
Abstract
Background
Endoscopic flexor hallucis longus (FHL) tendon transfer can be used in the management of acute or chronic Achilles tendon rupture (ATR), including in elite sportspeople. A recent cadaveric study demonstrated that an increased ultimate load could be applied using an FHL tendon transfer with interference screw and cortical button applied using a tension slide technique compared with interference screw alone. The aim of this study was to explore patient-reported functional outcomes following this modification to this operation.
Methods
We reviewed the imaging, history, patient-related outcome measures (PROMs), and complications of 17 patients who underwent endoscopic FHL tendon transfer for chronic ATR using the modified FHL reconstruction technique. The primary outcome was the Manchester-Oxford Foot Questionnaire (MOxFQ), EuroQol–5 Dimensions (EQ-5D), and visual analog score for pain (VAS-Pain) with a mean follow up of 1.5 years.
Results
Seventeen patients (11 male, 6 female) underwent endoscopic FHL tendon transfer for chronic ATR between September 2020 and May 2023. Mean (SD) age at the time of surgery was 58.3 (16.1) years, and mean (SD) BMI was 27.6 (4.8). A specific event in the history associated with the rupture was present in 13 of 17 patients (76.5%); the median (IQR) time between injury and surgery was 33 weeks (21-42). Sixteen surgeries were primary procedures for chronic ATR, and 1 surgery was a revision procedure after a failed open acute ATR repair. MOxFQ, EQ-5D, and VAS-pain scores all showed a statistically significant improvement postoperatively (minimum 10 months) when compared to preoperative scores. There was 1 symptomatic complication of tibial neuritis (5.9%).
Conclusion
Endoscopic FHL tendon transfer for chronic ATR augmented using a cortical button as well as an interference screw seems to be a safe and effective procedure, with patients reporting a statistically significant improvement in health-related quality of life, pain, and specific foot and ankle outcome function.
Keywords
Introduction
Achilles tendon rupture is a significant and increasingly common injury, particularly among active individuals engaged in sports or high-intensity physical activities. The incidence of Achilles tendon rupture is between 8 and 29 per 100 000 people per year,10,16,33 with the majority of cases occurring during sporting activities and running.4,13 Intrinsic patient characteristics such as increasing age, male sex, obesity, and comorbidities such as end-stage renal failure have been shown to predispose patients to Achilles tendon pathology, and extrinsic factors such as drugs including fluoroquinolones and corticosteroids can increase the risk of tendon rupture. 41
Despite an increasing incidence of rupture10,33 the proportion receiving operative intervention for an acute Achilles tendon rupture is decreasing16,33 because of the increase in “functional bracing” for nonoperative treatment, which enables early full weightbearing and rehabilitation. A number of studies have demonstrated equivocal outcomes for operatively vs “functional bracing”–managed patients with fewer complications in the nonoperative group.30,43 However, there is also contrasting evidence that suggests surgery for acute tears results in lower rerupture rates compared with nonoperative management.7,24 Surgical treatment may result in increased power and torque and therefore this is the preferred management in elite athletes,25,39,43 although whether this is applicable to the general population it is unclear.
Chronic Achilles tendon rupture (ATR) 9 or failure of acute Achilles tendon rupture management frequently leads to weakness, instability, increased dorsiflexion of the ankle, swelling, and pain. These symptoms are a result of increased Achilles tendon length, which effectively defunctions the gastrocnemius and soleus muscles to a degree. Because of this loss of effective ankle plantarflexion, nonoperative management with physiotherapy is reserved for those who have maintained most function or very low demand patients or those at too high risk for an anesthetic. Therefore, in most cases of chronic ATR a surgical approach is required to restore function. Open repair and tendon transfer (most frequently flexor hallucis longus) is associated with relatively large incisions, wound complications, calf atrophy, and scarring.8,20,27
Advances in surgical technology have allowed the development of endoscopic minimally invasive techniques in the treatment of chronic ATR with the potential advantages of reduced postoperative pain, faster recovery rates and improved cosmetic outcomes. 8 The flexor hallucis longus (FHL) tendon is most commonly used as is a long thin tendon with good tensile strength27,28,40 and many studies have reported good clinical outcomes following endoscopic FHL transfer for both acute and chronic Achilles tendon ruptures.1 -3,12,15,18,35,44
The use of a cortical button in addition to an interference score for FHL transfer for Achilles tendon rupture has been described in an open procedure. 29 A biomechanical study has subsequently demonstrated that the use of a cortical button in addition to an interference screw in FHL tendon transfer significantly increased ultimate load. 23 The combination of a second line of fixation and the benefit of increased pullout strength seem to offer benefits to patients so we have therefore modified the endoscopic FHL tendon transfer procedure to use a cortical button in addition to the interference screw.
Aims and Objectives
The aim of this study was to evaluate the clinical function and outcomes following a modification to the endoscopic FHL reconstruction for chronic ATR.
Methods
Study Design and Setting
This study design was a retrospective analysis of prospectively collected patient-reported outcome measures (PROMs) for 18 consecutive patients undergoing endoscopic flexor hallucis longus (FHL) tendon transfer (EFHLTT) for chronic Achilles tendon rupture (ATR) by a single surgeon over a 3-year period at 3 hospitals in the United Kingdom. This study followed the Declaration of Helsinki and the Guidelines for Good Clinical Practice and was reported in line with the STROBE guidelines for observational studies. 42 As the study was embedded within routine clinical care, and registered as a local service evaluation project for analysis of routinely collected data, ethics approval was not required.
Participants
Patients were defined as having a chronic Achilles tendon rupture (ATR) if they had a confirmed tear on imaging (either magnetic resonance imaging or ultrasonographic scan) and were seen in clinic at least 6 weeks postinjury (for those who had a specific memory of the injury occurring; Figure 1 demonstrates an MRI scan of chronic ATR). These patients had either failed conservative management or had a missed diagnosis of acute ATR. The patients who were included in this study were those who opted for surgery after a discussion of management options including nonoperative intervention. Our criteria for offering surgery were patients who had reduced function with their chronic ATR, were previously ambulating independently and would likely be suitable candidates for general anesthetic. Each patient who underwent endoscopic FHL tendon transfer prospectively completed preoperative patient-reported outcome measures (PROMs), which were stored in a national online registry on the day of surgery. Patients completed follow-up PROMs and clinical assessment at routine time points following surgery and were followed up for a minimum of 10 months.

Sagittal magnetic resonance imaging scan demonstrating high signal in the Achilles tendon.
Variables
The primary outcome was a validated foot and ankle PROM, the Manchester-Oxford Foot Questionnaire (MOXFQ),5,6,22 which was assessed at a minimum of 1 year following endoscopic FHL tendon transfer. Secondary outcomes included validated general health-related quality of life PROMs including the EuroQol–5 Dimensions, 5 Levels (EQ-5D-5L) visual analog scale (EQ-VAS), and pain visual analog scale (VAS-Pain).
Although we were not directly able to clinically assess the (theoretical) additional stability provided by the tension slide, we performed careful complication analysis to identify the safety profile of this operation and fixation method.
Complications identified by either the patient or surgeon in outpatient clinics were prospectively recorded at the point of diagnosis and categorized using the adapted Clavien-Dindo complication classification. 19
Operative Technique
All operations were conducted by an experienced foot and ankle surgeon (RR). The patient is positioned in the recovery position with the operating side down. This allows for safe anesthesia but full access to the posterior ankle for hindfoot endoscopy. A standard 2-portal hind foot endoscopy as described by van Dijk et al 38 was performed in each case. Retrocalcaneal bursal excision and calcaneoplasty are initially performed ensuring access to the posterior calcaneus. The FHL tendon is then identified medially. If there is an os trigonum or prominent Steida process, this is detached and removed to allow access to the FHL tendon. The tendon is freed from its sheath shaving carefully medial to lateral to avoid damage to the adjacent neurovascular bundle. The tendon is then grasped through a third proximal and central portal and held under full tension. It is then released from medial to lateral using endoscopic scissors. The tendon is then whipstitched and sized to do a line to line drilling and biotenodesis insertion. Through the proximal medial incision, a 2.4 spade-tipped wire is drilled bicortically through the calcaneus (Figure 2A) and overdrilled with a cannulated flexible reamer matching the size of the tendon to a depth of 25 mm (Figure 2B). This is generally sufficient with the length of FHL harvested for tensioned docking. The threads of the whipstitched tendon are then shuttled from the medial portal to the accessory proximal medial portal ensuring the tendon is not caught up in the soft tissue bridge. A specific challenge of this technique is passing the button through the posterior soft tissues from the proximal medial portal to the calcaneus with dislodgement of the button from its handle. As such a locked button is preferred that can be unlocked once passed. The senior author has found the Arthrex proximal biceps button to be ideal for this. The button is threaded onto the whipstitch and using the stable handle the button is inserted from the proximal portal through the heel and unlocked and flipped just under the calcaneus (Figure 2, C and D). This step can be checked on radiographs. The foot is held in full plantarflexion and a tension slide technique is used to fully dock the tendon. A mark should be made on the tendon 25 mm from the end to ensure visualization that the tendon is fully docked as much as possible. Additional fixation is achieved with an interference screw, which is again inserted through the proximal medial portal (Figure 2, E). The key steps are demonstrated using saw bones on Figure 2 with the final construct shown in Figure 2F. A postoperative radiograph of the construct is shown in Figure 3.

Saw bone photographs demonstrating the technique of endoscopic flexor hallucis longus tendon transfer using a cortical button and interference screw. (A) The flexor hallucis longus tendon has been whipstitched and a 2.4 spade-tipped wire is drilled bicortically through the calcaneus. (B) Overdrilling with a cannulated flexible reamer matching the size of the tendon to a depth of 25 mm. (C) Whipstitched tendon threaded into cortical button and introduced into calcaneus. (D) Button detached and flipped on plantar aspect of calcaneus. (E) The tension slide technique has been used to fully dock the tendon and the interference screw is being inserted. (F) The final construct with cortical button and interference screw.

Postoperative radiograph of the flexor hallucis longus tendon transfer with interference screw and cortical button construct.
Post op care
All patients were immobilized nonweightbearing in an equinus cast for 2 weeks to allow wounds to heal.
At 2 weeks they were given a walking boot and allowed to fully weightbear in this and could remove it at night. No strict protocol of wedges was applied but 1 or 2 wedges were allowed for comfort. Patients were referred to physiotherapy at this appointment with the expectation that physical therapy would begin at week 2 or 3. At 2 weeks, active and band-assisted plantar flexion against resistance and active dorsiflexion to neutral was allowed. Seated heel raises could begin at 2 weeks.
Patients were expected to wean from the walking boot by 6 weeks. Dorsiflexion beyond neutral for gait, standing heel rises (starting bilaterally, and progressing to single heel raise), and calf raise was allowed from 6 weeks.
Calf stretch was allowed from 12 weeks. Return to impact activities such as running was physiotherapy led but generally initiated from 12 weeks.
The majority of patients did not engage in regular sports activities, but those who were engaged in sports such as netball, dancing, and trail running were guided through a sports-specific rehabilitation with the expectation that they would return to full competitive sporting by 6 months.
We did not change our postoperative protocol from that used when using an interference screw without cortical button.
Bias
We attempted to address potential sources of bias within the study design by purposefully minimizing exclusion criteria and including consecutive patients to reduce selection bias. Data were collected prospectively minimizing recall bias.
Study Size
Given there are currently no published data on outcomes from this technique, we included all patients eligible for inclusion.
Quantitative Variables
We collected data on age, gender, BMI, imaging modality, distance of rupture from calcaneal insertion, and time between injury and surgery.
Statistical Methods
The paired t test for parametric data was used for continuous outcomes and descriptive statistics used for categorical data. All analyses were performed with Python SciPy package. 36 Statistical significance was defined as P <.05.
Ethical Approval and Funding
This study was registered as a local service evaluation project for analysis of routinely collected data including prospectively collected PROMs. There was no funding to support this study.
Results
Between September 2020 and May 2023, 17 patients (11 male; 6 female) underwent endoscopic FHL tendon transfer for chronic Achilles tendon rupture by a single surgeon. The mean ± SD age was 58.3 ± 16.1 years. The mean BMI was 27.6 ± 4.7. All patients ambulated without walking aids prior to injury, and 3 of the patients engaged in regular sport (trail running, netball, and dancing). Sixteen were primary operations, 1 was a revision following rerupture after primary Achilles tendon repair. Eight were diagnosed on ultrasonographic scan, and 9 were diagnosed on magnetic resonance imaging (MRI) scan. Four patients had no history of acute injury, the median time between injury and surgery of the other 13 patients was 33 weeks (interquartile range 21-42 weeks). The median distance between site of rupture and calcaneal insertion was 5.5 cm with an interquartile range of 4-6 cm in the 13 patients that had this information reported in their scans. The mean follow up was 1.5 ± 0.7 years with a minimum of 10-month follow-up. The primary outcome was the MOXFQ score, which was available for 16 patients (94%). Figure 4 summarizes enrollment and follow-up. Table 1 and Figure 5 demonstrate a statistically significant improvement in all MOXFQ domains following surgery (P < .05). The greatest improvement was observed in walking/standing scores, but improvements within the domains of pain and social interaction were also statistically significant (P < .05).

Flowchart demonstrating patient participation and follow-up rates in study.
Patient-Reported Outcomes Following Primary Endoscopic Flexor Hallucis Longus Tendon Transfer for Chronic Achilles Tendon Rupture.

Abbreviations: EQ-5D-5L, EuroQoL–5 dimensions, 5 levels; MOXFQ, The Manchester-Oxford Foot Questionnaire; VAS, visual analog scale.
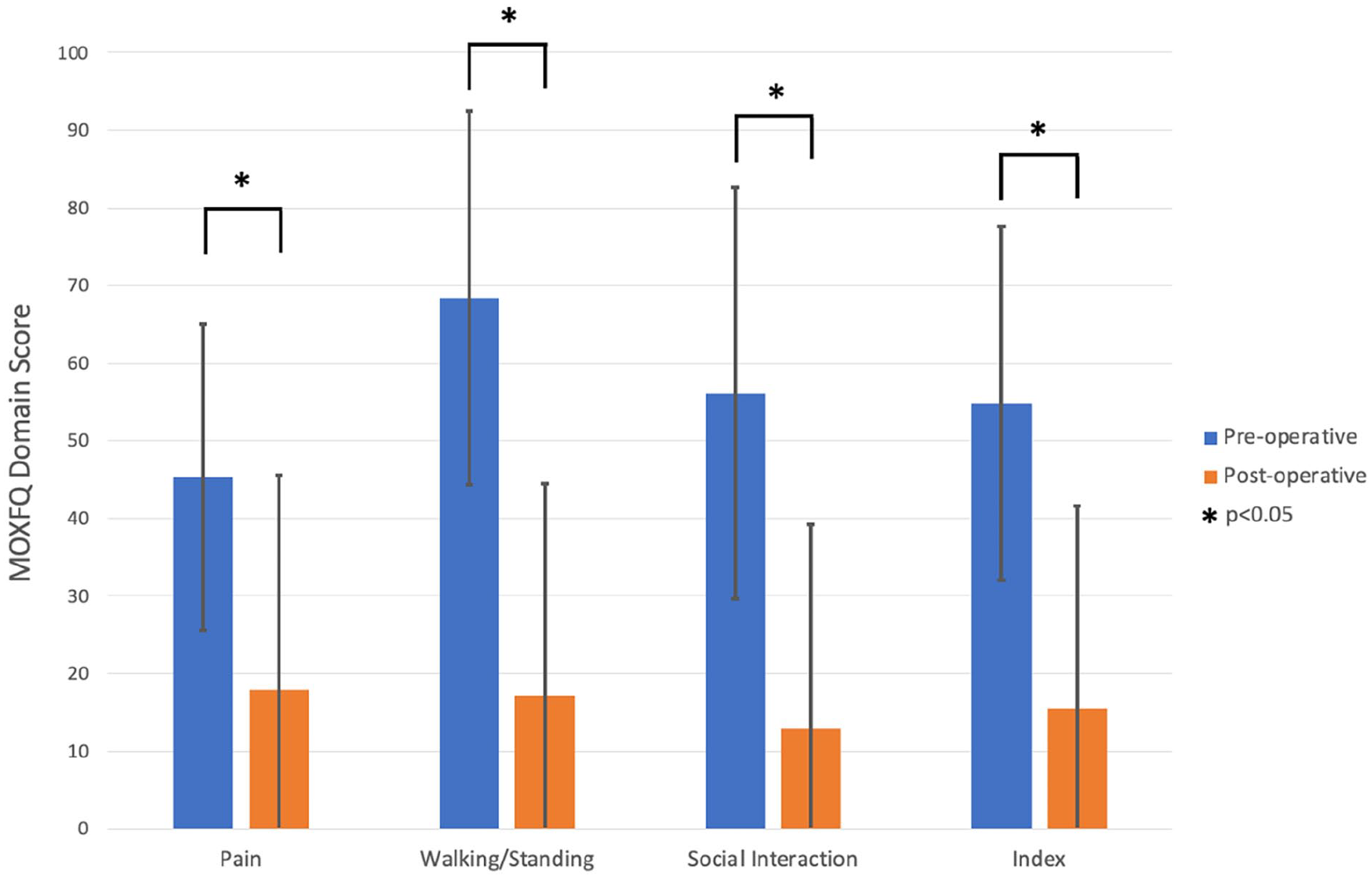
Graph demonstrating statistically significant improvement in pre- and postoperative outcomes in all MOXFQ domains following endoscopic flexor hallucis longus tendon transfer for chronic Achilles tendon rupture.
Secondary outcomes included the EQ-5D and VAS pain. Table 1 shows the improvement in both the EQ-5D-5L Index and VAS which were statistically significant (P < .05). Similarly there was a statistically significant improvement in VAS Pain (P < .05).
There was only 1 symptomatic postoperative complication (5.9%), which was classified as Grade 3B 19 : a case of tibial nerve neuritis secondary to scarring and the patient went on to have a tarsal tunnel release. There was 1 case (grade 2A) where the interference screw backed out but the cortical button remained in place and the patient remained asymptomatic (Figure 6).

Postoperative radiographic case where the interference screw backed out but the cortical button remained in place, holding the repair. The patient was asymptomatic.
Discussion
Key Results
This is the first study to report clinical outcomes of using a cortical button and interference screw for FHL tendon transfer. Patients reported a statistically significant postoperative improvement in all of our PROMs (MOXFQ, EQ-VAS, and VAS pain) when compared to their preoperative PROMs. These PROMs demonstrate an improvement in patients’ subjective symptoms including pain, instability, and ability to undertake activities including work and recreational activities.
Evidence
There have now been multiple publications describing endoscopic FHL tendon transfer for both acute and chronic Achilles tendon rupture (Table 2).1 -3,12,15,18,34,35,40,44-47 A systematic review of studies to date have indicated that endoscopic FHL transfers are associated with fewer complication rates relative to open FHL reconstruction while simultaneously maintaining favorable clinical outcomes and a return to preinjury sporting abilities. 34 There are, however, limited numbers of comparative studies of endoscopic vs open FHL tendon transfer for Achilles tendon rupture. Gerstner et al 12 published a series of 18 endoscopic FHL transfers and 24 open FHL transfers for noninsertional Achilles tendinopathy and concluded that both procedures were effective, the endoscopic treatment resulted in a statistically significantly greater improvement in the AOFAS score (52.8% in the endoscopy group compared to 41.4% in the open group), and there were slightly fewer complications. The complications experienced by the open group included 3 permanent complications (2 hypertrophic scarring at the incision, 1 persistent edema of the lower limb) and 4 nonpermanent complications (1 wound dehiscence, 2 sural nerve irritation, and 1 tendinitis of the FHL tendon) whereas the endoscopic group only had 4 patients that had temporary scar sensitivity.
Summary of Papers Reporting Clinical Outcomes of Endoscopic Flexor Hallucis Longus (FHL) for Achilles Tendon (AT) Rupture.
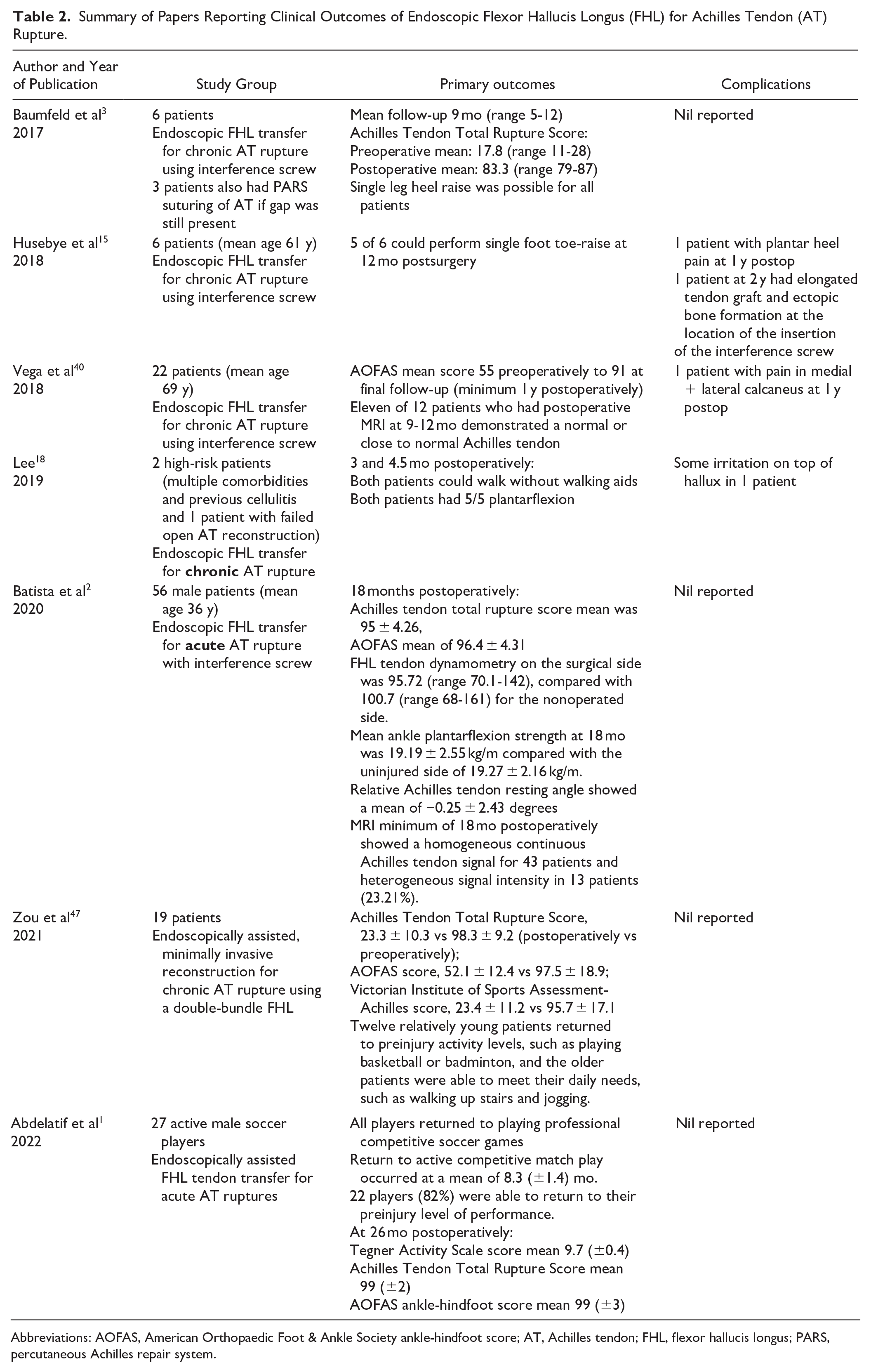
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; AT, Achilles tendon; FHL, flexor hallucis longus; PARS, percutaneous Achilles repair system.
The use of cortical buttons is common in other procedures, notably distal biceps repair17,21,26,31,32 and anterior cruciate ligament reconstruction. 11 Cortical button fixation has been found to be biomechanically stronger than suture anchors, bone tunnels, interference screw fixation and transosseous sutures by several studies.11,17,21,26,31,32,37 Mazzocca et al 23 determined that the interference screw had the lowest displacement when compared with suture anchors, a bone tunnel, and a cortical button. The combination of these 2 (cortical button and interference screw) therefore offer the potential for an excellent environment for tendon transfers. 14
Shinabarger et al 32 published an open technique of a bicortical button and interference screw for FHL tendon transfer for Achilles tendon rupture. They felt that as well as offering biomechanical superiority in strength the combination afforded other advantages: firstly that if failure of the biotenodesis screw did occur then the cortical button offers a second line of fixation to avoid failure of the tendon fixation (as seen in our case Figure 6); second, the cortical button allows tensioning of the tendon as it acts as a pulley allowing the surgeon to assess and adjust the tension based on foot position, etc. They concluded that by using both the cortical button and the interference screw in soft tissue to bone attachment, the ideal properties of high load to failure with minimal displacement are both present, allowing early mobilization and weightbearing and potential improvement in patient outcomes.
Neary et al 25 performed biomechanical analysis on 12 matched pairs of cadaveric lower legs and demonstrated that the use of a cortical button in addition to an interference screw in FHL tendon transfer significantly increased ultimate load (343.72 + 68.93 N compared with 255.62 + 77.17 N in interference screw alone specimens). It did not significantly affect cyclic displacement or structural stiffness.
Strengths
There are a number of strengths of this study; there is minimal loss to follow-up, and use of a validated patient-reported outcome measure strengthens the study’s outcome assessments, providing a standardized and objective metric for future studies to evaluate and compare participant experiences against.
Limitations
This study is limited by a small sample size, limiting generalizability and external validity. Short-term follow-up prevents a comprehensive understanding of long-term effects, whereas missing data on return to sports hinders assessing functional outcomes fully. The absence of a comparator group means it is difficult to assess the utility of the cortical button compared with endoscopic FHL tendon transfer alone. As our senior surgeon now performs all FHL tendon transfers endoscopically, we also do not have an open surgery comparison group. The cost of the additional cortical button was £300 and we have not done a cost-benefit analysis because of the lack of a control group.
Conclusion
Endoscopic FHL transfer for Achilles tendon rupture can be augmented using a cortical button applied using a tension slide technique. Patients undergoing this procedure reported statistically significant improvements in quality of life, pain, and specific foot and ankle function following surgery. Further studies are required with longer-term follow-up and greater patient numbers to further assess the efficacy of this technique with clinical comparison to standard interference screw fixation alone to see if the theoretically increased security translates to improvements in return to sport or PROMs.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251325862 – Supplemental material for Endoscopic Flexor Hallucis Longus Transfer With Interference Screw and Additional Tension Slide Cortical Button for Chronic Achilles Tendon Rupture
Supplemental material, sj-pdf-1-fao-10.1177_24730114251325862 for Endoscopic Flexor Hallucis Longus Transfer With Interference Screw and Additional Tension Slide Cortical Button for Chronic Achilles Tendon Rupture by Ayla Claire Newton, Samuel Franklin, Thomas Lorchan Lewis, Sanjana Mehrotra, Siddhartha Murhekar, Vikramman Vignaraja and Robbie Ray in Foot & Ankle Orthopaedics
Footnotes
Ethical approval
This study was embedded within routine clinical care and registered as a local service evaluation project for analysis of routinely collected data; therefore, ethics approval was not required.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robbie Ray, MBChB, ChM(T&O), FRCSed(Tr&Orth), FEBOT, reported disclosures related to manuscript of previously receiving funding from Arthrex beyond the scope of this study and general disclosures being on the surgeon advisory board for Enovis; consults for Enovis/Novastep and Medartis; and has teaching commitments for Enovis, Novastep, Marquardt UK, Medartis, and Arthrex. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
All patients gave verbal consent to have their data, imaging and PROMs viewed & published anonymously for research purposes.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.