significantly increased over time. Logistic regression analysis demonstrated that the odds of a presenter being female increased by approximately 8.97% per year (OR 1.0897, 95% CI 1.0506-1.1302, P < .0001), indicating a meaningful upward trend in female participation (Figure 2).
Descriptive Statistics of Female and Male Positions by Session Type and Role Over Time.


Female vs male speaker representation across AOFAS meetings. There is an increasing trend in female speakers, panelists, and moderators from 2012 to 2024; however, female representation remains low.
A χ2 test comparing female AOFAS membership to female meeting speakers was conducted to evaluate whether female participation at the annual meeting was reflective of overall AOFAS membership trends. There was no statistically significant difference (χ2 = 0.000, P = .9628), indicating that female representation among meeting speakers was proportional and nearly identical to their overall membership numbers.
A Cochran-Mantel-Haenszel (CMH) test was also conducted to obtain a pooled OR across years while stratifying by year to control for temporal variability. The results of the CMH analysis were consistent with the logistic regression findings (CMH OR 1.643, 95% CI 1.18-2.287, P = .02), further validating the observed associations between gender and session type.
Technical Session Involvement
Across all sessions, there were a total of 2088 technical and 308 nontechnical sessions. Female speakers led 10.8% (n = 225), and male speakers led 89.2% (n = 1863) of the total technical sessions, compared with 16.6% (n = 51) and 83.4% (n = 257) of nontechnical sessions by females and males, respectively. Females were significantly more likely than males to be assigned to nontechnical sessions compared with technical sessions (OR 1.5111, 95% CI 1.0792-2.1158, P = .0162), indicating potential gender disparities in session type distribution (Figure 3).

Odds ratios for female vs male representation across speaker roles. Female speakers are significantly more likely to be assigned nontechnical speaking roles.
To further assess trends across individual years, ORs for female vs male representation were calculated separately for each year. These yearly ORs varied, with certain years showing higher or lower female participation in specific roles. Notably, the odds of female representation in nontechnical vs technical roles were significantly higher in 2020 (OR 12.24, 95% CI 4.082-36.67, P < .001), while in other years, the differences were smaller and not statistically significant (Figure 4).
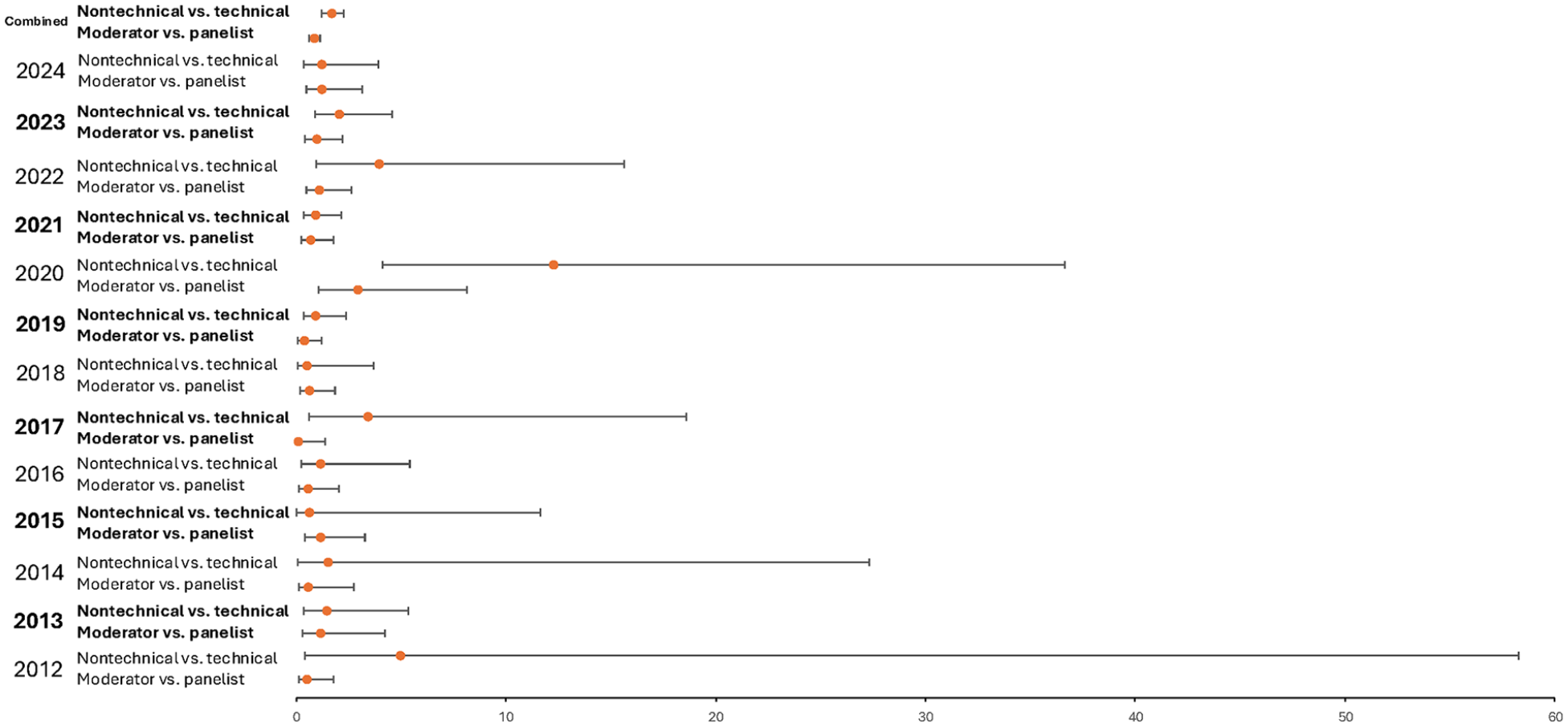
Odds ratios for female vs male representation across speaker responsibility status. Female speakers are significantly more likely to hold a nontechnical speaking role.
Leadership and Moderator Roles
A total of 605 moderators and 1791 panelists were analyzed in AOFAS sessions across all years. Females constituted 10.1% (n = 61) of moderators. Greater female representation was demonstrated in panelist roles, with 12.0% (n = 215) female panelists in all sessions. When analyzing speaker roles, no significant difference was observed between males and females regarding being assigned as a moderator vs a panelist (OR 1.2313, P = .179), suggesting equitable representation across these roles across the 13-year time frame (Figure 3). Looking at individual years, there was no significant difference in OR for female speakers holding moderator roles vs panelist roles, except for 2020 (2.93, 95% CI 1.06-8.15, P < .04) (Figure 4).
Discussion
Over the span of 13 years (2012-2024), our analysis of the AOFAS Annual Meetings revealed a gradual increase in female participation across various roles, with female speakers rising from less than 10% in 2012 to approximately 17% in 2024. Reassuringly, the AOFAS is demonstrating its commitment to female visibility by fairly representing female speakers as we saw no significant underrepresentation in female speaker opportunities compared with AOFAS female membership. Collectively, these findings indicate that although female participation has increased over time, disparities remain in the types of sessions where female speakers are represented. The discrepancy between the logistic regression and χ2 test results highlights the need for a nuanced interpretation of representation metrics, as female membership and speaker participation appear proportionate, yet disparities persist in session type assignments. Furthermore, the variation in yearly ORs suggests that certain years, such as 2020, may have had unique factors contributing to higher female representation in nontechnical roles, warranting further investigation into conference structure and selection processes during those years. These findings highlight both progress and ongoing barriers in high-visibility roles at AOFAS.
Our findings align with broader patterns in orthopaedic surgery, where women comprise a small proportion of high-visibility roles at major conferences. A decade-long study of American Academy of Orthopaedic Surgeons (AAOS) meetings found that although women speakers were proportional to membership, they were significantly more likely than men to be in nontechnical speaking roles (OR 3.85, 95% CI 2.79-4.78). 26 Similarly, a 2018 cross-sectional study of 17 orthopaedic society meetings revealed proportional representation of women, yet women were significantly more likely to lead nontechnical sessions (OR 4.2, 95% CI 2.7-6.5; P < .001) 12 across all society meetings. Our data from AOFAS further support these findings showing that females were significantly more likely to occupy nontechnical speaking roles. This trend highlights a persistent gender imbalance in roles that carry professional prestige and visibility, reinforcing broader systemic challenges. Visibility in high prestige speaking roles is essential not only for advancing individual careers, but also for providing mentorship and role models, which are crucial for addressing the leaky pipeline of women in orthopaedics.
Within the foot and ankle community, the rise in female representation at AOFAS meetings reflects trends across other specialties but still lags behind the growing proportion of women entering the medical profession. The dominance of male speakers parallels the broader field of orthopaedic surgery, where only 6% of practicing orthopaedic surgeons are female, compared with 37% of total physicians. 2 Although AOFAS meetings show greater female representation relative to the field’s demographics, achieving parity in technical and leadership roles requires continued, targeted efforts to support a more inclusive environment in orthopaedic surgery.
Access to role models and mentorship is an important factor in addressing gender disparities.34,36 Research has shown that exposure to role models is strongly associated with medical students' choice of specialty, with 90% of medical graduates reporting that mentors shaped their professional attitudes and career aspirations.27,41 Furthermore, data from the Ruth Jackson Orthopaedic Society (RJOS) show that about 57% of practicing female orthopaedists work in a hospital, medical center or academic practice, suggesting they interact with resident, fellows, and students, thus serving as potential role models. 11 Initiatives such as RJOS, Nth Dimensions, and the Perry Initiative offer programing and mentorship opportunities for female trainees at various stages of their careers in orthopaedics, starting as early as high school.8,15 These programs demonstrably improved female match rates into orthopaedic residencies. 16
Increasing female visibility in prestigious speaking roles and leadership positions is a complementary approach to mentorship programs. Speaking and serving as a moderator at conferences not only establishes an individual as an expert in their field, but also increases their networking and career advancement opportunities. 20 Expanding female representation in these roles has great potential for modeling success to future generations of medical professionals, potentially addressing the leaky pipeline in the field.4,9
There are several limitations to this study that must be considered. First, gender was used as a proxy for sex, inferred from the names of conference participants listed in the AOFAS meeting programs. This approach, which assumes that names correlate with gender, is widely used in research where direct gender identification is not feasible.17,32 However, we recognize that gender may not always align with an individual's sex as assigned at birth, and this method may introduce classification bias despite the high interrater reliability achieved in our study. Second, while categorizing sessions as technical and nontechnical follows prior literature, it remains a somewhat subjective process and may vary in interpretation. Lastly, there are substantial differences in sample sizes between categories, which could influence the power and generalizability of the findings.
Conclusion
Our study revealed that overall female speaker involvement at AOFAS Annual Meetings was representative of female membership in the society over the past decade. It also demonstrated a gradual increase in female representation in speaking, panelist, and moderator roles. However, disparities remain, particularly in technical sessions. Visibility in these roles is essential for career development, mentorship, and establishing credibility. The ongoing gender imbalance may limit opportunities for women to fully participate and progress in the field.
Achieving gender parity will require sustained efforts to cultivate an environment that actively supports female involvement across all levels of orthopaedic surgery. Initiatives such as equitable speaker selection practices, implicit bias training for selection committees, and expanding mentorship programs can support this goal. As the field evolves, AOFAS and other societies should continue to ensure women are represented in influential positions across all levels, helping to inspire and retain the next generation of female orthopaedic surgeons.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251328691 – Supplemental material for Breaking the Glass Ceiling: Female Speaker Representation at the American Orthopaedic Foot & Ankle Society Annual Meetings Over Time
Supplemental material, sj-pdf-1-fao-10.1177_24730114251328691 for Breaking the Glass Ceiling: Female Speaker Representation at the American Orthopaedic Foot & Ankle Society Annual Meetings Over Time by Katherine M. Kutzer, Rochelle Bitolas, Raquel S. Garcia, Alexandra Hunter Aitchison, Julia E. Ralph, Sally J. Kuehn, Andrew E. Hanselman, Albert T. Anastasio and Samuel B. Adams in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew E. Hanselman, MD, reports consulting fees from Artelon and Arthrex, Inc; and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid from American Orthopaedic Foot & Ankle Society. Albert Thomas Anastasio, MD, reports consulting fees from QPIX Solutions. Samuel B. Adams, MD, reports royalties or licenses from DJ Orthopaedics; consulting fees from Coventus/Flower, Stryker, DJO, Orthofix, Inc, Regeneration Technologies, and Exactech, Inc; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid from American Orthopaedic Foot & Ankle Society; and stock or stock options from Medshape. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.