
Abstract
Background:
Hindfoot arthrodesis is a procedure commonly performed to address degenerative changes and/or malalignment of the hindfoot, yet robust literature comparing traditional and modern constructs is sparse. The purpose of this study is to evaluate the efficacy of nitinol staples in hindfoot arthrodesis as compared to isolated screws and combined staple and screw constructs.
Methods:
A 10-year retrospective review of all patients undergoing hindfoot arthrodesis at our institution was performed. Hindfoot arthrodesis was defined as either a triple (subtalar, talonavicular, and calcaneocuboid), double (subtalar + talonavicular), or isolated arthrodesis. Outcomes included fusion success rate and reoperation rate. A postoperative CT confirming the presence or absence of osseous bridging was required for inclusion in the fusion outcome analysis.
Results:
We assessed 113 patients who underwent arthrodesis procedures across 128 joints in the hindfoot. There was no significant difference in functional outcomes between screws, staples, or the combination screw and staple constructs used in hindfoot arthrodesis. However, screws alone were associated with a significantly higher complication rate than staple-only fixation (P = .028).
Conclusion:
Nitinol staples are effective in hindfoot arthrodesis with respect to fusion success rate and may be associated with decreased revision rates compared with traditional screws only or staple plus screw constructs. Larger studies will be necessary to validate these findings and contribute to an assessment of the usage of these nascent constructs in hindfoot arthrodesis.
Level of Evidence:
Level III, retrospective cohort study.
This is a visual representation of the abstract.
Introduction
Hindfoot arthrodesis is a procedure commonly performed to address end-stage arthritis and malalignment of the hindfoot. The arthrodesis procedure involves debridement of any remaining articular cartilage and bony apposition with implanted hardware to achieve greater hindfoot stability and functional capacity at the expense of range of motion. In fact, subtalar arthrodesis has been shown to reduce motion along the inversion-eversion axis by more than 85% whereas talonavicular arthrodesis restricts internal/external rotation by more than 50%. 15
A large proportion of patients undergoing hindfoot arthrodesis have had prior surgical intervention and hardware implantation within adjacent joints due to indiscriminate degenerative changes of the foot. 3 Selecting the proper surgical instrumentation and approach is essential to maximizing postoperative functional outcomes in an anatomically stressed region. There is no consensus, however, regarding the optimal fixation construct for this purpose.4,7,11 The few clinical studies on failure do not validate fusion via CT, which has been shown to be more accurate than x-ray in evaluating fusion.2,6,14 Furthermore, the majority of these studies do not include next-generation constructs such as nitinol staples, the use of which is rapidly growing in orthopaedics. 12
Nitinol staples are shape-memory alloys designed to undergo changes in crystalloid configuration when placed under load with the goal of sustaining compression.8,9,11 The use of these constructs has increased over time at our institution. These staples differ from traditional crossing screws in that screws tend to lose traction with load, falling out of place and causing complications postoperatively. The purpose of this study is to provide a comprehensive clinical evaluation of the efficacy of the most common constructs utilized in hindfoot arthrodesis, including next generation nitinol staples.
Methods
This study was an IRB-approved retrospective cohort study including all patients who underwent hindfoot arthrodesis from 2013 to 2023 at a single institution. The average follow-up time for patients in this study was 2.2 years. Inclusion criteria for hindfoot arthrodesis were an isolated arthrodesis of one of the subtalar, talonavicular, or calcaneocuboid joints; a double arthrodesis of the subtalar and talonavicular joints; or a triple arthrodesis of all 3 joints (Figure 1).
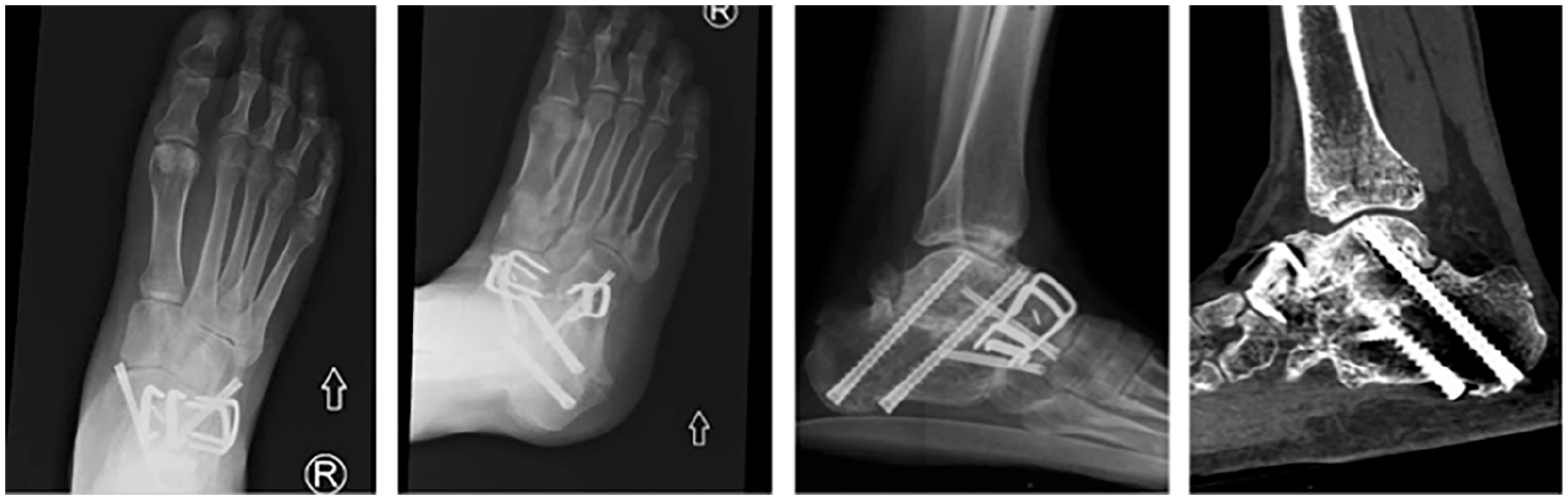
Series of plain film radiographs and sagittal CT scan demonstrating a successful triple arthrodesis of the hindfoot using a combination of screws and staples.
This study used 2 advanced nitinol staple systems: BME (DePuy Synthes, Raynham, MA) and DynaNite (Arthrex, Naples, FL). A consistent surgical technique was employed to ensure standardized fixation across procedures. Two staples were used to achieve fusion at the subtalar (ST) and talonavicular (TN) joints, whereas the calcaneocuboid (CC) joint was stabilized with a single staple. Similarly, in procedures involving screw fixation, 2 screws were placed at both the ST and TN joints, whereas the CC joint received a single screw. For the staple plus screw group, fixation was uniformly performed with 1 staple and 1 lag screw per joint to enhance construct stability. Bone graft was used in all cases: Allosync Pure (Arthrex).
The primary outcomes of this study were fusion success rate and complications including revision surgery due to nonunion, infection, or other reasons such as symptomatic hardware removal. Successful fusion of the joints was only assessed using CT imaging due to the detail of the modality. Therefore, only patients with postoperative CT image were included in analysis of these functional outcomes. For assessment of complication outcomes, patients without postoperative CT imaging were included only if they had follow-up visits after their procedure. Postoperative CTs were obtained at the 3-month, 6-month, and 1-year time points. Exclusion criteria included patients who underwent arthrodesis at joints other than those specified, staged revisions at initial surgery, or fixation methods other than nitinol staples or screws. Those without postoperative follow-up visits were excluded from complication analysis. Cases deviating from the standardized fixation protocol, surgeries outside 2013-2023, and patients with missing operative details, follow-up data, or imaging were also excluded.
These outcomes were compared across the various constructs used within the procedures—including the use of screws alone, staples alone, or a combination of both (staple plus screw)—as well as the various joints fused. This was purely an exploratory analysis that assessed omnibus significance between the construct groups, followed by pairwise comparisons if the overall group differences were found to be statistically significant at α = 0.05 or borderline significant (defined as a P value between .05 and .10). With the understanding that additional testing in an exploratory analysis increases the likelihood of type I error, P values obtained from pairwise comparisons were corrected using the Benjamini-Hochberg false discovery rate correction to reduce the likelihood of false positive results. Categorical analyses used chi-squared analysis when all expected frequencies were greater than 5, and Fisher exact testing otherwise. Numerical analyses used analysis of variance for omnibus testing and t tests for pairwise comparison. Statistical analyses were conducted in Python 3.11.7 and Microsoft Excel.
A power analysis for fusion rate was conducted based on sample size, effect size, and significance level. The calculated effect size (Cohen w) was 0.1978, indicating a small to moderate effect. The analysis yielded a power of 0.5043, suggesting a 50.43% probability of detecting a true effect, if present, at the .05 significance level.
Results
This study assessed fusion outcomes for 128 joints and complication rates for 187 joints across 113 patients following hindfoot arthrodesis. All analyses performed in this study were conducted on a per-joint basis. A description of patient characteristics can be found in Table 1. There were no statistically significant differences in demographic parameters across any of the joints studied. Because some patients underwent arthrodesis of multiple joints using varied constructs, the total number of patients is less than the sum of the number of patients in each construct group.
Patient Characteristics.

The P value reported in the table is the omnibus P value comparing each of the constructs.
Active smoking status was determined by an indication of tobacco use within the 30 days prior to the primary fusion procedure.
Among the constructs used within these procedures, there were no significant differences detected in fusion success rate between screws, staples, or a combination of the two in hindfoot arthrodesis (P = .084, calculated using Fisher exact testing) (Table 2). Given that this P value was borderline significant and given the underpowered nature of this study, further pairwise comparisons were performed, again using Fisher exact testing. No significant pairwise differences were found between any of the construct groups: screws vs staples (p = .062), screws vs staples plus screws (p = .288), and staples vs staples + screws (p = .385). These P values remained statistically insignificant following false discovery rate correction. However, when looking at the subtalar joint given the adequate sample size, subtalar joints fused as part of a triple arthrodesis with screws were found to have a significantly higher fusion rate than isolated subtalar fusion with screws (95.8% vs 65.4%, p = .011).
Fusion Outcomes Stratified by Construct and Joint. a

Each cell represents the fusion rate followed by the total number of joints attempted to be fused in parentheses (number of total joints) for the appropriate construct and joint. The P value reported in the table is the omnibus P value comparing each of the constructs.
Statistical significance at p = .011.
Regarding complication rates, staple fixation required no revision surgery in our cohort. Across the studied constructs, the omnibus test yielded a P value of 0.021 (Table 3). Following pairwise testing and false discovery rate correction, staple-only fixation was found to have a significantly lower revision rate than screw-only fixation (p = .028) as well as joint staple plus screw fixation (p = .028). Although statistical significance testing was not performed for revision subtypes, screw fixation resulted in a greater proportion of patients requiring reoperation for hardware removal and infection debridement than staple-plus-screw and staple-only fixation.
Complication Data Stratified by Fusion Construct. a

The P value reported in the table represents the omnibus significance among all 3 construct groups. Asterisks and daggers denote pairwise significant differences between the corresponding constructs at a Benjamini-Hochberg corrected value of P = .028 for both comparisons.
Discussion
Our study demonstrates no significant differences between screw-only, staple-only, or combined staple and screw fixation in achieving successful fusion in the hindfoot. However, the results presented represent a clinically significant difference of an almost 20% increase in fusion success for staple-only fixation compared with screw-only fixation. Our data on revision surgery rates further support these findings, showing a significant increase in complication rates for both screw and staple-plus-screw constructs compared to staple-only fixation in the hindfoot, even after applying false discovery rate correction.
Biomechanical data indicate that staple-only fixation does not differ significantly from screw-only fixation in terms of translational motion of the talonavicular joint along the x-y-z planes following cyclic loading, nor in fixation strength when subjected to shearing forces at the subtalar, talonavicular, and calcaneocuboid joints.8,11 Although one study found that adding a nitinol staple and plate to a 5.5-mm cannulated screw resulted in greater failure loads compared with the screw alone, this effect cannot be attributed solely to the staple, as the concurrent use of a plate—which has been shown to outperform screw fixation alone—confounds the comparison.4,9
Although our data agree with the biomechanical literature as it pertains to a statistical analysis, our study is underpowered to detect this difference given the choice to verify fusion via CT analysis. Therefore, based on the clinically significant difference in fusion rates of nearly 20% between the staple-only and screw-only groups, it is likely that staple-only fixation does indeed lead to greater fusion outcomes in the hindfoot compared with screw-only fixation. However, when the screw constructs were analyzed with regard to isolated subtalar fusion or subtalar fusion as part of a triple arthrodesis, we found a significant increase in fusion success rate when screws were used for fusion as part of a triple arthrodesis. This is an interesting secondary finding that may indicate greater benefit to screw fusion when supported by adjacent joint stabilization as seen in triple arthrodesis.
The overall difference in construct performance is further supported by our data indicating screw-only fixation to have a reoperation rate of 16% compared with 0% for the staple-only group. One possible explanation is that nitinol staples are lower-profile fixation constructs capable of providing equivalent compressive force while occupying less surface area and decreasing contact with surrounding soft tissue.1,10 This in turn could lead to decreased hardware irritation, localized inflammation, risk of infection, or risk of construct-related revision surgery.
Of note, although the joint staple and screw construct achieved high rates of fusion, it was also associated with a significantly higher revision rate than staple-only fixation. The authors believe that this is likely due to the operative technique, in which the placement of the screw across the joint interface before staple placement leads to a counteractive force that resists the dynamic compression of the staple, thereby causing backing out and local tissue irritation. Anecdotally, the authors have changed their practice patterns in light of these realizations and believe this has improved outcomes, although future, randomized study is necessary to truly compare these 2 methods.
Overall, our results support the use of nitinol staples in hindfoot arthrodesis and add to the limited data on this topic.5,13 Our results also suggest that nitinol staples may in fact be superior constructs with regard to reducing postoperative complication rates.
Our study has several limitations that should be addressed in future research. First, because of the rigorous inclusion criteria for CT imaging, our sample size was limited. This limited the power of our study and the ability to detect differences between the constructs. Furthermore, our institutional policy changed in the later time frame of this study to obtain postoperative CTs at the 3-month, 6-month, and 1-year time points for all patients. This change raises the possibility that the patients in our analysis include those that received CT imaging for clinical concern and not as part of study protocol. However, despite this potential bias, our fusion rates closely mimic those found in the literature, reducing the concern for the contributing effect of this bias.5,13
In addition, another important limitation is that the distribution of joints was not heterogenous between the constructs compared. For example, screw-only fixation was predominantly used in the subtalar joint whereas both staple and staple plus screw fixation were predominantly in the talonavicular and calcaneocuboid joints. Although these joints are all part of the hindfoot, this limits the generalizability of our findings as constructs are not compared across the same joints.
Conclusion
We found in this retrospective review that nitinol staples were an effective option for hindfoot arthrodesis as they were associated with a high fusion success rate with minimal need for reoperation. Compared with screw fixation, nitinol staples may represent a more effective option in the hindfoot. Future analyses comparing these 2 constructs across a homogenous set of joints with CT validation is necessary to corroborate the findings reported herein.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251328660 – Supplemental material for A CT-Validated Comparative Analysis of Fixation Constructs for Hindfoot Arthrodesis: Fusion and Complication Rates
Supplemental material, sj-pdf-1-fao-10.1177_24730114251328660 for A CT-Validated Comparative Analysis of Fixation Constructs for Hindfoot Arthrodesis: Fusion and Complication Rates by John Dalloul, Abhinav R. Balu, Peter C. Shen, Rachel Bergman, Ryan Filler, Armen S. Kelikian, Muhammad Mutawakkil, Milap Patel and Anish R. Kadakia in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Institutional Review Board at Northwestern Medicine, under approval number STU00215919. All study procedures complied with the ethical standards of the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all participants included in the study.
Data Availability Statement
The data supporting the findings of this study are not publicly available because of institutional policies and proprietary restrictions. As these data are derived from internal records and protected by confidentiality agreements, they are accessible only to authorized personnel within our institution. However, inquiries regarding potential data access for collaborative purposes may be directed to the corresponding author, Abhinav Balu, subject to approval and adherence to data sharing policies.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Armen S. Kelikian, MD, reports disclosures relevant to manuscript of consultancy for Treace Medical Concepts, Trimed, Trilliant Surgical, Stryker Corporation, MedShape, and Smith & Nephew. Muhammad Mutawakkil, MD, reports disclosures relevant to manuscript of support for travel/food from Arthrex, Medwest Associates, Supreme Orthopedics, and Paragon 28. Anish R. Kadakia, MD, reports disclosures relevant to manuscript of consulting fees and royalties from Arthrex Inc, and consulting fees from DePuy Synthes and ACUMED. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.