
Abstract
Background:
Subtalar arthrodesis is a commonly performed procedure for the treatment of posttraumatic or primary osteoarthritis and several hindfoot deformities. The primary objective of this study is to evaluate the efficacy and safety of a minimally invasive technique for cartilage removal of the subtalar joint using a modified sinus tarsi approach.
Methods:
An anatomical study was performed on 8 pairs of fresh frozen cadaveric feet. A modified 2.5-cm sinus tarsi approach was used to access the subtalar joint. Cartilage removal was performed in 2 groups using either a 13-mm Shannon burr (GB) or a curette (GC) with subsequent systematic dissection. Standardized scaled photographs of the resected articular surfaces were analyzed in ImageJ software to quantify cartilage removal. Nearby vulnerable anatomical structures such as the intermediate and lateral dorsal cutaneous nerves, peroneal, tibialis posterior, flexor digitorum longus, and flexor hallucis longus tendons were assessed for injury.
Results:
The area of completely removed cartilage in GC was median 79.7% talar and 76.6% calcaneal. In GB, median 67.8% of the talar cartilage and 76.8% of the calcaneal cartilage was removed. The overall mean of cartilage resection was 73% (±7.7). There was no statistically significant difference between the groups. Anatomical structures at risk were not inadvertently injured.
Conclusion:
Subtalar cartilage resection can be performed safely using a minimally invasive modified sinus tarsi approach and either a Shannon burr or curettes. The amount of cartilage resection is less than that reported in the literature for open cartilage resection, but may be beneficial in select patient populations at increased risk for wound healing compromise and infection.
Level of Evidence:
Level III, comparative cadaver study
This is a visual representation of the abstract.
Introduction
Posttraumatic osteoarthritis of the subtalar joint after calcaneus fracture is the most common indication for arthrodesis of the subtalar joint (52%), followed by primary osteoarthritis (17.5%) and rigid pes planovalgus deformity (9.5%). 19 Especially after nonoperative treatment of intra-articular calcaneus fractures, there is an increased risk of conversion to arthrodesis of the subtalar joint (16.9% after nonoperative vs 3.9% after surgical treatment of calcaneal fractures). 11
In addition to the traditional open surgical technique for subtalar arthrodesis, there has been a significant increase in arthroscopic surgery in recent years because of the comparatively lower overall complication rates (13.1% arthroscopic, 20.3% open surgery). 19 Dysesthesia of the sural nerve occurs relatively frequently at 13.3% (open) and 5.8% (arthroscopic). 17 A review of the literature on subtalar joint arthrodesis reveals a lack of reporting on specific complications, particularly infections and wound healing disorders. In a systematic review of 22 studies, 7 studies reported the occurrence of infections, with a range of 1% to 6%. 19 The number of high-risk patients with diabetes, rheumatism, peripheral arterial disease, or a history of smoking was very limited.
Meta-analyses have shown a generally increased risk of wound healing disorders and wound infections for patients with diabetes mellitus (odds ratio [OR] 1.53), rheumatoid arthritis (OR 1.53), and nicotine abuse (OR 1.79), meaning that these risk groups in particular can benefit from minimally invasive surgical techniques.9,14
The percutaneous, minimally invasive removal of cartilage from joints using burrs without fluoroscopy and arthroscopy has already been successfully trialed in other joints (eg, the metatarsocuneiform joint in preparation for Lapidus arthrodesis).18,22,24
As arthroscopic procedures can be time-consuming and require a high level of equipment and material expenditure, the primary aim of this study is to investigate the effectiveness and safety of cartilage resection of the subtalar joint using a minimally invasive, modified sinus tarsi approach and to compare 2 different techniques for cartilage removal (Shannon burr vs curette) in order to provide a less invasive procedure for high-risk patients.
We hypothesize that percentage cartilage resection of the subtalar joint using a minimally invasive approach is equivalent to open cartilage resection using a sinus tarsi approach. To assess the safety of the surgical technique, adjacent anatomical structures, specifically the intermediate and lateral dorsal cutaneous nerves, the tendons of the peroneal (PT), tibialis posterior (TP), flexor digitorum longus (FDL), and flexor hallucis longus (FHL) muscles will be evaluated for potential injury.
The null hypothesis is that there is no significant difference between the groups in the percentage of the articular surface that is decartilaginized.
Methods
This anatomical study was performed on 8 pairs of fresh frozen cadaveric feet. Assuming an effect size of 0.8, and testing dependent samples by comparing left vs right legs (randomly assigned to different surgical methods), a sample size of 8 pairs (16 individual specimens) is required to achieve a significance level of 0.05 and a power of 0.8 using G*Power 3.1.9.7. All cadaver donors signed a declaration of consent for the use of their bodies for scientific purposes during their lifetime.
None of the specimens showed signs of previous surgery on the hindfoot, which would have led to exclusion. Furthermore, none of the specimens showed any significant deformity.
The right and left feet of each pair were randomly assigned to either group curette (GC) or group burr (GB).
All procedures were performed by a single surgeon, who is experienced in MIS techniques.
Surgical Technique
A mini-open sinus tarsi approach with a defined incision length of 2.5 cm was performed 2 cm distal to the margin of the fibula tip pointing toward the base of the third metatarsal, enabling the distraction of the joint, which would otherwise be prevented by the highly taut skin (Figure 1).
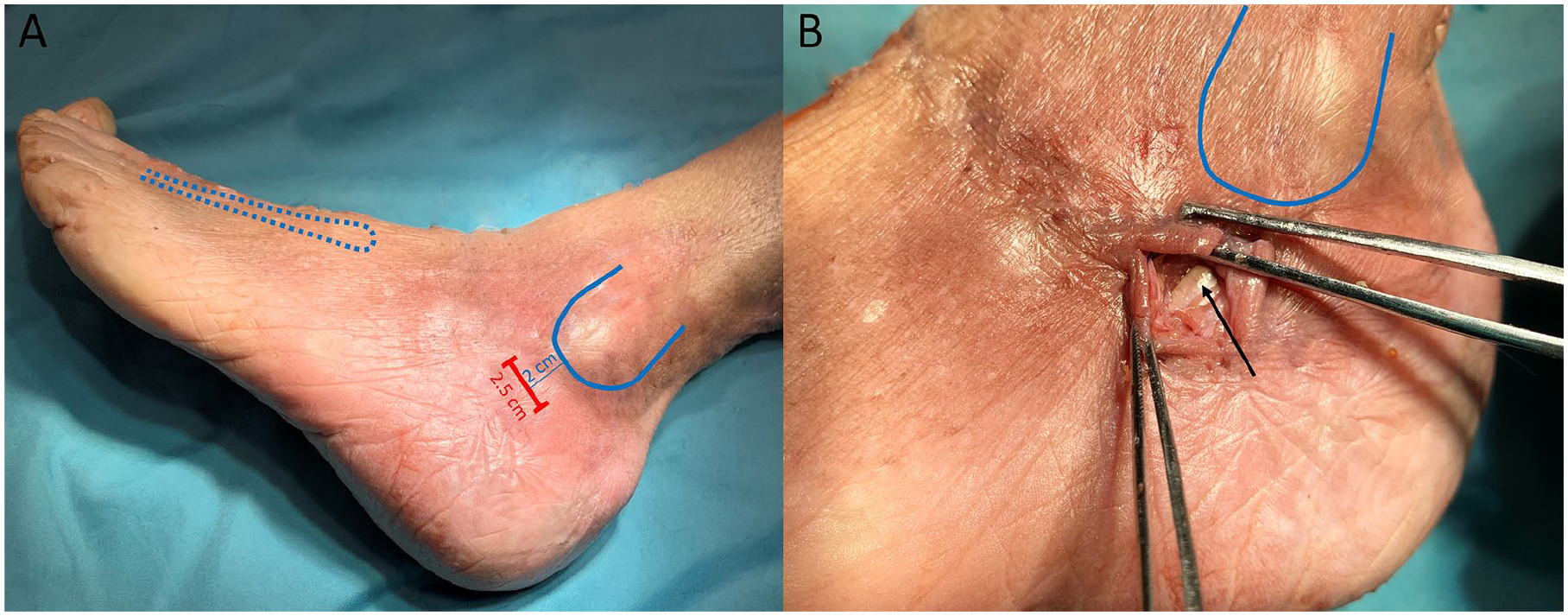
Approach planning and skin incision. (A) The 2.5-cm modified mini-open sinus tarsi approach (red line) is situated 2 cm distal to the margin of the fibula tip pointing at the third metatarsal base (blue dotted line). (B) After skin incision and dividing the peroneal tendon sheath, the peroneus brevis tendon is visible (marked by the black arrow).
The peroneus brevis tendon sheath was identified, partially divided longitudinally, and the tendon was gently held to the side caudally (Figure 1).
After partial resection of fatty tissue in the tarsal sinus, the subtalar joint was exposed.
Distraction of the joint using a Hintermann spreader with K-wire placement in the lateral talar process and calcaneus allows visualization of the entry level of the posterior facet of the subtalar joint (Figure 2).

Access to the subtalar joint. (A) K-wires inserted into the lateral talar process (black arrow) and calcaneus (white arrow). The Hintermann distractor provides access to the posterior facet of the subtalar joint. (B) The Shannon burr can be inserted into the joint. (C) Instruments used for cartilage removal: small curette and a 2 × 13-mm Shannon burr.
Cartilage was then removed systematically from distal to proximal from the articular surfaces of the posterior facet using a curette (GC) or a 2 × 13-mm Shannon burr (3000 rpm) (GB) (Figure 2) only based on tactile feedback without fluoroscopy. The anterior and middle facets were not prepared.
Outcome Measure
After completion of the subtalar joint resection, all specimens were systematically dissected. Intermediate and lateral dorsal cutaneous nerve, PL, TP, FDL, and FHL were visualized and examined for injuries. The talus was then completely removed and the articular surfaces were cleaned of debris and visualized (Figure 3). Standardized, scaled photographs of the articular surfaces were taken and analyzed using ImageJ software (Image Processing and Analysis in Java – Wayne, Rasband; National Institutes of Health, Bethesda, MD). The resection areas were semiautomatically marked using color thresholding and manual correction to identify all areas of resected and remaining cartilage and to determine the areas in millimeters-squared (Figure 4). This was used to calculate the percentage of the subtalar joint that was completely decartilaginized.
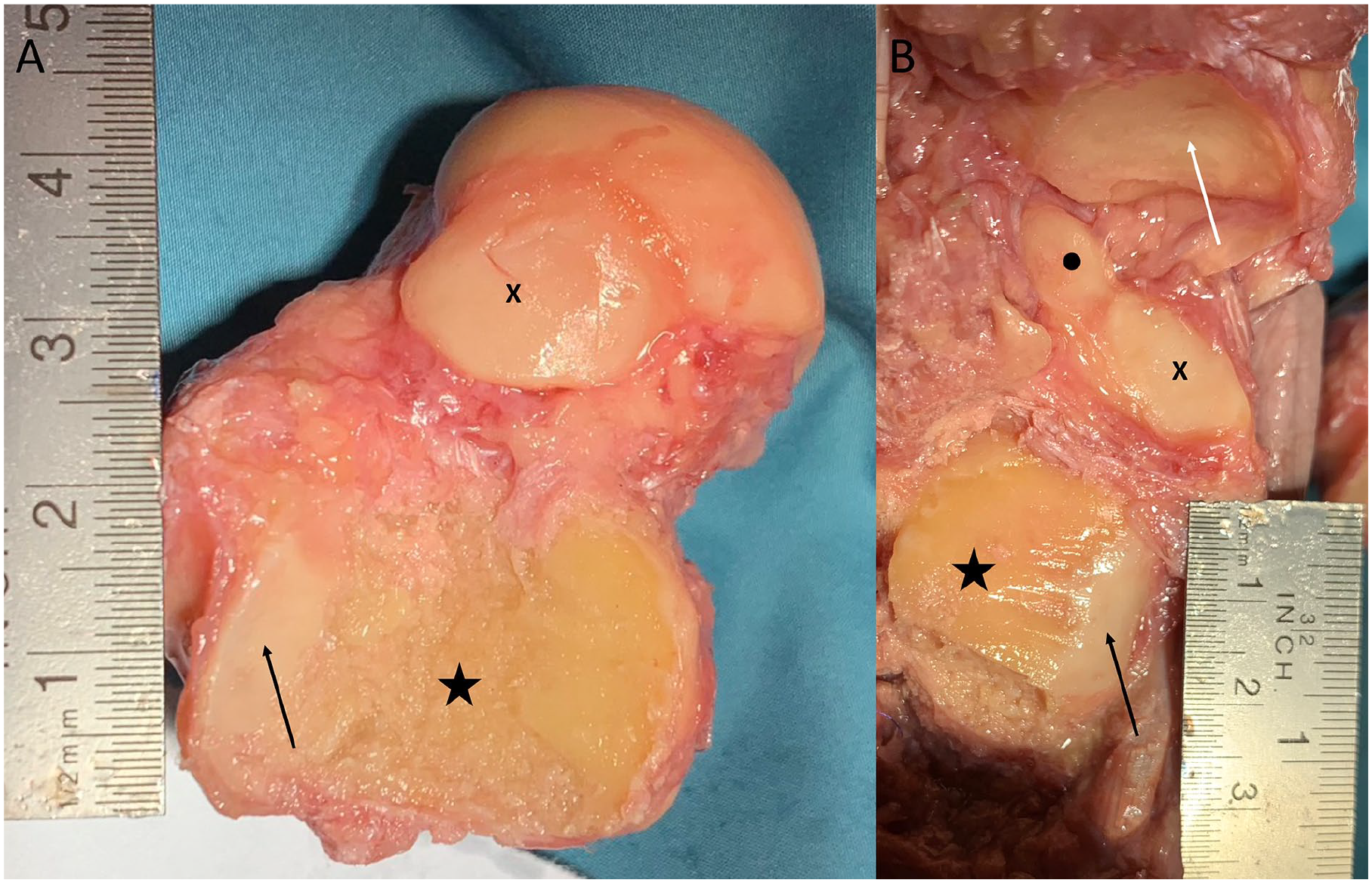
Evaluation of cartilage removal after dissection. (A) Talus extracted, axial view from plantar. The star marks the posterior calcaneal articular surface. The arrow points to the remaining cartilage at the posteromedial portion. X shows the middle calcaneal articular surface. (B) Axial view of the calcaneus. The star marks the posterior facet. The arrow indicates the remaining cartilage at the posteromedial portion of the posterior facet. X marks the middle facet, and the point shows the anterior facet. The white arrow indicates the cartilage of the navicular bone.
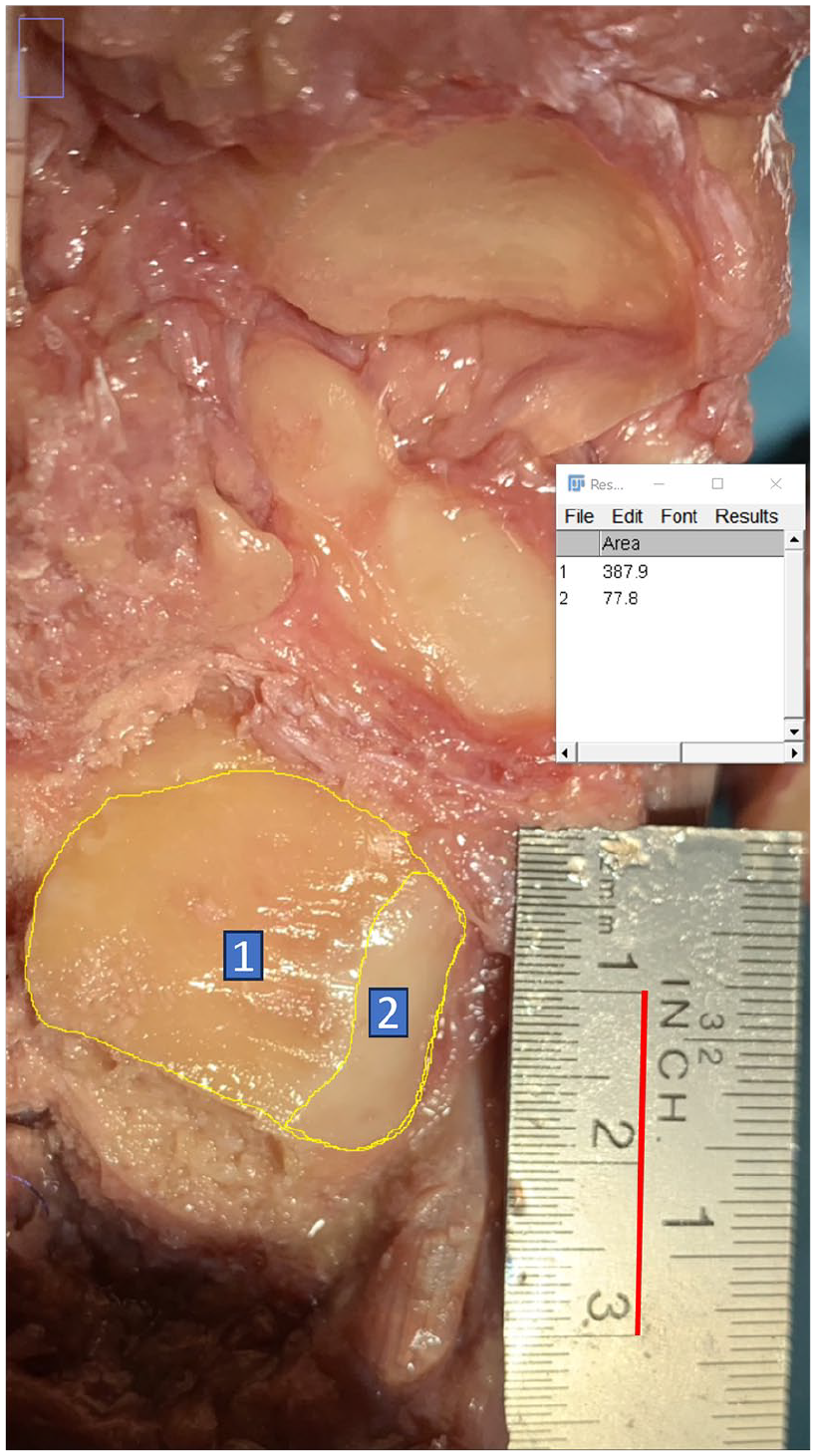
Quantitative analysis of cartilage removal in ImageJ Software. Scaled photograph of the posterior articular surface of the calcaneus after cartilage removal and talus extraction. The scale was set to the red line = 20 mm on the ruler. Yellow lines mark the semiautomatically defined areas completely removed (1) and remaining (2) cartilage in ImageJ software with data output window at the right side (area in mm²).
Statistical Methods
Data analysis was performed using Jamovi (version 2.3) statistics software. 21 Statistical significance was defined at the 5% level (P ≤ .05). The Shapiro-Wilk test was used to evaluate the normal distribution of the measured areas before and after cartilage removal. Comparative descriptive statistics included independent samples t test, mean, median, quartiles, and interquartile range.
Results
All of the 16 feet were eligible for analysis. The Shapiro-Wilk test confirmed the normal distribution of all area measurements.
Primary Outcome
The area of completely removed cartilage in GC was median 79.7% (IQR 13.8) talar and 76.6% (IQR 14.7) calcaneal. In GB, median 67.8% (IQR 10.1) of the talar cartilage and 76.8% (IQR 19.2) of the calcaneal cartilage was removed. The overall mean of cartilage resection was 73% (±7.7). Table 1 and Figure 5 summarize the descriptive statistics.
Descriptives.

Abbreviation: IQR, interquartile range.

Boxplots demonstrating descriptive statistics of overall cartilage resection in group comparison. The blue box shows 25% and 75% quartiles with interquartile ranges. The black square marks the mean values, and the horizontal black line marks the median values. The violin lines illustrate the asymmetric distribution of the values. Note that the curette group had only outliers with low values of cartilage resection, whereas the other values are concentrated above the mean values.
The largest areas of the remaining cartilage were identified on the posteromedial calcaneal articular surface, which is challenging to access because of the curvature of the articular surface.
Injuries to the intermediate and lateral dorsal cutaneous nerves, PT, TP, FDL, and FHL tendons were not recorded in any case.
Secondary Outcome
The independent samples t test yielded a P value of.171 for talar articular surface denudation and .905 for calcaneal articular surface denudation in the group comparison. Thus, the null hypothesis that there is no significant difference between the groups in the percentage of articular surfaces that have been decartilaginized is accepted.
Discussion
It has been shown that an average cartilage resection of 73% (±7.7%) can be safely performed through a minimally invasive 2.5-cm modified sinus tarsi approach without damaging potentially compromised surrounding anatomical structures. In the group comparison, no differences were found in the amount of cartilage resection using the curette and the 13-mm Shannon burr. Although not statistically significant, there was a near 10% difference in the removal of cartilage from the talar articular surface (79.7% GC vs 67.8% GB). This difference may reach significance in larger samples. We assume that the reason for this is that the curvature of the articular surface can be better followed with a curved curette than with a rigid, straight burr. This is also true in accessing the posteromedial region, which is often difficult to reach. However, it is not possible to determine with certainty whether the retention of cartilage in this region causes a significant valgus deformity, particularly if additional cancellous bone grafting is performed laterally.
The violin curves of the box plots (Figure 5) provide insight into the learning curve of the procedure. The downward outliers with low resection rates were the initial preparations in each case, and with increasing repetition, significantly higher resection areas were observed in the last repetitions. This suggests that rapid progress through practice may be expected. Our findings go along with Zhao et al, 24 who conducted an anatomical investigation on a smaller sample size (N = 5) of specimens, evaluating the efficacy of open subtalar joint cartilage resection in comparison to the minimally invasive reamer technique. The median cartilage resection achieved via minimally invasive techniques was notably higher than that achieved through open techniques (76.6% vs 73.8%, respectively). Nevertheless, an investigation into the safety of the procedure was not part of their study. When compared to the existing literature, the percentage of cartilage resection achieved in this study (73%) is less than that achieved by the open approach (94%). 1
Nevertheless, it is noteworthy that the occurrence of pseudarthrosis following subtalar arthrodesis is relatively high in open or arthroscopic procedures, reaching up to 16.9%. 19 This suggests that the complete cartilage resection under visualization may not be the sole determining factor, but rather that patient-specific risk factors, such as diabetes and nicotine abuse, may have a significant impact. A comprehensive retrospective study of isolated subtalar joint arthrodesis (N = 184) identified nicotine abuse as a significant risk factor for nonunion, with 92% of nonsmokers and only 73% of smokers fusing. 6
The stability of the arthrodesis is also a contributing factor (double screw fixation vs single screw, delta technique vs parallel, autologous vs allogenic bone grafting, etc).
It seems probable that a certain amount of articular cartilage is not entirely resected when minimally invasive percutaneous approaches are employed, because of the absence of direct visualization. 18 However, in a clinical study, Vernois and Redfern achieved a fusion rate of 96% (N = 70, 6-month follow-up) after percutaneous resection of the metatarsocuneiform joint in Lapidus arthrodesis, which is lower than the general pseudoarthrosis rate of 8.1% reported in meta-analyses of foot and ankle arthrodesis.3,22 There is still insufficient evidence as to how much of the articular surface needs to be completely decartilaginized to achieve adequate fusion and stable arthrodesis.
In a retrospective analysis of 42 ankle and subtalar joint arthrodesis, Dorsey et al 5 provided evidence that stable fusion is achieved when >33% of the articular surfaces are visibly bony overbuilt on sagittal CT. Similar results were observed by Glazebrook et al, 8 who identified a CT morphologic fusion of 25% to 49% of the articular surface in correlation with clinical joint stability as a critical value for successful fusion at 6-month follow-up (N = 275).
Mader et al12,13 demonstrated that after percutaneous retrograde tibiotalocalcaneal (TTC) nail arthrodesis with complete omission of subtalar joint preparation, 90% of arthrodeses still fused clinically and radiographically within 16 weeks (N = 10). The authors attributed the fusion to the partial destruction of the posterior facet during the opening drill. Lowe et al 10 demonstrated in a cadaver study that only 4% of the calcaneal and 5.9% of the talar articular surface is destroyed when using a standard 12-mm opening drill for TTC arthrodesis.
This observation is supported by a retrospective multicenter study by Mulhern et al (N = 40), who detected a radiologically progressive fusion after retrograde TTC nailing without debridement of the subtalar joint in the follow-up period of 11.6 ± 9.1 months (32% complete fusion, 40.5% partial fusion). 16
Therefore, the resection of mean 73% of the subtalar articular cartilage achieved in this study can be expected to result in successful fusion of the joint.
Our findings align with those of Zhao et al, 24 who similarly identified that there was an increased risk of inadvertently milling depressions and unevenness of the rounded articular surfaces when using the burr, which could potentially lead to misalignment, shortening or delayed union (Figure 6). The present study demonstrated that inadvertent bone resection can be avoided through the use of a curette with an equivalent degree of cartilage resection.
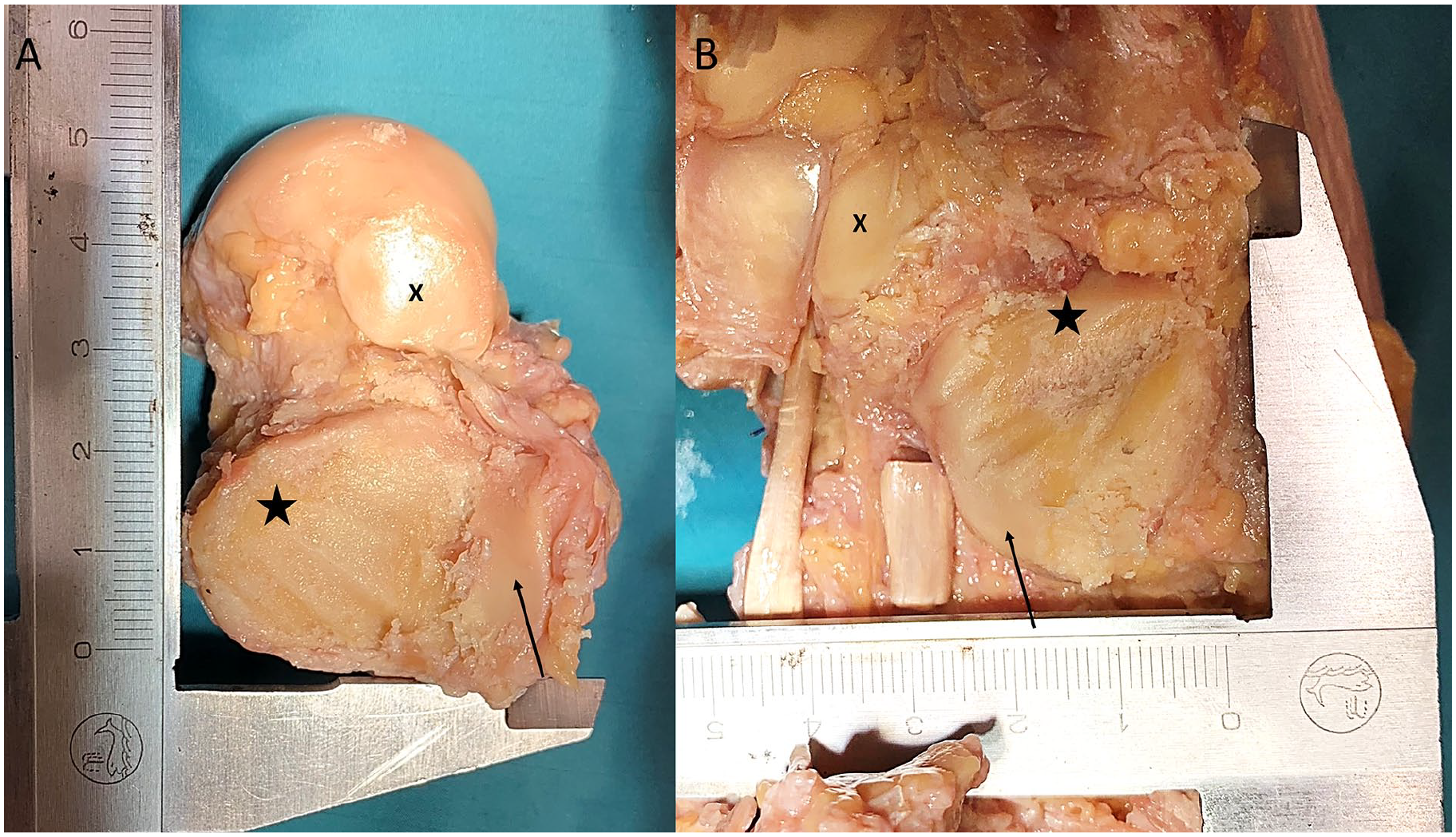
Example of uneven cartilage removal using the Shannon burr. (A) Talus extracted, axial view from plantar. The star marks the posterior calcaneal articular surface. The arrow points to the remaining cartilage at the posteromedial portion. X shows the middle calcaneal articular surface. The cartilage removal left small indentations on the bone. (B) Axial view of the calcaneus. The star marks the posterior facet. The arrow indicates the remaining cartilage at the posteromedial portion of the posterior facet. X marks the middle facet. The burr created a substantial groove in the cancellous bone.
Nevertheless, the exclusive utilization of a curette renders the process of opening the subchondral bone lamella more arduous, particularly in the context of sclerotic bone. Consequently, it is recommended that multifocal drilling of the arthrodesis surface be undertaken in addition. It is conceivable that arthroscopy could enhance the quality of joint preparation. Nevertheless, the mean operative time for arthroscopic subtalar joint arthrodesis is relatively long (50-160 minutes) and necessitates the use of a substantial quantity of material.2,17 Although the precise preparation time was not documented, an estimation of approximately 15 minutes was deemed appropriate, with no notable discrepancies between the groups.
In particular, patients with diabetes mellitus, Charcot arthropathy, nicotine abuse, peripheral vascular disease, and rheumatoid arthritis may therefore benefit from the reduced invasiveness, potentially less scarring, shorter operative time, and lower rates of wound healing failure and infection associated with MIS techniques.4,6,7,15,20,23
However, the limitations of this MIS technique are any type of bony corrections, such as those required for posttraumatic hindfoot varus, posttraumatic loss of Böhler angle, rigid pes planovalgus, or pes cavovarus, which demand direct visualization of the joint. In the authors' opinion, minimally invasive cartilage resection is most appropriate for high-risk patients with planned in situ arthrodeses with limited bony axis correction. Furthermore, this approach may prove beneficial in tibiotalocalcaneal arthrodesis. Because of the limited visualization, precise anatomical knowledge of the course of the joint and intraoperative fluoroscopy are necessary, and therefore cadaver training is strongly recommended before the technique is applied to the patient.
This study is subject to the usual limitations of cadaveric studies, with a relatively small sample size and therefore limited direct applicability of the results to clinical practice. The absence of visualization renders it challenging to discern the remaining areas of cartilage or regions of pronounced sclerosis, which could potentially elevate the risk of pseudarthrosis. Randomized controlled clinical trials are required to evaluate the actual bony fusion after minimally invasive resection of the subtalar joint compared with the classic open procedure. All procedures were performed by a single surgeon. Despite the semiautomatic measurement of residual cartilage areas in the ImageJ software, there remains a degree of subjectivity in the assessment. It is possible that the learning curve may have had an adverse effect on the results of the cartilage resection, given that significantly higher percentages of cartilage could be removed in the later preparations. Furthermore, the exact time of preparation was not documented, so that this can only be estimated retrospectively.
Conclusion
Cartilage resection of the subtalar joint can be safely performed minimally invasively. The extent of cartilage resection is inferior to that achieved by the open approach. The literature provides evidence that 73% cartilage resection appears to be sufficient for stable fusion. The minimally invasive technique offers potential advantages in terms of infection risk, wound healing disorders, scarring, potential nerve injury, and shorter operative time. It might be a useful alternative in planned in situ subtalar arthrodesis or tibiotalocalcaneal arthrodesis in select high-risk patients.
Future case series are needed to compare fusion rates and postoperative complications of open and minimally invasive subtalar joint arthrodesis.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251315666 – Supplemental material for Minimally Invasive Cartilage Resection of the Subtalar Joint: An Anatomical Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114251315666 for Minimally Invasive Cartilage Resection of the Subtalar Joint: An Anatomical Study by Sebastian Schilde, Dariusch Arbab, Maria Felsberg, Heike Kielstein, Karl-Stefan Delank and Natalia Gutteck in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because it is a cadaver study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.