
Abstract
Background:
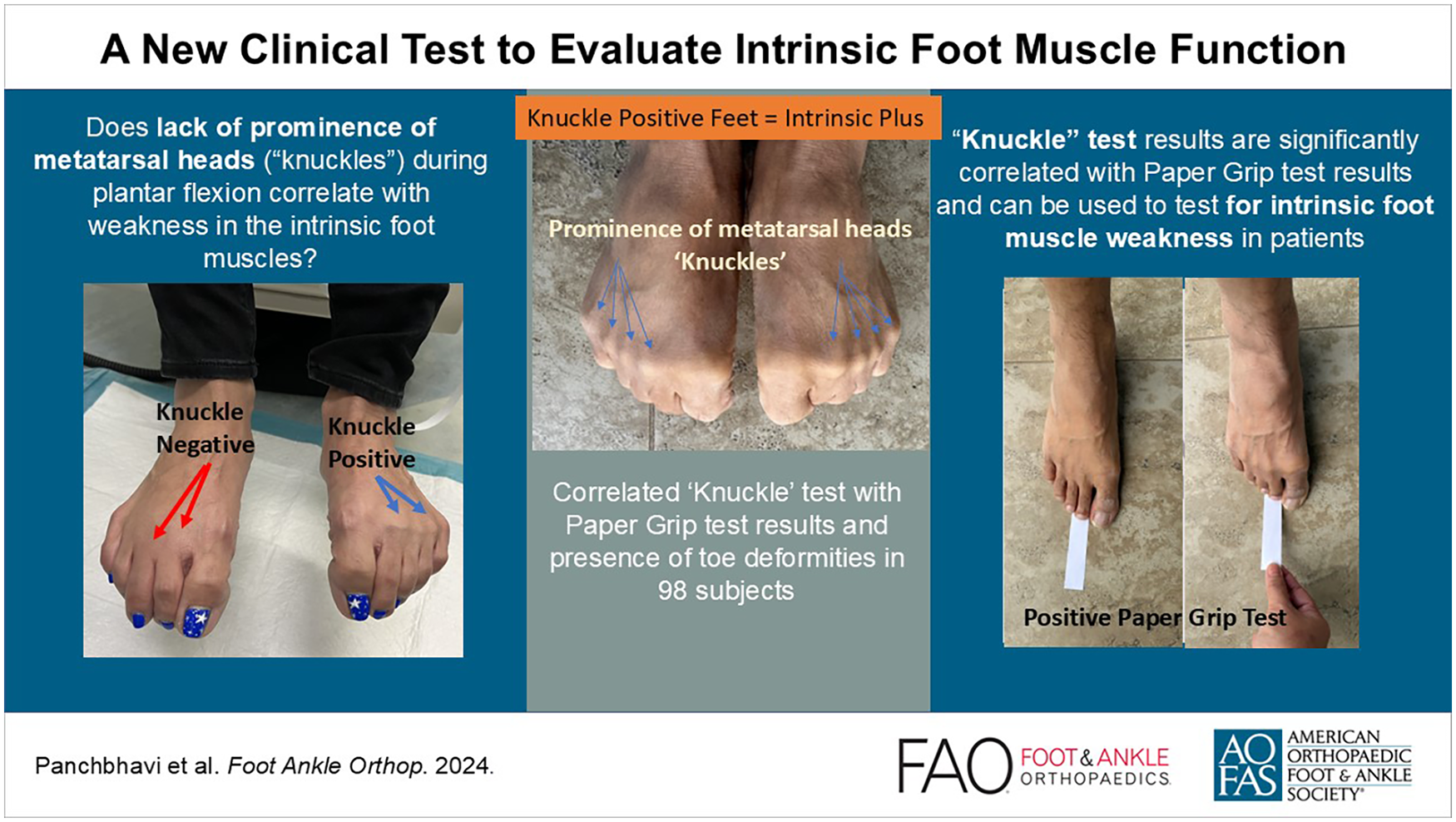
Intrinsic foot muscle weakness has been implicated in a wide range of forefoot conditions and is typically measured by the paper grip test. The proposed “knuckle test” is intended to evaluate intrinsic foot muscle function, in which active flexion of toes makes the metatarsal heads (“knuckles”) prominent in the forefoot. This study seeks to compare prevalence of negative knuckle test results and intrinsic muscle weakness in patients, primarily by association with a positive paper grip test result and secondarily with presence of toe deformities.
Methods:
Ninety-eight patients, 55 with toe deformity and 43 without, were evaluated for ability to flex their toes to the extent of knuckle prominence (knuckle test) and grip paper on the ground with their toes (paper grip test). Variables were compared between those with positive and negative knuckle test results.
Results:
A negative knuckle test result is significantly associated with the inability to grip a paper strip (P < .05).
Conclusion:
Given that the paper grip test outcomes are a well-established sign of intrinsic muscle weakness, the significant association between knuckle and paper grip test outcomes substantiates the use of the knuckle test to detect intrinsic muscle weakness. The knuckle test is a potentially quick, simple, and cost-effective clinical maneuver to indicate intrinsic foot muscle weakness in a patient.
Level of Evidence:
Level III, diagnostic test development.
Introduction
Weakness of the intrinsic muscles of the foot contributes to an imbalance between the flexor and extensor muscles and has consequently been implicated in a wide range of problems in patients, including the development of plantar heel pain,8,12 chronic ankle instability,4,12 lesser toe deformities,7,12 hallux valgus,12,13 and increased fall risks.5,10
The paper grip test, originally established by de Win et al, 2 was used to measure intrinsic muscle weakness in leprosy patients. Electromyography confirmed the activity of the intrinsic muscles during the test. The paper grip test demonstrates a high interrater (intraclass correlation coefficient [ICC] 0.87) and intrarater reliability (ICC 0.56)2,12 and has consequently been used as a general measure of intrinsic muscle weakness in successive studies.2,10
Active flexion of the toes makes the metatarsal heads, or “knuckles,” visibly prominent on the dorsum of the forefoot, and this activity can be used as a clinical test to evaluate intrinsic muscle function. The objective of this study is to evaluate the proposed “knuckle” test, wherein the inability to make the knuckles prominent in the forefoot is associated with intrinsic muscle weakness, determined primarily by a positive paper grip test result and secondarily by the presence of toe deformities. The authors hypothesize that a negative knuckle test result, or the inability to actively plantar flex the metatarsophalangeal joint (MTPJ), will be associated with intrinsic muscle weakness and/or the presence of toe deformities in patients.
Methods
Between January 2019 and January 2020, the authors prospectively observed 55 patients with forefoot pain and some element of lesser MTPJ deformity, instability, or both. Forty-three patients with no forefoot pain or MTPJ deformity were also observed as a control group. Exclusion criteria for participants included patients younger than 18 years; patients who had prior surgery involving the toe, forefoot, or midfoot; patients with toe ulcers, foot infections, diabetic neuropathy, or Charcot neuroarthropathy; and patients with general or systemic musculoskeletal or neurologic conditions such as inflammatory disorders, stroke, traumatic brain injury, or cerebral palsy. This study design received ethical approval from the study institution’s Institutional Review Board.
Patients completed a short survey to identify factors associated with plantar plate injuries: body mass index (BMI), gender, age, smoking history, diabetes, sports history, injury history, frequency and history of immobilization boot wear, hyperflexibility, and collagen disorders. Patients underwent a physical examination, and data were collected on the following variables: findings of plantar plate injury, MTPJ swelling, presence of toe deformities (V sign, floating toe, hammer toe, crossover toe, etc), hyperflexibility, supination, pronation, forefoot pain, or forefoot swelling. Toe deformities evaluated for this study included hammer toes, hallux valgus, hallux rigidus, crossover toes, bunionette, claw toes, and mallet toes. There were 2 observers, one being a board-certified orthopaedic surgeon with fellowship training in foot and ankle surgery. The tests performed included the knuckle test, MTPJ drawer test, and the paper grip test.
In the paper grip test, a strip of paper is placed underneath the patient’s toe. When the patient plantar flexes the digit, the examiner pulls the paper strip from beneath the toe. A positive result occurs when there is no digital purchase on the ground, and therefore no tear in the paper. Therefore, in this study, a positive result on the paper grip test is indicative of intrinsic muscle weakness.
A positive knuckle test result was defined as visible appearance of metatarsal heads when the patient is actively flexing the MTPJ (Figure 1). A negative knuckle test result was defined as the converse: when the “knuckles” were not visibly prominent when the patient is actively flexing the MTPJ.

A depiction of positive and negative knuckle test results.
Continuous variables were summarized by means and SDs and categorical data with frequencies and proportions. Continuous and categorical variables were compared between those with positive and negative paper grip tests using Student t test and Fisher exact test, respectively. Any variables significant on bivariate analysis were included in a multivariate logistic regression. A similar analysis was carried out for presence of deformities.
Results
The total sample size comprised 98 individuals, with a mean age of 42.6 years (SD = 19.95). Participants were additionally characterized based on the presence of toe deformities; 21% (n = 9) of male participants and 50% (n = 28) of female participants had deformities. Overall, 79% (n = 33) of male participants and 50% (n = 28) of female participants did not have toe deformities.
A positive paper grip test result was observed in 19% of participants, whereas 79% of participants had a negative paper grip test result. Bivariate analysis of paper grip test outcomes, detailed in Table 1, revealed significant associations with age (P < .00001) and sex (P < .05). Knuckle test outcomes were significantly associated with paper grip test outcomes (P < .001).
Bivariate Analysis of Paper Grip Test Outcomes.

Any significant variables found in bivariate analysis were included in the multivariate analysis of paper grip test outcomes (Table 2). With every year increase in age, patients were 1.087 times likelier to have a positive paper grip test result (P < .001). Women were 2.246 times likelier to have a positive paper grip test result (P < .05). Finally, patients with a negative knuckle test result were 4.334 times likelier to have a positive paper grip test result (P < .05).
Multivariate Analysis of Paper Grip Test Outcomes.

For a secondary analysis, presence of deformities in patients were examined. Bivariate analysis of deformities in patients revealed significant associations with age (P < .001) and sex (P < .01) (Table 3). Knuckle test outcomes were significantly associated with the presence of deformities in patients (P < .05). Significant variables in the bivariate analysis were included in multivariable analysis of deformities. With every year increase in age, patients were 1.037 times likelier to have deformities (P < .01). Female patients were 2.618 times likelier to have a toe deformity (P < .05). There was no significant association between a negative knuckle test and the presence of deformities within the logistic regression model (Table 4).
Bivariate Analysis of Deformities in Patients.

Multivariate Analysis of Deformities in Patients.

Discussion
The objective of the study was to evaluate the ability of intrinsic muscles to plantar flex the metatarsophalangeal joint. The knuckles can be made prominent if the intrinsic muscle power can overcome the extrinsic muscle power. If there is abnormality that leads to spasticity in extrinsic muscles or weakness in intrinsic muscles, then the imbalance of muscle power between the extrinsic and intrinsic will lead to a negative knuckle test.
This study looked at a physical maneuver a patient can perform in the clinic that involves active flexion of the toes. Ability to fully flex the toes makes the “knuckles” prominent, and a negative knuckle test result was defined as the inability to flex the MTPJ to the point of metatarsal prominence. This inability is significantly associated with a positive paper grip test result (OR = 4.334, P < .05), indicative of a degree of intrinsic muscle weakness. A negative knuckle test result was significantly associated with the presence of deformities in bivariate analysis (P < .05) and insignificantly associated in multivariate analysis. Considering this definite association with a positive paper grip result and a trend of association with toe deformities in patients, a negative knuckle test result may be a helpful indicator in determining intrinsic muscle weakness in patients.
To substantiate an association between a negative knuckle test result and intrinsic muscle weakness, there should be an association between knuckle test results and other established signs of intrinsic muscle weakness. de Win et al 2 uses the paper grip test as a method to indicate intrinsic muscle weakness in leprosy patients. Leprosy may cause paralysis in the hands or feet, and neuropathy of the tibial nerve may increase the risk of toe deformities in patients. After blocking the tibial nerve with bupivacaine (and thereby temporarily causing weakness of intrinsic foot muscles), paper grip test results changed from negative (normal) to positive (abnormal) in both nonleprosy and leprosy patients. Menz et al 9 used the paper grip test to measure toe weakness in healthy subjects, noting that subjects with a positive paper grip result exhibited significantly reduced plantarflexion strength in greater and lesser toes. Both studies by de Win et al 2 and Menz et al 9 substantiate the validity of the paper grip test in detecting intrinsic muscle weakness. The validity of the paper grip test and a significant association between paper grip test and knuckle test results substantiates the use of the knuckle test to demonstrate intrinsic muscle weakness.
Intrinsic foot muscle weakness has been implicated in the development of toe deformities. Kimura et al 7 examined the relationship between foot deformities and neuropathy in diabetic patients, noting that neuropathic feet with claw toes have less intrinsic foot muscle volume than patients without claw toe disorder. Taş and Çetin 14 examined thickness and cross-sectional area of intrinsic foot muscles in patients with hallux valgus. In hallux valgus patients, abductor hallucis muscles and flexor digitorum brevis muscles had less cross-sectional area and were thinner than the control group. In their interpretation of this finding, the authors suggested that this decrease in size of intrinsic foot muscles negatively impacts toe stabilization, causing hallux valgus. Furthermore, in the paper grip tests performed by de Win et al, 2 patients with toe deformities were likelier to display positive paper grip test results in comparison to the control group. A trend of association between the presence of toe deformities and a negative knuckle test further substantiates its validity.
Although the causality of the relationship between toe deformities and intrinsic muscle patients have been debated, 1 toe deformities are strongly indicative of intrinsic foot muscle weakness in patients. The tendons of the extrinsic muscles have attachments in the bases of the middle and distal phalanges. When the MTPJ is in neutral or flexed position, the long extensor tendons are elongated, and the long flexor tendons are shortened. Bus et al 1 notes that the extensors have a greater mechanical advantage over the flexors at the MTPJ, and weakness in the intrinsic foot muscles exaggerates the relative strength in extrinsic muscles, leading to an extended position of the MPTJ and flexed position at the IP joints.
There are a few limitations to this study’s approach and to the knuckle test. Because of the small sample size, the authors were unable to examine the efficacy of the knuckle test in respect to individual types of toe deformities, such as hammer toes, claw toes, or mallet toes. Nevertheless, the type of toe deformity observed did not seem to affect the association between presence of a toe deformity and negative knuckle test results in patients. In many patients, partial prominence of knuckles was observed; some but not all metatarsal heads became visible during active plantar flexion of the MTPJ. A positive result on the knuckle examination was defined as the visible prominence of all “knuckles” during this motion. This is a fairly strict interpretation of a positive result and may exclude some patients with moderately weaker intrinsic muscles. There is no way to ensure that the patient is exerting all force possible during the knuckle test, giving the appearance of a negative result. Despite these limitations, however, the knuckle test presents as a quick, simple, and cost-effective clinical maneuver to indicate intrinsic foot muscle weakness in a patient.
This test supplements physical examination findings such as pain or swelling in the forefoot at the MTPJ. Stable MTPJ and competent plantar plate and capsular attachment are necessary for the intrinsic muscles to be effective plantar flexors of the MTPJ. Therefore, patients with tenderness in this joint and showing a positive Lachman test may have difficulty in making the knuckles prominent. In the initial stages of capsulitis or synovitis of the MTPJ or in patients with chronic usage of high heels leading to atrophy of the intrinsics can benefit from understanding the pathology when they can see the inability to make the knuckles prominent. Physiotherapy to regain the intrinsic muscle strength and the ability to make the knuckles prominent, may be able to reverse this and prevent further deformities related to the imbalance of muscle power between the extrinsic muscles and intrinsic muscles. In a systematic review of 13 studies, Jaffri et al 6 notes that intrinsic foot muscle exercises were found to significantly decrease navicular drop, improve balance, strength, and patient-reported outcomes for disability. Dygut and Piwowar 3 notes that restoration of the arch of the foot, aided by intrinsic foot muscle exercises, guarantees the recovery of the function of pulling forces of the foot muscles responsible for physiological alignment of the hallux, which is significant concerning conservative treatment of hallux valgus.
This study shows that the inability to make knuckles prominent can occur without the existence of toe deformities. If the clinician can detect weakness, then preventative measures, such as intrinsic foot muscle exercises, can be implemented. Furthermore, the knuckle test serves as a powerful visual motivator for patients in this condition. When patients are able to make knuckles prominent in one foot but not the other, as shown in Figure 1, it helps them understand their condition and motivates compliance with intrinsic muscle exercises. By testing for intrinsic foot muscle weakness, clinicians can discuss conservative and preventative interventions like intrinsic foot muscle exercises early on with patients, helping slow or arrest development of toe deformities.
Future studies include an investigation into outcomes of the intrinsic foot muscle exercise regime and quantifying any changes in intrinsic foot muscle volume, with use of magnetic resonance imaging to directly as described by Smith et al. 11
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241303172 – Supplemental material for A New Clinical Test to Evaluate Intrinsic Foot Muscle Function
Supplemental material, sj-pdf-1-fao-10.1177_24730114241303172 for A New Clinical Test to Evaluate Intrinsic Foot Muscle Function by Megna Panchbhavi, Michael C. Poliner, Patrick M. Finegan and Daniel C. Jupiter in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Texas Medical Branch (IRB 19-0012)).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.