Abstract
Category:
Midfoot/Forefoot; Other
Introduction/Purpose:
The typical cavovarus deformity seen in patients with Charcot-Marie-Tooth involves plantarflexion of the first ray. Surgical correction often includes a dorsiflexion osteotomy at the first metatarsal base or medial cuneiform. The exact apex of the deformity has never been proven, although it is presumed to be within the medial cuneiform. The aim of this study was to utilize weight-bearing computed tomography (WBCT) to localize and quantify the plantarflexion deformity in CMT patients.
Methods:
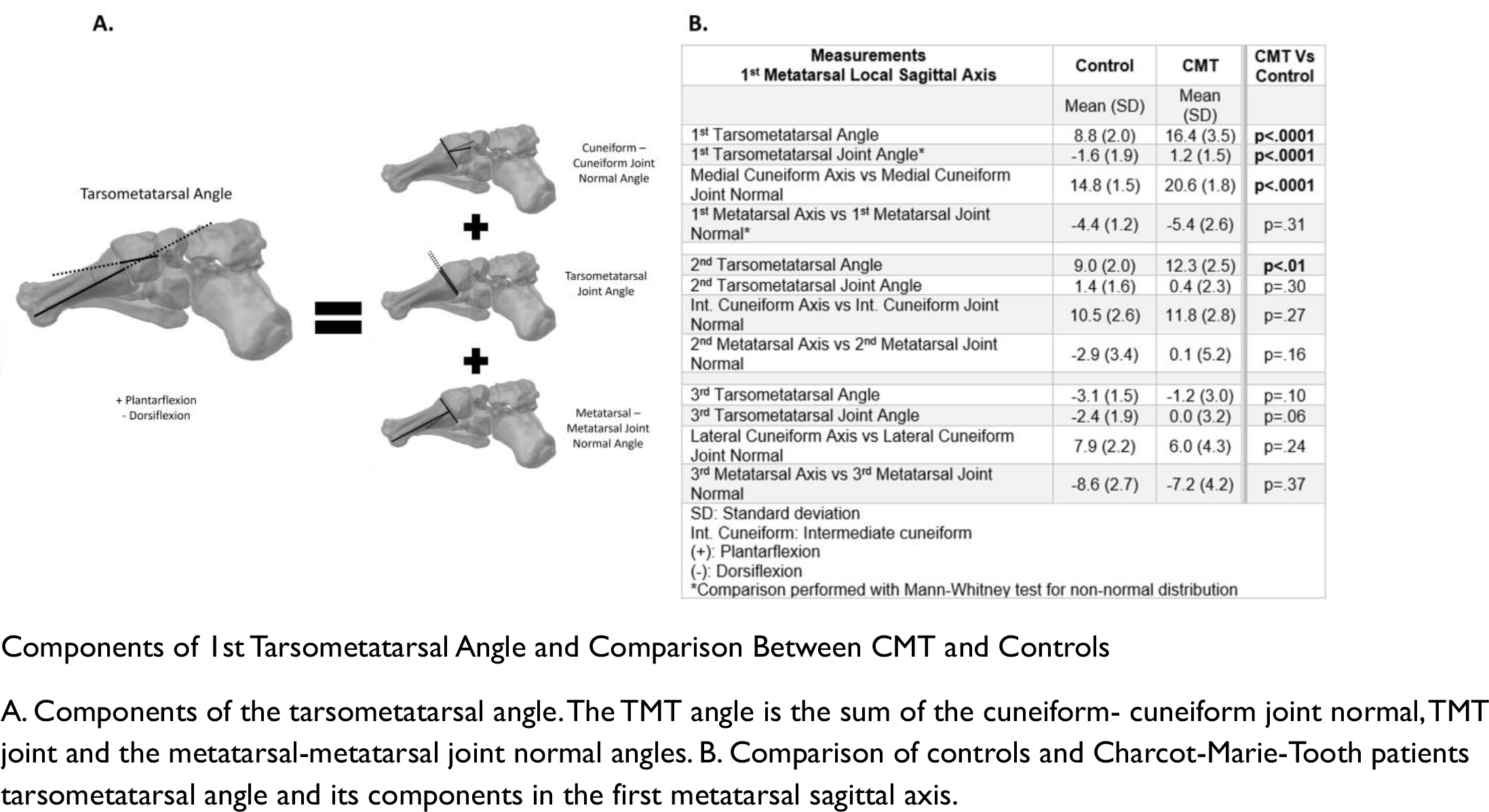
WBCTs of 16 CMT patients with lateral Meary’s angle >20 degrees were compared to controls utilizing semi-automated analysis software (Disior Bonelogic). Due to the complex deformity seen in CMT patients, a local coordinate system based on the first metatarsal was used. The tarsometatarsal angle was subdivided into components (cuneiform-cuneiform joint normal, tarsometatarsal joint and metatarsal-metatarsal joint normal) and compared between CMT and controls (Figure 1A). CMT patient’s first, second and third rays were also compared. Means were compared with a 2-sample t test (p <.05).
Results:
CMT patients had significantly more plantarflexion of the first ray than controls (8.8 versus 16.4 degrees respectively (p < 0.001)) (Figure 1B). The largest difference of was found at the cuneiform-cuneiform joint normal with 20.6 degrees of plantarflexion in CMT patients versus 14.8 degrees in controls (p <.0001). There was also approximately 2 degrees of plantar flexion at the TMT joint (p <.001) but no difference at the metatarsal-metatarsal joint normal angle. When comparing the flexion of the first ray versus the second, as well as the second versus the third rays, there were significant differences in the tarsometatarsal, cuneiform-cuneiform joint and metatarsal-metatarsal joint angles.
Conclusion:
Plantarflexion deformity in CMT patients is primarily an osseous deformity at the level of the medial cuneiform with a lesser contribution from the tarsometatarsal joint. This finding has implications for CMT surgery regarding location of a dorsiflexion osteotomy at the apex of deformity.