
Abstract
Background:
Nitinol compression staples have been increasingly used in foot and ankle orthopaedic surgery because of simple implantation, reproducibility, and favorable biomechanical features. Compared with traditional implants (i.e., plates and screws), nitinol staple use in foot and ankle orthopaedics has not been extensively described. This systematic review aims to describe the current clinical outcomes of nitinol staple use in forefoot and midfoot surgery.
Methods:
A search was conducted using PubMed, Web of Science, and Embase. All studies that included clinical outcomes of nitinol in foot surgery were evaluated for their demographics, outcome scores, or complication rates. Biomechanical studies and studies investigating nitinol nails in the hindfoot were excluded. Two reviewers screened titles, abstracts, and full texts.
Results:
Of the 198 total articles from the search, 9 articles met the inclusion criteria. Of the 9 articles, 4 articles investigated outcomes of nitinol in the forefoot, 3 articles in the midfoot, 1 article in the forefoot and midfoot, and 1 article in the midfoot and hindfoot. This systematic review included articles that were retrospective in nature and thus subject to selection bias. The mean follow-up ranged from 6 to 35.9 months. The included studies demonstrated significantly improved postoperative visual analog scale pain score (P < .001), Ankle Osteoarthritis Scale scores (P < .001), and Foot and Ankle Ability Measure activities of daily living scores (P < .001). Of the 6 studies that report union for patients receiving purely nitinol staple constructs or nitinol staples in combination with another construct, the overall fusion rate was 94.6% and the overall complication rate was 11.25%.
Conclusion:
This systematic review demonstrates that nitinol staples in foot surgery, whether alone or in combination with another construct, can achieve an acceptable fusion rate. However, currently we found highly limited clinical study data directly comparing nitinol staples to traditional implants. The current literature is heterogenous in its discussion of nitinol staple configurations and designs.
Level of Evidence:
Level IV, Systematic Review.
Introduction
Currently, there are several techniques and constructs including plates, screws, staples, and a combination of implants for foot arthrodesis.5,11,30,31 Sustained compression across the joint and increased bone apposition are needed for effective fusion and union. 24 There has been an increase in the use of the shape memory alloy nitinol due to properties including sustained dynamic compression, ease of use, and acceptable fusion rates on radiography. 29 Nitinol is a metal alloy composed of nickel and titanium in a roughly equal ratio and has been shown to be particularly useful in creating dynamic compression over transverse fracture lines. 33
Although this technology was initially manufactured in the 1980s, the metal did not gain popularity in foot and ankle surgery until recently. 34 Initially, nitinol use was less favorable because of its complicated clinical application and lack of practicality as it required refrigeration before application in older-generation nitinol constructs. 30 However, newer-generation constructs no longer require refrigeration and arrive in a preloaded noncompressed state that gains dynamic compression once implanted in the patient. 30 Nitinol’s structure aims to allow for unloading of large amounts of stress and provide strong compression via its elasticity, which may allow for micromotion over a fracture site and improved long-term healing. 34 These same elastic properties may also enable the implant to combat deformation from weightbearing postsurgery. 10 The staples are also designed to have different numbers of legs, ranging from 2 to 4, and surgeons may opt to use a combination of nitinol implants in different configurations (orthogonal, transverse, etc) across the fusion site.
The simple implantation and reproducibility of newer-generation nitinol implants has led to increased resurgence in recent years for treatment of tarsal fractures, and various joint fusions.7,11,29 This systematic review aims to investigate the clinical performance of nitinol staples and to describe the potential advantages and disadvantages they possess to guide appropriate implant selection in foot and ankle orthopaedic surgery.
Materials and Methods
Search Strategy
The following databases were included in the electronic search strategy from database inception until November 15, 2023: PubMed, Web of Science, and Embase. Specific terms were used (“nitinol” AND “staple”). This systematic review is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1).
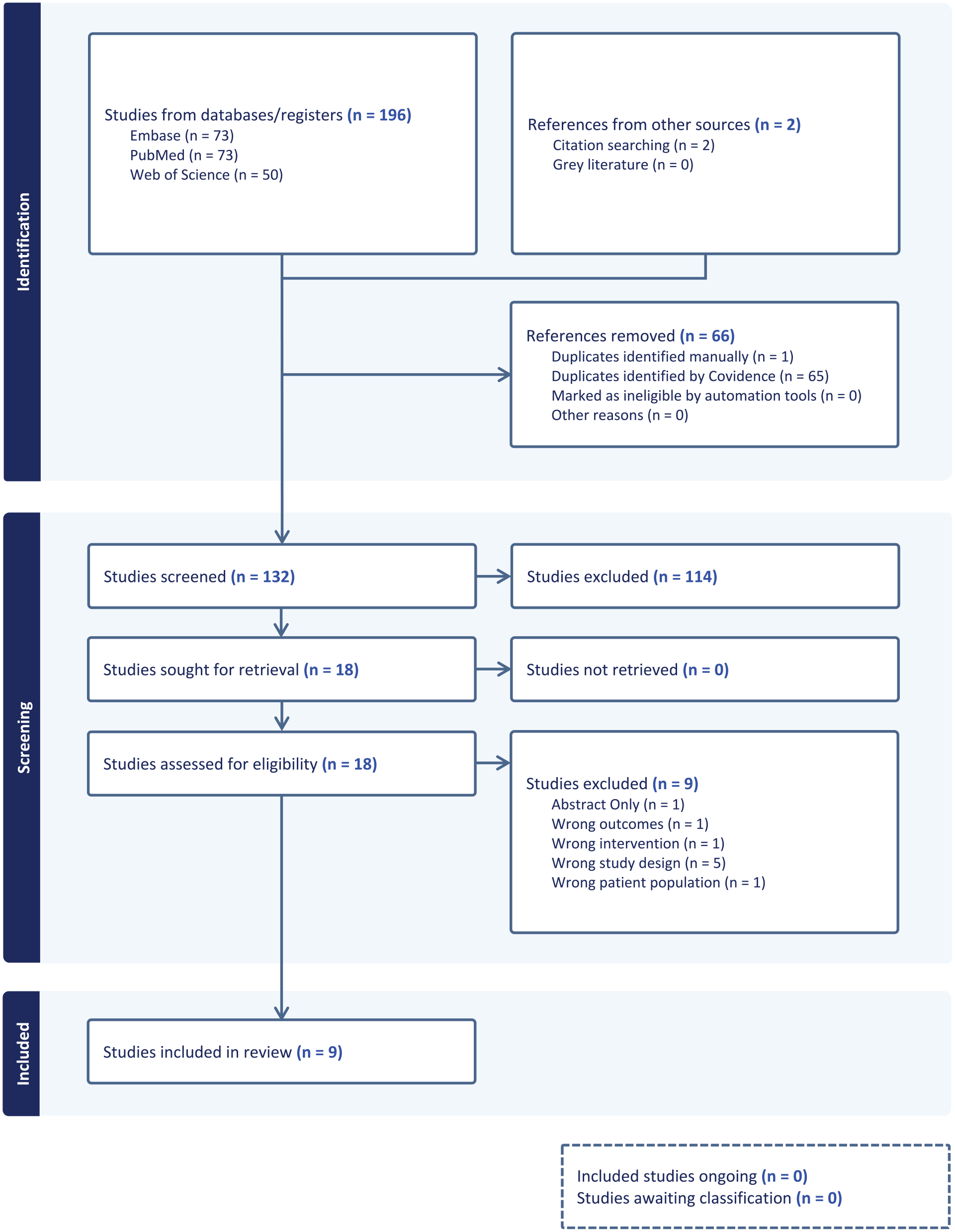
Nitinol in foot surgery.
Criteria for Study Selection
Inclusion criteria included surgical intervention with nitinol staples in foot orthopaedic surgery, full-text publications, and English language publications. Case reports with 3 or fewer cases, narrative reviews, technical notes and letters/personal opinions, and biomechanical studies were excluded. Articles addressing the use of nitinol nails in foot and ankle surgery were excluded as the focus of this analysis is nitinol staples.
Type of Outcome Measures
The following frequency outcomes were looked for in studies: union rate, revision rate, complications, or validated score measurements such as the visual analog scale (VAS) for pain and the Foot and Ankle Ability Measure activities of daily living subscale. Types of complications included broken staples, hardware discomfort, and wound infection.
Data Extraction
In preparing this systematic review, the PRISMA guidelines were used as a checklist (Figure 1). Studies were independently assessed for inclusion by 2 reviewers (A.R. and H.H.). The reviewers evaluated all identified titles and abstracts independently and excluded any articles within the exclusion criteria. The remaining articles were evaluated in full text and against the eligibility criteria. Differences between reviewers (A.R. and H.H.) were resolved by discussion to reach a consensus. Data collected include first author, year of publication, type of study (retrospective, prospective, randomized controlled trial), mean patient age, number of males/females, diagnosis at time of surgery, surgical interventions, type of nitinol staple used, complications, and mean follow-up time.
Results
Search Results
Of the 196 articles that were obtained in the original search, only 7 of those articles were included and 2 were later added, bringing the total number of screened articles to 198.7,11,15,21,25,30,32 The references were obtained for the 7 articles included from the initial search. Two additional studies by Neumann et al 23 and Dombrowsky et al 8 were included that met the search criteria and were not present in the initial search because of being a larger case series and more recently published, respectively. We obtained Neumann et al’s additional study using citation searching from one of the included studies. Our search likely missed this article due to it being labeled as a “case series” in its respective journal, even though it included 44 patients (51 feet). The Dombrowsky et al study was not included in the initial search due it being published more recently. From the extracted data, tables were constructed to show an overview of findings from each study (Table 1), postoperative course and outcomes reported in each study (Table 2), and complications reported in each study (Table 3).
Data Extraction From the 9 Included Articles in This Systematic Review.

Abbreviations: LPP, low-profile dorsal titanium locked plate; Retro, retrospective; SCP, staple compression plate; TMT, tarsometatarsal.
Unless otherwise noted, data are expressed as means.
Postoperative Course and Outcomes From the 9 Included Articles in This Systematic Review.

Abbreviations: ADL, activities of daily living subscale; AOFAS, American Orthopaedic Foot & Ankle Society; AOS, Ankle Osteoarthritis Scale; FAAM, Foot and Ankle Ability Measure; FFI-R, Foot Function Index–Revised; HVA, hallux valgus angle; IMA, intermetatarsal angle; IPA, interphalangeal angle; IQR, interquartile range; VAS, visual analog scale.
Unless otherwise noted, data are expressed as means.
Nonunions, Revisions, and Complications From the 9 Included Articles in This Systematic Review.

Characteristics of the Selected Studies
Of the studies included in this systematic review, 4 articles investigated outcomes of nitinol exclusively in forefoot procedures, 3 articles exclusively in midfoot procedures, 1 article in forefoot and midfoot, and 1 article in midfoot and hindfoot. All 9 articles were retrospective in nature. A total of 569 patients who underwent orthopaedic surgery of the foot with a type of nitinol staple implant participated in 9 studies. The mean age of the pooled sample was 55.53 years. Mereau and Ford 21 did not provide age of participants, fusion rate, or male/female gender. The type of nitinol implant used and surgical technique (single/double staple, etc.) varied between the included studies. The overall data from the studies within this systematic review could not be synthesized as a whole due to relatively high heterogeneity between the current studies on nitinol in foot surgery.
Clinical Outcomes
Tables 2 and 3 summarize the outcomes of the individual studies.
Union rate
Eight studies reported the union rate (Table 3). Neumann et al 23 reported no nonunions at final clinical follow-up (40.4 ± 15.8 weeks) or radiographic (34.6 ± 13.9) follow-up. Elattar et al 11 found no difference in clinical and radiographic union rate between a novel staple compression plate (SCP) or low-profile dorsal titanium locked plate (LPP) (95.7% vs 90.5%, respectively). Ravenell and Doh 25 reported a 94% radiographic union rate in patients with immediate weightbearing. Dombrowsky et al 8 found a greater rate of radiographic union among hybrid and staple-only constructs in comparison to plate-and-screw constructs (P = .0085). Schipper et al 30 found no significant difference in radiographic union rate between a nitinol staple-only construct or a combined nitinol staple and threaded screw construct (P = .33).
Broken implants
Four studies reported on broken staples (Table 3).7,21,25,30 Schipper et al 30 reported that in the staple-only group, of the 4 patients with nonunion, 3 had evidence of broken staples, and 3 patients who had union also had broken staples. Further, in the hybrid group, of the 3 patients with nonunion, 2 had evidence of broken staples, and 3 patients who had union also had broken staples. 30
Postoperative infection and wound dehiscence
Two studies had postoperative wound infection,23,32 and 1 study had postoperative wound dehiscence 11 (Table 3). Elattar et al 11 reported no difference between the SCP and LPP group in regard to wound dehiscence and 1 patient in each group had wound dehiscence.
Revision surgery
Eight studies reported on revision surgery (Table 3). Dombrowsky et al 8 found no difference in the rate of reoperation among a nitinol staple construct, a hybrid construct, and a plate-and-screw construct.
Hardware removal
Four studies reported instance of hardware removal (Table 3).8,15,30,32 Dombrowsky et al 8 found a higher rate of hardware removal secondary to pain in the plate-and-screw and hybrid groups in comparison to the staple-only group (P = .0127). Schipper et al 30 reported that 2 patients (3%) in the staple group underwent removal due to irritation whereas no patients in the staple and screw group underwent removal.
Outcome measures
Four studies reported preoperative and/or postoperative pain and mobility outcomes scores (Table 2).7,15,23,32 Dock et al 7 found that AOS pain and disability scores and foot and ankle ability measure scores significantly improved (P < .001). Elattar et al 11 did not report any significant difference in PROMIS scores or Foot Function Index (FFI) scores between the SCP or LPP constructs. Dock et al (P < .001), Horner et al 15 (P < .02), and Neumann et al 23 (P < .001) reported significant improvement in the VAS score postoperatively. A significant reduction in the hallux valgus angle postoperatively was seen in both Neumann et al (P < .001) and Elattar et al. The intermetatarsal and interphalangeal angles also significantly improved postoperatively in the Neumann et al study (P < .001).
Postoperative course
Six studies reported on the postoperative course (Table 2).7,11,23,25,30,33 Elattar et al, 11 Ravenell and Doh, 25 and Neumann et al 23 reported patients who were immediately weightbearing postoperatively.
Bone graft utilization
Three studies reports use of intraoperative bone graft (Table 2).7,8,23 Dock et al 7 did not specify the number of patients who had bone graft use. Dock et al and Neumann et al 23 did not report what type of bone graft was used. Dombrowsky et al 8 reported the use of autograft, bone marrow aspirate, and orthobiologics in their 3 respective groups. Patients in the mixed construct and staple-only groups had significantly more bone graft used than the plate-and-screw group (P < .0102).
Discussion
Nitinol staple use has gained more attention recently because of the improvements in implant storage and simple use. This systematic review demonstrates that based on the current literature, nitinol staples used alone or in combination with other implants have an overall fusion rate of roughly 94.58% and complication rate of 11.25% in the 6 studies that reported nitinol-specific fusion. These outcomes are reassuring given nitinol’s simplicity in use and reduced operation and tourniquet times in comparison to traditional implants. 8 Although there are limited studies directly comparing nitinol staples to plate-and-screw implants, 8 some studies included in this systematic review were able to make comparisons that demonstrated similar outcomes of nitinol staples used either alone or in a hybrid construct to traditional implants.11,30
Although there is no consensus on the optimal arthrodesis technique for the first metatarsophalangeal joint (MTPJ), fixation with a dorsal locking plate (with or without an additional compression screw) has become the most commonly used approach.13,16,19,31 Other fixation techniques include K-wires and crossing lag screws.12,17,22 Doty et al 9 previously reported a fusion rate of 98% using a dorsal locking plate with a lag screw for first MTPJ arthrodesis. Similarly, Mann et al 18 reported a 95.24% fusion rate using a low-profile titanium locking plate with crossed Kirschner wire or a lag screw. Cichero et al 4 found a single-construct locking plate with an interfragmentary screw separately had increased nonunion in comparison to a construct combining a locking plate and interfragmentary compression screw (P = .016). Although there have been no studies directly comparing nitinol staples to other fixation methods in first MTPJ arthrodesis, Elattar et al 11 and Ravenell and Doh 25 demonstrated similar fusion rates to traditional fixation methods in their specific use of nitinol constructs. However, Elattar et al used a hybrid construct, which makes it unreasonable to attribute their fusion rate to purely nitinol. In addition, Ravenell and Doh 25 along with Besse et al 2 (99% union rate) and Choudhary et al 3 (96.7% union rate) have demonstrated acceptable union rates with immediate weightbearing post–nitinol staple arthrodesis. Further, the ability for the SCP in Elattar et al’s 11 study to have both nitinol’s inherent compression and the stability of a dorsal locked plate is favorable biomechanically and requires further clinical investigation. It would also be interesting to see comparisons between this hybrid SCP design and that of a 4-pronged staple, which would provide a similar design structure, although with different biomechanical features. 11
Thus far, biomechanical studies have demonstrated greater gap angle deformation in both adduction and dorsiflexion with nitinol staples vs screws and increased resistance to gapping.1,27 However, Schafer et al 28 also demonstrated significantly reduced numbers of cycles to failure in a biomechanical study of orthogonal nitinol staples in comparison to transarticular lag screws.
Currently, fixation with dorsal plating has been a commonly used approach in midfoot arthrodesis of the tarsometatarsal joint. Schipper et al’s 30 comparison of fixation with only nitinol staples or nitinol staples in combination with a screw demonstrated no significant difference in rates of union (P = .33) or rates of revision (P = .66). In the group fixated with a purely nitinol construct, 93.8% of patients and 95.1% of joints demonstrated radiographic union at final follow-up. 30 This is in contrast to the nitinol staple in combination with a screw group, in which 90.6% of patients and 95.7% of joints demonstrated radiographic union at final follow-up. 30 These rates of fusion are similar to those described in the literature for traditional implants; however, varying populations and surgical techniques may play a role as well. Cottom and Vora 5 previously reported use of a medial locking plate with a plantar compression screw in Lapidus arthrodesis and found 17% of patients needed hardware removal, 9% developed recurrence, and 2% had nonunion. In addition, DeVries et al 6 demonstrated that locked plates had significantly greater rates of union (98.5%) than crossed-screws (89.4%) in first tarsometatarsal arthrodesis. Menke et al 20 also reported a 90.5% rate of fusion in metatarsocuneiform (MTC) arthrodesis using a lag screw and locking plate. Most recently, Dombrowsky et al 8 demonstrated the only known study to directly compare nitinol staples alone to plates-and-screw constructs in primary arthrodesis of Lisfranc dislocations. Of the 121 patients included, 93.4% of patients and 95.7% of joints had radiographic union at final follow-up. Arthrodesis with a plate-and-screw construct was associated with significantly more nonunions in comparison to the hybrid or staple-only groups (P = .0085). In addition, plate-and-screw fixation was an independent risk factor for nonunion in comparison to staple-only fixation (P = .041). Further, there were greater rates of hardware removal for pain in the plate-and-screw and hybrid groups compared with the staple-only group (P = .0127) and longer length of operation for the plate-and-screw group in comparison to the other groups (P < .0001). These results are similar to Walsh et al’s 32 study of nitinol in Lisfranc injury that showed an average AOFAS midfoot score of 77.8 at a mean 4-year follow-up. Although Dombrowsky et al shows favorable results for nitinol staples in indicated situations, increased bone graft use, which was a positive predictor of union, was more commonly used in the staple-only and hybrid groups and there was a greater prevalence of diabetes in the plate-and-screw group. In addition, in 117 joints that had a subsequent CT scan, there was no significant difference in union between groups.
Further, there is still uncertainty regarding the use of 2-, 3-, and 4-leg nitinol staples. Hoon et al 14 found that a dual staple construct applied orthogonally greater than doubled compression compared with a single staple. Double-staple constructs have also been seen to be more than 2 times stiffer than plate constructs, possibly promoting the use of double-staple constructs over single staples when feasible. 14 In addition, both single- and double-staple models have shown roughly a 7% increase in compressive load across an osteotomy over 10 minutes in comparison to no such increase from static plate fixation. 14 In addition, Russell et al 26 noted that a double-staple construct implanted orthogonally provides better contact pressure in comparison to a single staple in a simulated Lapidus procedure. Further clinical studies investigating this are needed to understand the optimal use of nitinol staples.
The results of this analysis should be interpreted within the context of the following limitations. Only 1 of the included studies made a direct comparison between nitinol staples and traditional implants. In addition, the comparisons made in the study are generalized and seek to promote further comparisons between nitinol staples and traditional implants in both the forefoot and midfoot. In addition, there is heterogeneity among studies with respect to the nitinol constructs (number of staple legs, hybrid staple/screw, etc). This heterogeneity is further seen with the use of different postoperative courses (Table 2) and different use of graft material in each study. Furthermore, the studies in this review include multiple primary diagnoses, anatomic areas, and construct types, which make it difficult to draw any definitive conclusions at this time. Lastly, the studies included in this data set were retrospective in nature and therefore susceptible to selection bias.
Conclusion
Sustained compression from nitinol staples makes the material a plausible implant for fixation of osteotomies and joint fusions of the forefoot and midfoot. This systematic review identified acceptable clinical outcomes and fusion rates with various configurations of nitinol staples in foot surgery. The heterogenous nature of the current literature on nitinol staple use makes definitive conclusions difficult to draw. Further clinical studies should be done that compare nitinol staples to traditional implants as well as different configurations of nitinol staple constructs.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241300158 – Supplemental material for Nitinol Compression Staples in Foot Orthopaedic Surgery: A Systematic Review
Supplemental material, sj-pdf-1-fao-10.1177_24730114241300158 for Nitinol Compression Staples in Foot Orthopaedic Surgery: A Systematic Review by Akshay R. Reddy, Hailey Hampton, Wojciech K. Dzieza and R. James Toussaint in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Institutional review board (IRB) approval was not applicable given the review did not involve experimentation of human or animal subjects, and the data reviewed are public.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr R. James Toussaint is a paid consultant for Medline Industries. The other authors have not received any financial payments or other benefits from any commercial entity. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.