
Abstract
Background:
With higher incidences of ankle sprains and chronic ankle instability in women, it has been postulated that hormonal modulation and ligamentous laxity influences injury propensity. The purpose of this study is to investigate the impact of hormonal fluctuation on ankle stability and ligamentous laxity and their potential contribution to injury propensity in the female athlete.
Methods:
In November 2023, a systematic review of the MEDLINE, Embase, and Cochrane Library databases was performed following PRISMA guidelines. Articles were included if they were published after the year 2000, evaluated outcomes related to the impact of hormones on ankle stability in healthy patients, and included menstrual tracking. The following search terms were used: “(sex or gender) AND (ankle stability)” and “(hormone) AND (ankle).”
Results:
Thirteen articles were included, with 253 (76.4%) women at a weighted mean age of 21.9 ± 2.0 years (range, 20.0-25.9). Five studies evaluated postural sway and balance noting greater sway rates during ovulation compared with the follicular phase. Greater muscle tone (P < .001) was observed in the follicular phase than ovulation for the tibialis anterior, peroneus longus, and lateral gastrocnemius. Significantly higher ankle joint laxity was observed in ovulation (P = .016).
Conclusion:
This review found that during ovulation, when estrogen peaks, subjects showed impaired balance with higher postural sway rates, greater ankle joint laxity, and decreased muscle and ligamentous tone and stiffness—an indicator of laxity. An underlying hormonally mediated etiology for the increased propensity to ankle instability in the female athlete is suggested. Syncing an athlete’s workout type and intensity around menstrual cycle phase may be an advantageous strategy for injury prevention.
This is a visual representation of the abstract.
Introduction
Lateral ankle sprains are one of the most common lower extremity injuries, especially among female athletes. 1 Studies have demonstrated that 30% to 70% of those who sustain an ankle sprain subsequently develop chronic ankle instability (CAI).27,34 When measuring ankle instability in a cohort of athletes, Tanen et al 36 found that CAI was significantly more prevalent in women than men in both high school and college athletes. Given these injuries may occur more frequently in women, it has been suggested that there is a relationship between hormonal modulation and ligamentous laxity.7,16,26 For similar lower extremity injuries, such as anterior cruciate ligament (ACL) injuries, intrinsic and extrinsic risk factors for injury have been explored to explain the higher injury rate in women.29,30 One proposed intrinsic risk factor is the hormonal fluctuation in women compared with their male counterparts primarily during the menstrual cycle. 37 As the estrogen, progesterone, and luteinizing hormones cyclically rise and fall, ligament alterations occur, resulting in susceptibility in ACL injury at specific times of the menstrual cycle.11,16 This impact has been tied to impact neuromuscular control around the knee influencing propensity to injury.
In human connective tissue, a sex-related difference has been observed in the role of estrogen regulation of both muscle mass and ligamentous laxity.15,22,39 Collagen synthesis is inhibited by estrogen, resulting in increased elasticity and decreased muscle tone and stiffness, all which compound into a lax ligament.22,26,39 Estrogen levels are highest in the ovulation and midluteal phases, both of which were demonstrated to be associated with the greatest amount of knee laxity during these phases.5,22,33 Furthermore, it is believed that this contributes to a previously determined higher degree of postural sway during ovulation rather than the follicular phase. 22 The alpha and beta receptors within tendons, ligaments, and skeletal muscles modify myofascial forces and neuromuscular control during the menstrual cycle. 28 Varying estrogen levels potentially impacts the receptors and their muscular coordination properties.
Similar to the research on the ACL, literature has explored the relationship between hormonal variations and their resulting changes on mechanical and functional stability that may substantiate the likelihood of ligamentous ankle injury.3,17 There is conflicting evidence whether hormonal modulation impacts postural sway and ligamentous changes, as well as a lack of consensus on which phases of the menstrual cycle may result in more instability. To our knowledge, no systematic reviews to date have evaluated this topic thus far. The purpose of this study is to investigate the impact of hormonal fluctuation on ankle stability and ligamentous laxity and their potential contribution to injury propensity in the female athlete.
Methods
Search Strategy
In November 2023, a systematic review of the MEDLINE, Embase, and Cochrane Library databases was performed between 2000 and 2023 based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 25 The following search terms were used: “(sex or gender) AND (ankle stability)” and “(hormone) AND (ankle).” Articles were included if they evaluated outcomes related to the impact of hormones on ankle stability in healthy patients, included menstrual tracking, were peer-reviewed and written in English, had a minimum of 5 patients per cohort, and were published after the year 2000. Studies with a male control group were included and evaluated, although this was not a requirement for inclusion. Articles were excluded if they evaluated patients who were injured or experiencing other associated pathologic processes impacting ankle function or stability. Additionally excluded were systematic reviews, case studies, conference abstracts, as well as animal, pediatric, or cadaveric studies. Titles, abstracts, and full-text articles were screened by 2 independent reviewers. If there were any disagreements, a senior author determined the final resolution. Because of the nature of the study design, this study was exempt from ethical and institutional review board approval.
Assessment of Level of Evidence and Methodologic Quality
Quality of clinical evidence and risk of bias for nonrandomized studies was assessed utilizing the Risk of Bias in Non-Randomized Studies-of Interventions (ROBINS-I) tool. 35 This tool evaluates 7 domains for potential bias, including study participant selection, potential confounders, missing data, reported results selection, intervention classification, deviations from described interventions, and outcome of measurement. An overall bias assessment is given in a final domain. The level of risk of bias judgments are low, moderate, serious, or critical.
Data Extraction and Evaluation
Two independent reviewers independently extracted and assessed the data from each individual study. A senior author resolved any conflicts. Patient demographic characteristics were collected, including sex, body mass index (BMI), age, cycle length, and length of subjective dysmenorrhea. Primary outcome measures included the relationship of menstrual phases and postural sway and balance testing measurements. Secondary outcome measures included tendon properties and ankle laxity. Because of the heterogeneity of studies, meta-analysis was not completed.
Results
The initial article search generated 3460 articles. Of these, 13 met the inclusion and exclusion criteria (Figure 1). Articles were composed of 8 cohort studies, 2 clinical trials, 2 case-control studies, and 1 cross-sectional study. Two-arm studies contrasted female and male control groups.

PRISMA flow diagram.
Study Characteristics and Patient Demographics
Patient demographic and study characteristic data are listed in Table 1. Five studies were level of evidence II8,11,17,20,31 and 8 studies were level of evidence III.4,10,18,22,28,32,38,39 According to the ROBINS-I classification, 5 studies were of low risk and 8 studies were of moderate risk (Figure 2).
Study Characteristics and Patient Demographics.

Abbreviations: BMI, body mass index; F, female; M, male.

ROBINS-I Bias Assessment.
Among the 13 included studies, there were 331 total participants, of which 78 (23.6%) were male and 253 (76.4%) were female. The weighted mean age for males was 23.6 ± 2.4 years (range, 21.1-27.3) and for females was 21.9 ± 2.0 years (range, 20.0-25.9). The weighted mean male body mass index (BMI) was 22.9 ± 1.8 (range, 21.7-24.3). The weighted mean female BMI was 21.4 ± 0.63 (range, 20.7-22.4). The weighted mean cycle length was 28.8 ± 2.4 days (range, 23.3-31.1). Similarly, the weighted mean time for subjective dysmenorrhea was 3.9 ± 0.89 days (range, 3.0-4.9).
Protocol
Menstruation tracking was performed through a variety of methods, including 6 months of self-monitoring,4,17 up to 3 months of self-monitoring,11,22,28,32,39 and use of basal body temperature.8,38 Digital ovulation tests were additionally used by 8 studies.8,10,11,17,18,22,38,39 All 13 studies collected data in the follicular and ovulation phases. Additionally, 5 studies collected data from the luteal phase.4,8,32,33,38
Postural Sway and Balance
Seven studies evaluated postural sway and balance properties, testing neuromuscular control of the ankle muscles using various balance station tasks (Table 2).10,17,20,22,28,32,39 Two studies noted that the tibialis anterior / peroneus longus (TA/PL) ratio was significantly higher in ovulating women than that in follicular phase women and male counterparts.17,22 As the balance tests increased in difficulty, this ratio significantly increased in ovulating women; however, the same increase was not observed in follicular phase women and men (P < .05). For the least difficult balance tests, no significant differences were observed between ovulation and follicular phase groups.17,20,22,28,39 In the 3 most difficult balance tests, 5 studies demonstrated significantly greater postural sway rates in ovulating women than both follicular phase women and men.17,20,22,28,39
Postural Sway and Balance.

Abbreviations: Fol; follicular; LG, lateral gastrocnemius; Ov, ovulation; PL peroneus longus; TA, tibialis anterior.
Limb dominance was evaluated by 1 study, noting that the participants had longer completion of Y-balance (P < .001) and standing length (P < .001) during the ovulation phase than the follicular phase. 10
Tendon Properties
Seven studies evaluated tendon and fascial properties.4,17,20,22,28,31,39 Three studies assessed muscle tone (Table 3).17,22,39 There was significantly greater muscle tone in the PL and TA in men than ovulation (P = .001) and follicular phase women (P = .01). 17 Similarly, greater elasticity in the TA was observed in men compared to follicular and ovulation phase women (P = .001). 17 Lee et al 21 noted greater TA muscle activity in the ovulation phase, whereas greater PL activity was noted in the follicular phase. Yim et al 39 noted greater muscle tone (P < .01) and lower elasticity (P < .05) in follicular phase than ovulation for the lateral gastrocnemius (LG). The PL demonstrated no differences in elasticity, but greater tone in follicular phase (P < .01). For the TA, elasticity was significantly lower in ovulating women (P < .05), although follicular phase women had a significantly greater stiffness and tone (P < .001). 39
Tendon Properties.
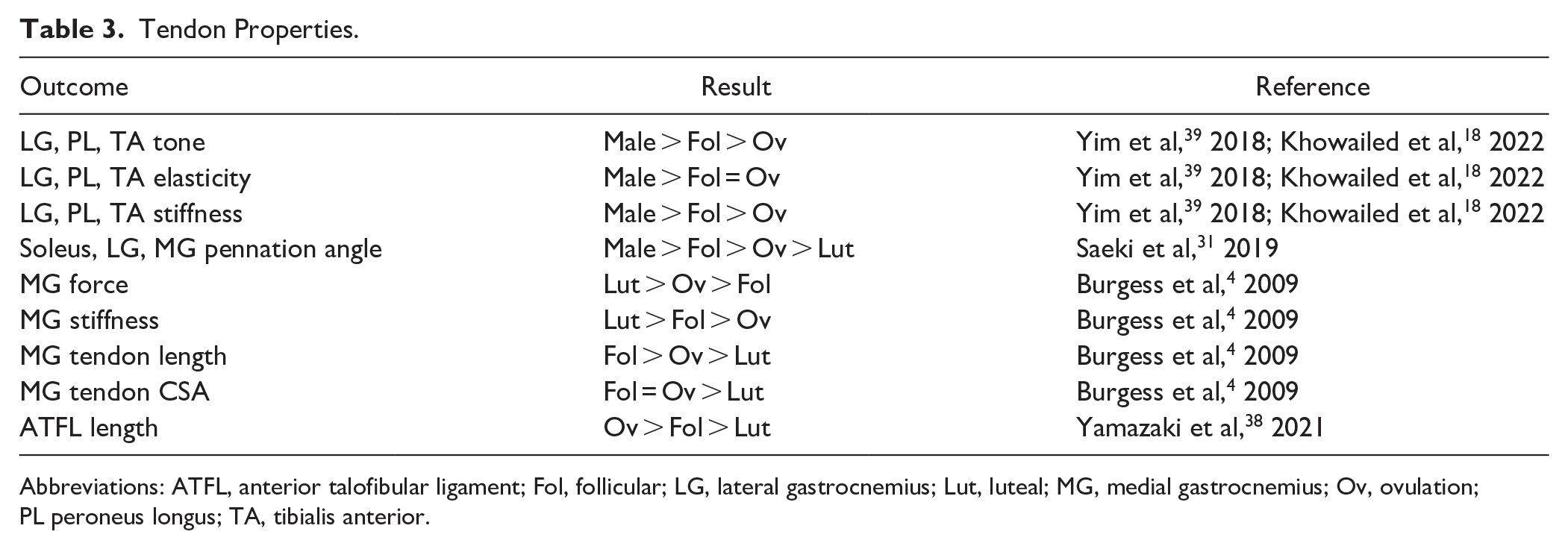
Abbreviations: ATFL, anterior talofibular ligament; Fol, follicular; LG, lateral gastrocnemius; Lut, luteal; MG, medial gastrocnemius; Ov, ovulation; PL peroneus longus; TA, tibialis anterior.
Two studies evaluated stiffness.4,31 Greater passive stiffness was observed in the soleus, MG, and LG in men compared to women, noting no impact on the menstrual cycle (P < .01). Soleus active muscle stiffness was greater in each menstrual cycle phase than men (P < .01). 31 Burgess et al 4 determined that although the MG showed lowest stiffness during ovulation and highest during follicular phases, there were no significant correlations between menstrual phase and stiffness properties.
Two studies evaluated foot length and plantar fascia properties.20,28 Greater foot length changes were observed in ovulating women than follicular phase women or men.20,28 Lee and Petrofsky 20 found greater plantar fascia length and thickness in ovulating women than men (P < .001).
Laxity
Two studies investigated joint laxity.11,38 Yamazaki et al 38 found that a significantly higher ankle general joint laxity score in the ovulation (P = .016) and luteal (P = .026) phases compared with the follicular phase, noting a significant number of ankle joints positive for laxity (P = .001). Greater ankle joint laxity was observed in women than men (P = .002), despite no impact on the ovulation cycle. 11
Discussion
The purpose of this study was to evaluate the impact of hormonal fluctuation on ankle stability and ligamentous laxity. This study’s main finding was that balance, postural stability, and ligamentous laxity especially in the ankle joint fluctuates throughout the menstrual cycle and between genders. The ovulation phase demonstrated greater postural sway rates, elasticity, and ankle joint laxity, as well as decreased tone and stiffness indicating that this phase may exhibit impaired balance and increased laxity. Ankle joint laxity was observed to be greater in women than men, with mixed results as to the impact of the menstrual cycle on these properties.
Although it is known that female athletes have a higher incidence of ankle injuries, the underlying contributing factors have yet to be fully determined. It has been postulated that neuromuscular control and hormonal fluctuations are linked, which was explored in the quadriceps muscle, noting that decreased quadriceps control for knee joint laxity during ovulation likely attributed to increased estrogen concentration.17,19,29 Studies in the current systematic review similarly explored the relationship of balance properties with ankle stabilization muscles, consistently finding greater postural sway rates in ovulating women than both those in follicular phase and control group men.17,20,22,28,39 Interestingly, no differences were found in the least difficult balance tests; however, as the difficulty increased, significant differences were observed in the TA/PL ratio.17,22 Additionally, the TA was more heavily relied on for neuromuscular activation during ovulation than the follicular phase, as increased TA activation may compensate for the greater postural sway rates and higher ankle laxity. 22 The underlying mechanism of these results can likely be attributed to the peaked levels of 17-β estradiol during ovulation compared with that of the follicular phase, which holds the lowest levels of estradiol.1,17,19 -21,40 With decreased balance properties, less motor control, and higher postural sway rates during the ovulation phase, the findings of this study indicate that it may be advantageous for female athletes to be cognizant of exercise requiring significant ankle proprioception and control during ovulation, particularly following an ankle sprain or those with chronic ankle instability.
Like postural sway and balance properties, tendon and muscular properties varied across men and as hormonal cycle fluctuated. Men had greater tone, elasticity, pennation angle, and tendon stiffness than women.11,18,31,39 However, follicular phase women proved to be superior to ovulating women in these metrics for the TA, PL, and gastrocnemius, although results varied depending on methodology.4,18,31,39 Muscles with larger pennation angles often exhibit higher stiffness because a greater amount of fibers contribute to increasing tension and force generation during contraction. 31 Interestingly, although tone and elasticity were not inversely related in all muscle properties, this was observed in ankle-stabilizing muscles, noting tone and stiffness to be lesser in ovulation and elasticity to be greater. Lower PL activity coupled with higher TA activity to account for the ankle laxity during ovulation affected by higher estrogen concentrations supports the findings of higher TA/PL coactivation ratio, greater postural sway, as well as reduced muscle tone and stiffness during ovulation.17,22,39 Estrogen has been shown to decrease collagen synthesis and increase its degradation as greater estrogen concentrations may result in decreased tendon stiffness and may have a negative impact on muscle force generation.4,12,24 However, this has not been shown to have an impact on muscle strength as both the existing literature and studies included in the current systematic review support that the menstrual cycle did not impact muscle strength.4,6,9,14 Plantar fascia length and thickness, as well as foot length were additionally assessed in this study. When load was applied, the plantar fascia experienced greater thinning and increased foot lengthening during ovulation than menstruation.20,28 A striking, nearly 50%, increase in foot length per kilogram body weight and 40% less plantar fascia thickness was noted during ovulation compared with menstruation. 28 The authors likened this to greater elasticity, as their methodology was based off of a previous study that had demonstrated greater laxity in the plantar fascia for women in both static and dynamic conditions but that, however, had not evaluated menstrual impacts.13,20 With greater elasticity, it is expected for increased balance impairment during the ovulation phase. These findings demonstrate that the connective tissues in the foot impacted by estrogen levels with significant changes in function, properties, and proprioception throughout phases of the menstrual cycle. Specific future evaluation of 17-β estradiol receptors in relation to the menstrual cycle is required to further elicit greater understanding of this phenomenon.
Although postural sway and tendon properties are expected to indicate greater laxity in the ankle, 2 studies specifically evaluated ankle joint laxity. Ericksen and Gribble 11 observed higher laxity in women than men, finding no significant differences in menstrual cycle. On the contrary, Yamazaki et al 38 found higher laxity in ovulation and luteal phases than in follicular phases. They noted that although previous reports have shown estrogen receptors to be in the plantar fascia, it is unknown whether similar receptors are found in the anterior talofibular ligament. The authors suggested that women may be more sensitive to estrogen effects in the anterior talofibular ligament during the ovulation phases, resulting in a causative factor for the higher propensity for ankle sprains in women.28,38 A limitation of the study by Ericksen and Gribble 11 is that their methodology simply evaluated preovulatory compared to postovulatory limiting variance in estrogen levels and potentially limiting their overall conclusion that fluctuations in the menstrual cycle were not present. Greater ligamentous laxity in the ankle can result in greater postural sway, which has been demonstrated by this study’s findings and prior literature.15,17,21,22,28,39 It is possible that this may be due to a mechanical lag in muscle activation because of variances in tension at the ankle joint. 39 Another consideration to be made is the impact of tissue temperature as it has been shown that greater concentrations of estrogen increase the tendon and ligament temperature during ovulation, increasing laxity and relaxation.28,39 A study by Lee et al21,39 stabilized leg temperature throughout the menstrual cycle, noting that estrogen impacted tendon laxity, although to a lesser extent, suggesting that these tissue changes observed in women are multifactorial because of cyclic changes caused by downstream effects of estrogen.
Understanding the underlying pathophysiology and biomechanics for the increased incidence of ankle sprains and CAI in female athletes is a crucial first step to treating the female athlete. However, beyond this, it is increasingly important to apply these principles to injury treatment and prevention. The results in this study demonstrate that during ovulation when estrogen levels are highest in the body, balance is low, postural sway is high, and ligamentous laxity is increased. More flexible and compliant tendon structures may have lower performance especially during activities requiring higher or more rapid force generation, resulting in decreased capacity to offset diminished stability. 4 The concept of “cycle syncing” is one that has gained traction both in the popular culture and medical spaces, with a current 544.9 million views on TikTok. 2 This concept bases the intensity level of workouts around the phase of the menstrual cycle. Primary literature on this topic is minimal and of low quality of evidence, with early data suggesting that there is potential that exercise performance may be minimally reduced during the early follicular phase. 23 Rather than fully adopting this “trend,” the current study’s results suggest that it may be advantageous for athletes to avoid high-intensity activity during ovulation (Figure 3). This would include activity that requires high-capacity force generation, plyometrics, uneven terrain, or sudden stopping or change of direction—all mechanisms that can increase risk for ankle sprain or reinjury in those with CAI. Further research is required on this topic to evaluate if this is an effective injury prevention strategy in the female athlete. This may include prospective studies tracking athlete menstrual cycle and injury incidence, as well as a randomized study comparing athlete injury propensity when using a “cycle syncing” strategy vs those who do not. Understanding the role of this as a true training and injury prevention tool is necessary to transition this from a popular culture trend to a validated clinical recommendation. It is additionally of value to study laxity metrics in athletes who are taking oral contraceptives and whether the same fluctuations in balance properties are seen when the menstrual cycle is artificially modulated. This would be of particular benefit if certain contraceptives were found to impact postural stability during ovulation to a lesser extent than the native menstrual cycle, therefore, suggesting that oral contraceptive pills may aid in injury prevention.

Proposed activity based on estrogen levels.
Limitations
This study is inherently limited by the included studies as they were heterogenous in nature, and all had varied methodologies limiting further cross-sectional analysis. Specifically, each study measured hormone levels slightly differently including assorted menstrual tracking, different phases of cycles, inconsistent presence of control groups, as well as inconsistent use of measurement of hormonal values. Additionally, heterogeneity was introduced by the diverse balance tests, measurement software, muscles tested, and devices used in each study. There was a lack of control for confounding variables introducing biases. This study assessed literature that was primarily level of evidence II and III, and although greater quality of evidence is not currently available in the present literature, this certainly presented a limitation for the quality and depth of conclusions to be drawn. The authors attempted to control for each of these as objectively as possible to analyze the topic in the most comprehensive manner possible. All findings are associations; causality cannot be inferred.
Conclusion
In this review we found that postural stability, balance, ligamentous laxity, and tendon properties fluctuate throughout the menstrual cycle. The ovulation phase, a state when estrogen levels peak was associated with impaired balance with higher postural sway rates, significantly greater ankle joint laxity, and decreased muscle and ligamentous tone and stiffness—an indicator of laxity. These results suggest a potential underlying hormonally mediated etiology for the increased propensity to ankle instability in the female athlete. Additionally, syncing an athlete’s workout type and intensity around menstrual cycle phase may be an advantageous strategy for injury prevention.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241300140 – Supplemental material for Hormonal Fluctuation and Ankle Instability in Women—Is There a Correlation?
Supplemental material, sj-pdf-1-fao-10.1177_24730114241300140 for Hormonal Fluctuation and Ankle Instability in Women—Is There a Correlation? by Hayden Hartman, Shannon Fehr and Arianna L. Gianakos in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study was exempt from ethical approval.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Arianna L. Gianakos, DO, reports general disclosures as a paid consultant for Arthrex, Inc., and Conmed, and is a board or committee member of the American Orthopaedic Foot & Ankle Society and the Ruth Jackson Orthopedic Society. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.