
Abstract
Background:
Acute Achilles tendon rupture (ATR) has increased in recent decades, reflecting the longer life expectancy and higher levels of activity. Surgical intervention has been the main treatment, but recently there has been growing interest in nonoperative approaches. Study compares surgical and conservative treatment of acute ATR, examining demographic data, rerupture rate, complications, and functional scale Achilles Total Tendon Rupture Score (ATRS).
Methods:
A literature review was conducted including randomized clinical trials and prospective cohorts. RevMan software was employed to ascertain the I² heterogeneity, with a view to determining whether a fixed or random effects model should be used for meta-analysis. The results were expressed as either the mean difference or relative risk (RR), as appropriate, with 95% CI.
Results:
Ten studies, published after 2010, were included in the analysis. Of the total 1327 participants, 57.8% received surgical treatment and 42.2% nonsurgical treatment. The follow-up was between 12-24 months. The rerupture rate was lower in surgical treatment (RR 0.28, 95% CI 0.15-0.50; P < .0001), although this was accompanied by a higher risk of complications (RR 2.39, 95% CI 1.57-3.63; P < .0001). The patient satisfaction was comparable between the 2 treatment groups, with no statistically significant difference on the ATRS scale (MD 0.87, 95% CI –1.18 to 2.92; P = .40).
Conclusion:
Surgical repair of acute ATR significantly reduces the risk of rerupture but it is associated with a higher rate of complications. Furthermore, there are no significant differences in the various functional scales in terms of patient satisfaction between the 2 treatments.
Level of Evidence:
II, meta-analysis
Keywords
Introduction
The Achilles tendon is involved in plantar flexion of the ankle, essential for everyday movement such as walking, running, and jumping.3,12 Rupture occurs between the second and eighth decade of life, with a peak incidence between 20 and 40 years. There is a male predominance (5:1), 3 and it is associated with sports activity in 75% of cases. 12
At the epidemiologic level, acute tendon ruptures (ATR) are frequent and increasing, with an annual incidence of 26.95/100 000 people in 1994, 5 rising to 31/100 000 in 2018 23 and 50/100 000 people in 2022. 21 This growth is due to the increase in physical activity in the population, in demand and in the age of those who practice these sports. 6
Surgical treatment is considered for many surgeons as the gold standard, especially if there is a delay in diagnosing the rupture. There are several techniques that aim to restore the anatomical length of the triceps suralis by approximating the disrupted ends and restoring the integrity. 3 The basis of conservative treatment is to place the foot in an equinus position, allowing the ends of the Achilles tendon to remain in contact. 2
The literature shows that conservative treatment should be considered in centers that use functional rehabilitation from the beginning, reserving surgical repair for those who do not have access to this system, typical of today’s public health systems. 29 In the case of functional treatment, a Spanish study defended that cast immobilization is a relatively risk-free procedure, as it avoids surgical complications and hospitalization, the time off work is shorter, and the results are comparable to those of surgical treatment.3,4 If surgery is chosen, it is associated with infection, impaired healing, and nerve damage, which are complications of surgery.14,25,32 Many published cost-analysis studies argue that surgical treatment is associated with higher costs but less pain, a factor that contributes to a better quality of life for patients who have undergone surgery compared to those who have not.10,20,30
For many decades, surgery was the primary treatment option for ruptured Achilles tendons in healthy active patients. 4 However, in 2010 a study was published that challenged the previous literature and showed that the outcomes of ATR were almost equivalent between surgical and non-operative treatment, provided that appropriate rehabilitation was followed. 34 Subsequently, several well-designed papers have been published on the best therapeutic approach. However, right now there is no study with a high level of evidence that studies professional athletes if they return to the same level of physical activity after conservative treatment, because in most cases, surgical treatment is the first choice.
The aim of our study is to compare demographic characteristics, rerupture rates, functional outcomes (Achilles tendon Total Rupture Score [ATRS]), and complication rates after conservative and surgical treatment of acute Achilles tendon rupture. We hypothesized that patients treated with a surgical treatment would have superior results compared with nonsurgical treatment after an acute Achilles tendon rupture in terms of rerupture, complications, and patient satisfaction.
Patients, Materials, and Methods
Search Strategy
This study was conducted according to the PRISMA standards for systematic reviews and meta-analyses. 26 The literature search was conducted by 2 researchers during June 2024 in the major databases (PubMed, Medline, Web of Science, Scopus, Embase and Cochrane) for articles comparing surgical and conservative treatment for acute ATR published after 2010.
The following MeSH terms were used: Achilles tendon rupture; operative treatment; non-operative treatment; re-rupture; tendon rupture score; ATRS; complications. Titles were screened and abstracts of studies of most interest were reviewed to select those considered suitable. The selected articles were then analyzed in full text using the inclusion and exclusion criteria until the final selection was made. The references of each one were also reviewed to find additional studies that met the requirements.
Inclusion and Exclusion Criteria
We included prospective observational studies or randomized clinical trials published after 2010 that aimed to compare clinical and subjective outcomes between conservative and surgical treatment of acute Achilles tendon rupture. We excluded studies with a lower level of evidence (retrospective studies, case series, reviews, biomechanical studies, or cadaver studies), published before 2010, that did not provide sufficient data for statistical analysis or whose inclusion criteria included participants younger than 16 years, chronic rupture, or rerupture. We included studies written in Spanish, English, and French.
Study Selection and Data Extraction
All information was extracted by 2 screeners, and the following data were collected: first author, year of publication, study design and methodologic characteristics, number of participants, demographic characteristics, variables analyzed, follow-up time, and main conclusions.
The variables extracted were demographic characteristics (age and sex), risk of rerupture, complications (pulmonary embolism, deep vein thrombosis [DVT], superficial and deep infection, sural nerve injury, changes in wound healing or dehiscence, failure of union of both ends, and chronic pain) and the Achilles tendon–specific functional scale, the Achilles tendon toral rupture score (ATRS).
Quality Assessment
To assess the risk of bias in trials, we used the RevMan software tool (version 5.4.1) 28 and applied the Cochrane Manual, which assesses random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. 7 Each item was rated as low risk (green), unclear risk (yellow), or high risk (red). When there was doubt about the risk of an item, this was resolved by a third reviewer.
Statistical Analysis
Qualitative and quantitative analysis of results was performed using RevMan statistical software (version 5.4.1). 28 Dichotomous variables, such as rerupture rate and clinical complications, were grouped as risk differences and their 95% CIs using the Mantel-Haenszel method. For continuous variables, such as the ATRS scale, the mean difference and its 95% CI were used.
Heterogeneity was assessed using the I2 statistic. The fixed effects model was used when I2 was ≤50%, and a random effects model was used if I2 was >50% and heterogeneity was significant. Meta-analysis was considered statistically significant when P values were <.05. The results were presented as numerical data together with the forest plot. The funnel plot was calculated to analyze publication bias.
Results
Studies and Assessment of Study Quality
A total of 1890 articles were retrieved from the different databases (Figure 1). Duplicates and those not relevant to the objective were excluded, leaving 38 full-text studies for analysis. Twenty-eight studies were excluded because they did not meet the inclusion and exclusion criteria, leaving a total of 10 articles, 9 randomized clinical trials (RCTs)6,9,11,14,16,20,23,25,34 and 1 prospective observational study. 13

Flow chart showing method of article selection.
The risk of bias assessment showed a low risk of bias for the outcomes analyzed, with the exception of the risk of detection (Figure 2).7,28

Risk of bias summary revealing the review of the authors’ decisions about each risk of bias item.
Figure 3 shows a combined result of the studies. It highlights the low risk of selection, with details of the method of randomization and allocation concealment. On the other hand, there is a high risk of blinding the assessors in more than 50% of the trials, which is justified in only 2 trials.16,20
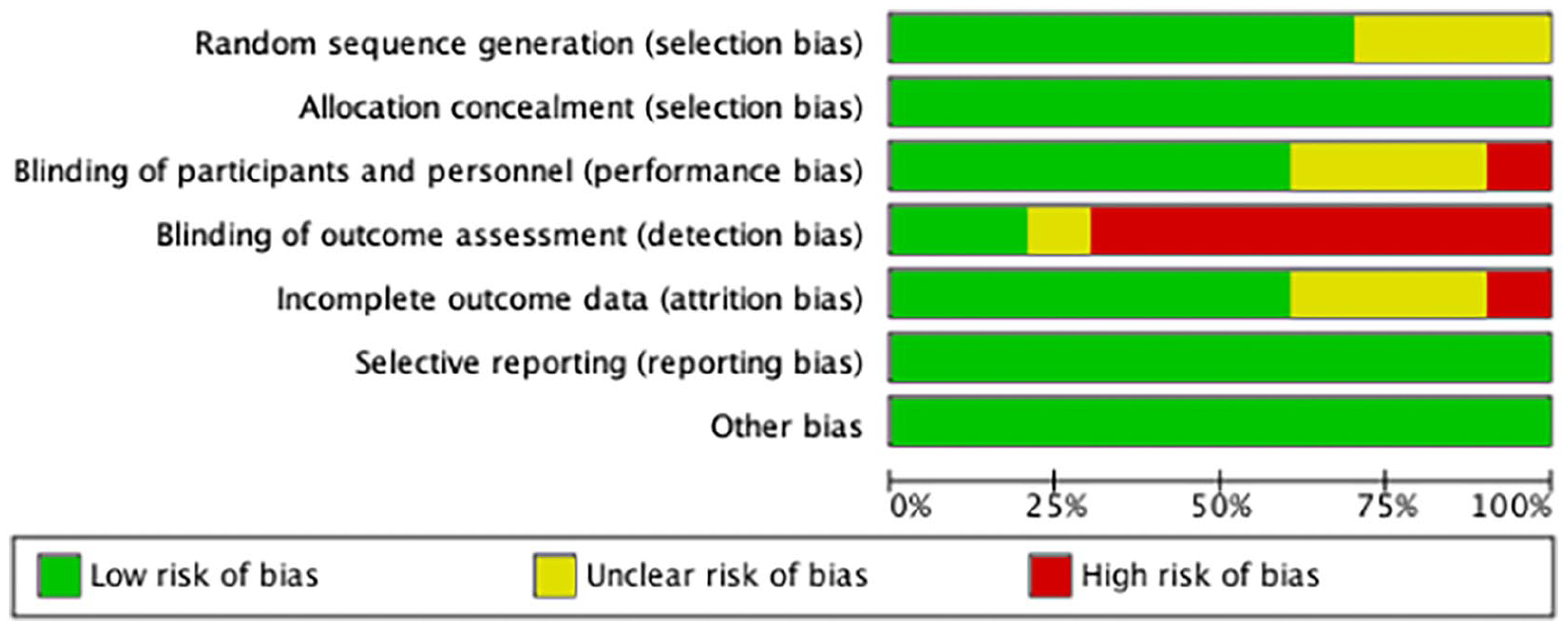
The pooled risk of bias for all included studies divided by source of bias.
Baseline Patient Characteristics
Table 1 shows the summary characteristics of the included articles. Sample sizes ranged from 34 to 526 participants, with a total of 1327 patients included in the systematic review, 767 surgical (57.8%) and 560 conservative (42.2%).
Baseline characteristics of included studies (N=10).

Abbreviations: NS, nonsurgical treatment; RCT, randomized controlled trial; S, surgical treatment.
There was a predominance of males with an age ranging from 39.7 to 41.1 years (40.26 years for surgical treatment and 40.5 years for conservative treatment). Follow-up ranged from 12 to 24 months, except for 1 RCT with a follow-up of 15.7 years. 14
Meta-analysis of Clinical Outcomes
Rerupture rate
The rerupture rate was analyzed in 8 of the 10 studies, 6 as a primary objective6,9,14,24,25,34 and 2 as a secondary objective.11,21 There were 13 of 682 cases with surgical treatment (1.9%) vs 39 of 479 (8.14%) with nonsurgical treatment. Using a fixed effects model (I2 = 0%; P = .66), a significantly lower rate of rerupture was found with surgical compared with conservative treatment (relative risk [RR] 0.28, 95% CI 0.15-0.50; P < .0001) (Figure 4).

Forest plot of meta-analysis for rerupture rate (n = 8). M-H, Mantel-Haenszel.
Achilles Tendon Total Rupture Score (ATRS)
The ATRS scale was analyzed in 6 trials, all as a primary endpoint.13,14,16,21,23,25 It is a self-administered scale consisting of 10 questions about daily life and physical activity, where the patient answers from 1 to 10, with a maximum score of 100 points. A fixed effects model was used (I2 = 0%, P = .94), and no statistically significant differences were found (MD 0.87, 95% CI –1.18 to 2.92; P = .40) (Figure 5).
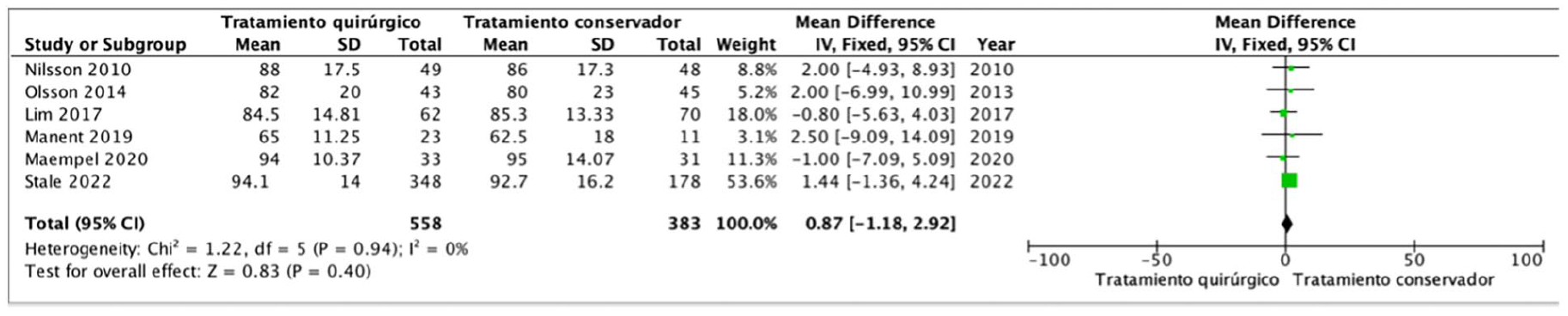
Forest plot of meta-analysis for ATRS scale (n = 6). IV, inverse variance.
Complications rate
The presence of complications other than rerupture was analyzed in 9 articles, all as a secondary outcome.6,9,11,14,21,24,25,34 There were 92 complications in surgical treatment (13.29%) and 25 in functional treatment (5.19%). Table 2 shows a summary of the different complications according to intervention, with particular emphasis on infection and healing problems in surgery and DVT and chronic pain in conservative treatment. Significant differences were found in favor of conservative treatment (RR 2.39, 95% CI 1.57-3.63; P < .0001) (Figure 6).
Summary of complications in surgical treatment and conservative treatment.


Forest plot of meta-analysis for complications rate (n = 9). M-H, Mantel-Haenszel.
Discussion
Recent studies have shown very inconsistent results, calling into question the best management of acute ATR. 27 This meta-analysis demonstrates that surgery is associated with a reduction in the rerupture rate compared with conservative management. However, it is associated with a higher rate of complications with no difference in patient satisfaction. These results are analyzed before treatment and at the final follow-up period. For future studies, it would be beneficial to expand these data and conduct analyses at different follow-up intervals to reach more consistent conclusions.
Rerupture Rate
Previous publications indicate that surgical treatment reduces the rate of rerupture compared with conservative treatment, with risk differences of approximately 5% to 7%,8,15,22,29,33 and no difference between open and percutaneous surgery. 18 It has been observed that as rehabilitation methods improve, the difference between the 2 interventions decreases. 19 Soroceanu et al 29 published in 2012 that using functional rehabilitation with early range of motion, rerupture rates were similar for both treatments, which was replicated in subsequent publications.22,34 Therefore, surgical repair should be considered first in centers that do not use early range of motion protocols.29,34
The included articles show a lower rate of rerupture with surgery, without showing statistically significant differences,6,9,11,14,23,25,34 with the exception of the most recent study. 21 These results mean that in our study rerupture occurs in 1.9% of surgeries and 8.14% of conservative treatments (difference in risk: 6.24%).
Rehabilitation22,29 or patient age 1 are the factors that most influence this rerupture, suggesting that older patients may benefit more from conservative treatment than younger patients because of the complications associated to surgery and the basal situation of the older patients. 1
Functional Scales
Lantto et al 12 showed that both treatments produce similar results in terms of clinical scores and patient satisfaction, with the main weakness being the difference in rehabilitation programs.
The ATRS scale is the most widely used because of its simplicity and accessibility. In our analysis, the mean ATRS score is 84.6 (65-94.14) for surgery and 83.58 (62.5-95) for nonoperative treatment, with no difference found (MD 0.87, 95% CI –1.18 to 2.92; P = .40). It was shown that surgery, by allowing more aggressive rehabilitation, may improve strength and allow earlier return to activities, which may influence patient perception.11,17,31
Other Complications
Complications such as wound scarring, infection, or nerve damage are seen with surgery but not with conservative treatment. Others, such as DVT or pulmonary embolism, which depend on factors such as good anticoagulation, can occur with either treatment. Studies show that the complication rate is higher with surgery, around 10% to 15%, 18 and lower with percutaneous intervention.1,5,8,15,22,27,29,33
Our results are consistent with the majority of the published literature, with 13.29% complications with surgical treatment (infection and scarring problems) vs 5.19% with conservative treatment (DVT and chronic pain). The absolute risk reduction is 8.1% with nonsurgical treatment.
This meta-analysis has a number of limitations. First, it includes 2 studies with Level II evidence, which reduces the evidence in this article. Second, the results may have been influenced by unpublished studies, although the funnel plot showed no publication bias. Third, it has an important clinical limitation in that the studies did not use a common rehabilitation protocol, which makes interpretation difficult. Fourth, surgical techniques continue to change, and the current analysis is based on the techniques used in the index studies. Newer less invasive approaches may be associated with different outcomes than reported herein.
In conclusion, our analysis of recent literature suggests that surgical treatment of acute Achilles tendon rupture lowers the risk of rerupture but carries a higher risk of surgery-related complications. Overall, average patient satisfaction appears comparable between treatments.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251327219 – Supplemental material for Achilles Tendon Rupture Treatment Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251327219 for Achilles Tendon Rupture Treatment Systematic Review and Meta-analysis by Sara España Fernández de Valderrama, Beatriz García Martínez and Laura Ezquerra Herrando in Foot & Ankle Orthopaedics
Footnotes
Appendix
Achilles Tendon Rupture Score (ATRS)
Funnel plot of publication bias for rerupture rate
Funnel plot of publication bias for ATRS scale
Funnel plot of publication bias for complications rate
Ethical Approval
This study compares previously published articles that have been approved by the relevant ethics committee. Our work does not require informed consent from patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.