
Abstract
Category:
Arthroscopy; Ankle
Introduction/Purpose:
The pathomechanism of anterolateral ankle impingement (ALAI) due to a distal fascicle of the anterior inferior tibiofibular ligament (DF-AITFL) has not been fully elucidated. In addition, due to its rarity, no definitive diagnostic criteria have been established for ALAI by DF-AITFL. This study was performed to document the symptom characteristics, MRI and arthroscopic findings, and postoperative clinical outcomes of ALAI due to a DF-AITFL.
Methods:
Twelve patients (5 males and 7 females of mean age 34.4 years (range 21-76 years)) diagnosed with ALAI due to DF-AITFL from November 2017 to August 2021 and treated surgically were included in this study. Symptom characteristics and symptom-related medical histories were evaluated. Clinical outcomes were assessed using a visual analogue scale (VAS), American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot functional scale, and foot function index (FFI). In addition, magnetic resonance imaging (MRI) and arthroscopic findings were evaluated.
Results:
All 12 patients had a history of ankle sprain prior to symptom onset. Mean VAS, AOFAS ankle-hindfoot functional scale, and FFI improved significantly postoperatively. DF-AITFL was confirmed by MRI in all cases (Fig. 1). Bone edema of the talus was observed in two cases (16.7%), and cartilage abnormalities in three (25%). Arthroscopy showed that the DF-AITFL contacted the anterolateral aspect of the talar dome during ROM in all cases and that the AITFL was bent where it contacted the anterolateral dome of the talus in 3 cases (25%). Partial tear or adhesion of the DF-AITFLwas noted in seven cases (58.3%), and cartilage deformation at the anterolateral talar dome in 4 cases (33.3%).
Conclusion:
ALAI due to DF-AITFL should be considered a possible cause of anterolateral ankle pain, especially in cases of ankle sprain.
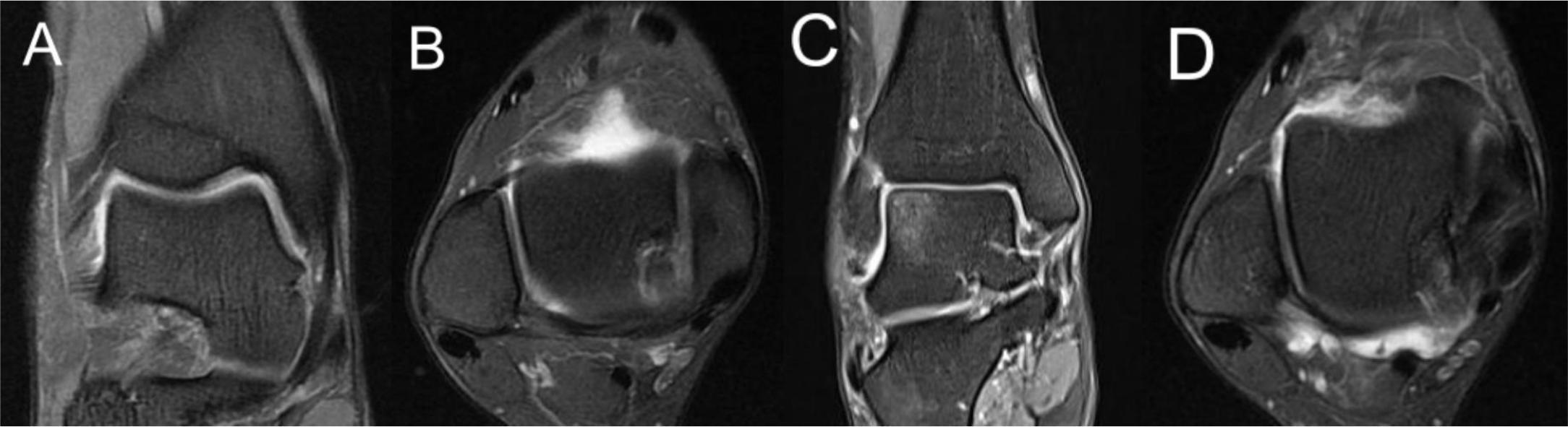
Figure 1. (A) The coronal oblique plane was prescribed for the DF-AITFL (arrow) using standard axial planes parallel to the AITFL (arrowhead). (B) The axial oblique plane was prescribed using coronal oblique planes parallel to the AITFL. The DF-AITFL was in contact with the anterolateral dome of the talus. Abnormal findings, including bone edema (asterisk) (C) and cartilage abnormalities (circle) (D) related to DF-AITFL were evaluated by MRI.