
Abstract
This is a visual representation of the abstract.
Keywords
Introduction
Infectious tenosynovitis most commonly affects the flexor tendons of the hand. Very few cases of infectious peroneal tenosynovitis (PTS) have been documented, with the majority involving mycobacteria or fungi.1,2,4 -6,8,10 Bacteria were the causal pathogen in only 2 published cases. Brown and Miller 1996 3 described a 17-year-old girl who presented with peroneal tenosynovitis following an endocervical gonococcal infection. Another case report by Schade et al 9 reported septic peroneal tenosynovitis caused by Staphylococcus aureus in an active-duty soldier who had recently undergone lateral ankle ligament reconstruction. According to a review of published vignettes using the query terms (peroneal tenosynovitis) AND ((bacterial) OR (tuberculoid) OR (tuberculous) OR (fungal) OR (histoplasma)) in PubMed, infectious peroneal tenosynovitis often presents as pain and swelling of the lateral ankle (Table 1). Most patients make a complete recovery following antimicrobial administration, and in some cases, surgical intervention. In this report, we detail a rare case of idiopathic bacterial PTS.
Review of Patient Characteristics, Diagnostic Tests, Treatment Options, and Outcomes for Reported Clinical Cases of Infectious Peroneal Tenosynovitis, Sorted by Causal Pathogen.

Abbreviations: I&D, irrigation and debridement; MRI, magnetic resonance imaging; PTA, prior to admission: TB, tuberculosis.
Case Report
Our case involves a 44-year-old woman with a medical history of rheumatoid arthritis (RA), congestive heart failure (CHF), hypertension, and tobacco use disorder. At presentation, her RA was being managed with methotrexate and adalimumab, with prednisone for flare-ups. She reported a 2-day history of right ankle pain and swelling without recent trauma or prior surgery to the ankle. Initial medical workup suggested a CHF flare, so she was admitted to the hospitalist service. The following day, laboratory results raised concern for infection, with a white blood cell count of 12.1 10e3/µL (reference range: 3.5-11.0 10e3/µL), erythrocyte sedimentation rate of 96 mm/h (reference range: 0-35 mm/h), and a c-reactive protein level of 48 mg/L (reference range: <5 mg/L). Radiographs of the right ankle demonstrated mild degenerative changes of the ankle joint without other osseous abnormalities (Figure 1). The inpatient rheumatology service suspected septic arthritis and recommended orthopaedic consultation. On orthopaedic examination, the patient had significant pain on range of motion of the right ankle. Swelling, tenderness, and erythema were noted diffusely about the ankle but appeared to be concentrated posterolaterally (Figure 2). Right ankle arthrocentesis yielded 2 mL of sanguineous fluid with 67.0% neutrophils, 8.0% lymphocytes, and 25% macrophages. No birefringent crystals were seen, and there was no growth on cultures. The sample clotted off and total nucleated cell counts were unable to be performed. At this point, the orthopaedic team had low suspicion for a septic joint based on the clinical examination and appearance of fluid on arthrocentesis. However, the patient was started on empiric vancomycin by the primary team because of their concern for septic arthritis vs cellulitis.

Anterior-posterior and lateral radiographs of the right ankle (second day of hospitalization) demonstrating mild arthritic changes without other osseous abnormalities.

Clinical picture demonstrating swelling and erythema of the patient’s lateral right ankle, the fourth day of her hospitalization.
Two days later, the patient continued to endorse lateral ankle pain, with no improvement in swelling or erythema. An additional arthrocentesis yielded another 2 mL of sanguineous fluid with total nucleated cell count of 18,000, 815,000 red blood cells, and 61% neutrophils. Again, there were no birefringent crystals and no growth seen on cultures. Thus, a septic arthritis diagnosis was deemed to be unlikely and the orthopaedic team recommended potential antibiotic treatment because of concern for cellulitis. The patient was subsequently transitioned from vancomycin to cefazolin.
Because of persistence of symptoms and the suspicion for peroneal tendon area pathology based on physical examination, MRI of the right ankle with and without contrast was obtained. Results were notable for signal hyperintensity near the peroneal tendon sheath with associated tenosynovial thickening and a peripherally enhancing fluid collection within the tenosynovium (Figure 3). This constellation of findings was suspicious for an infectious process within the tenosynovium of the peroneal tendon. Musculoskeletal radiology was consulted and performed an ultrasound-guided aspiration of the peroneal tendon sheath (Figure 4). 1 mL of serosanguinous fluid was obtained and, interestingly, this sample also clotted. Results demonstrated 88.0% neutrophils with no evidence of birefringent crystals. One week later, cultures from the ultrasound-guided aspiration yielded methicillin-sensitive S aureus (only seen in broth, amount not specified). However, culture data were not available at the time.
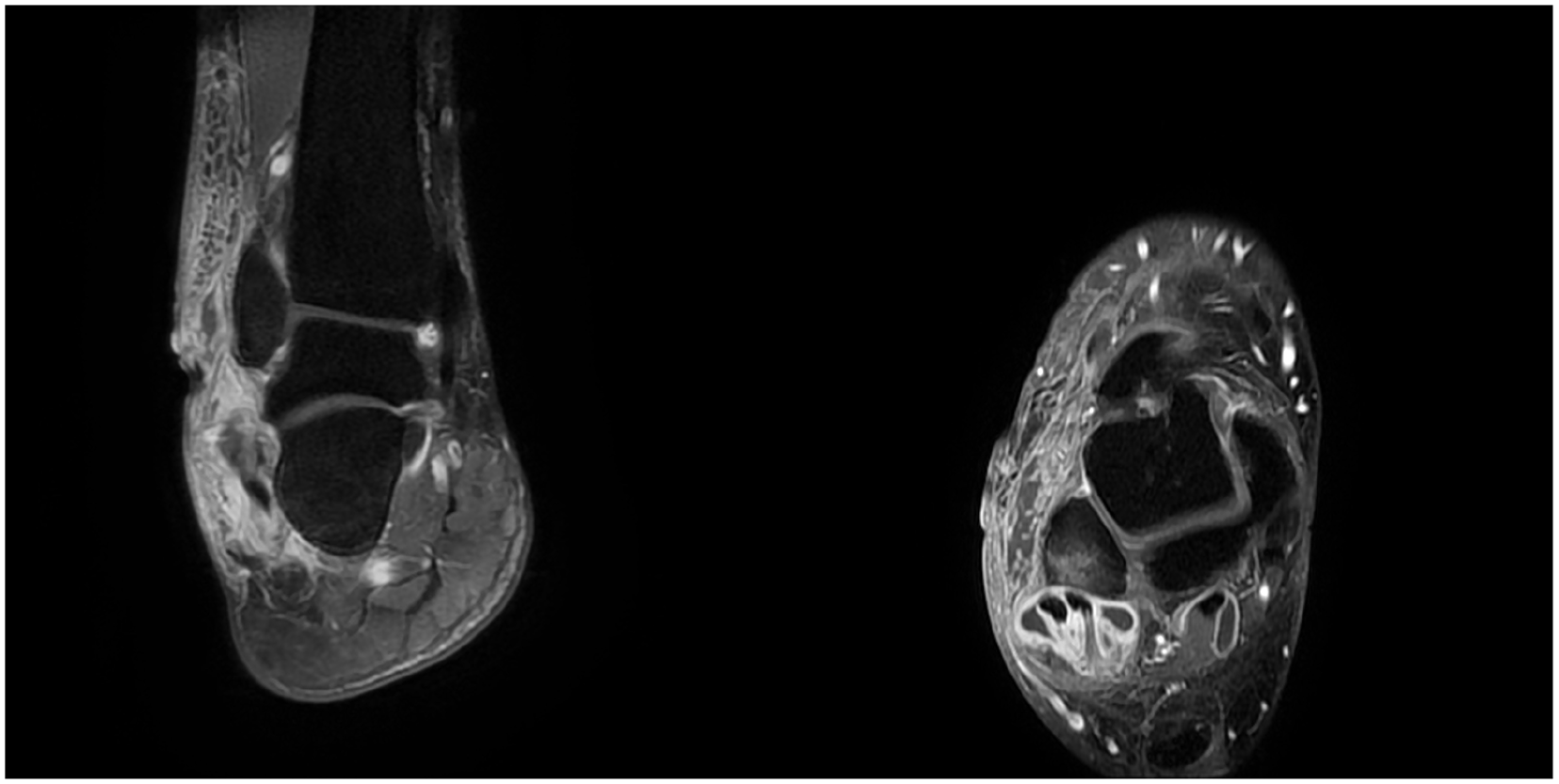
Axial and coronal images from T1 postcontrast magnetic resonance imaging on the fifth day of her hospitalization. The images demonstrate tenosynovitis of the peroneus longus, peroneus brevis, flexor hallucis longus, and tibialis posterior tendons with fluid collection and peripheral enhancement.

Ultrasonographic image depicting ultrasound-guided aspiration of fluid from the right peroneal tendon sheath.
Because of MRI findings and persistence of symptoms despite antibiotic therapy, operative irrigation and debridement of the tendon sheath was performed. Approximately 7 mL of purulent material was drained from within the tendon sheath. Thickened and diseased tenosynovium was debrided to healthy-appearing tissue. Histology revealed scarring with chronic inflammation, consistent with rheumatoid nodule-like changes. The patient was started on empiric intravenous ceftriaxone and vancomycin based on recommendations by the infectious disease team. Cultures from 3 surgical specimens ultimately grew methicillin-sensitive Staphylococcus epidermidis (only seen in broth, amount read as rare), and ceftriaxone was discontinued.
By the first postoperative day, the patient’s symptoms had greatly improved. She was discharged on postoperative day 5 with an ankle splint for use at night and when at rest. Per infectious disease, she was prescribed 1 g of oral cefalexin 3 times daily for 21 days. By final follow-up approximately 2 months after discharge, the patient was asymptomatic without evidence of recurrence.
Discussion
Peroneal tenosynovitis due to bacterial pathogens is quite uncommon. 9 In this case, the patient complained of persistent lateral ankle pain with nondiagnostic arthrocentesis and MRI. Although preoperative and intraoperative cultures demonstrated low quantities of S epidermidis and S aureus, it is not possible to attribute the case to a specific causal organism because of potential eradication of the pathogen by the patient’s antibiotic therapy. However, the finding of purulent discharge during tenosynovectomy strongly suggests a bacterial etiology as the source of the patient’s tenosynovitis.
Prior literature has established an association between RA flares and PTS.7,11 Consequently, it is possible that this patient’s tenosynovitis may have been related to her preexisting RA, which had been affecting her ankles bilaterally for months. However, tenosynovitis associated with RA and other autoimmune diseases is generally noninfectious, unlike in this case. Notably, the patient had been taking immunosuppressant medications for her RA with recent increases in prednisone and methotrexate dosages. The combination of a baseline inflamed synovium and immunosuppression may have created an opportunistic environment for infection.
The eventual diagnosis was contingent on the decision to order MRI after 2 negative arthrocentesis. This was a result of the care team maintaining heightened concern for infection because of the persistence of symptoms. Literature on infectious PTS demonstrates that in many other cases, the choice to pursue MRI has also been a central step in discerning the diagnosis (Table 1). The role of aspiration in guiding decision making remains unclear.
Although no high-quality studies or practice management guidelines exist to direct the treatment of pyogenic PTS, review of prior reports demonstrates consistent patterns. Cases of bacterial PTS have been treated surgically with tenosynovectomies and/or debridements followed by antimicrobial therapy (Table 1). We report a case that was managed successfully with tenosynovectomy and operative irrigation and debridement of the peroneal tendon sheath in addition to antibiotic therapy with intravenous vancomycin followed by oral cefalexin, in alignment with reviewed literature. Given the sparsity of literature on this condition, it is unclear whether other management options could pose benefits for patients with bacterial PTS.
Conclusion
Bacterial PTS is a rare, yet possible, cause of lateral ankle pain. In patients with persistent symptoms and negative ankle arthrocentesis, PTS may be considered to guide decision making surrounding advanced imaging, antibiotic administration, and surgical intervention.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241303933 – Supplemental material for Idiopathic Bacterial Peroneal Tenosynovitis: A Case Report and Literature Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114241303933 for Idiopathic Bacterial Peroneal Tenosynovitis: A Case Report and Literature Review by Tanios Dagher, Douglas J. Weaver and Kelly Hynes in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series. Verbal informed consent was obtained from the patient for her anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.