
Abstract
Background:
The impact of social health on patient-reported outcomes (PROs) is gaining increasing attention within the orthopaedic community. Few studies have explored any relationship between social deprivation levels and PROs in orthopaedic foot and ankle patients.
Methods:
We retrospectively identified patients who presented to an orthopaedic foot and ankle clinic for new evaluation. Patients completed PROs including PROMIS physical function (PF), PROMIS pain interference (PI), and the Foot and Ankle Ability Measure (FAAM). Social deprivation was measured using the Area Deprivation Index (ADI), a metric that incorporates various domains of poverty, education, housing, and employment. The ADI score quantifies the degree of social deprivation based on the 9-digit home zip code but is not a specific measure to an individual patient. Briefly, a lower ADI indicates less deprivation whereas a higher score denotes greater deprivation. Patient characteristics and outcomes were summarized and stratified by the nationally defined median ADI. Multivariable linear regression models assessed the relationships between PROs and continuous ADI controlling for demographics (age, sex, race/ethnicity, marital status, and employment status).
Results:
Our cohort consisted of 1565 patients with PRO and appropriate zip code data. Patients in the most-deprived median ADI split had more pain (median PROMIS-PI 62.7 vs 61.2, P = .001) and less function (median PROMIS-PF 37.1 vs 38.6, P = .021) compared with the least-deprived median ADI split. The clinical significance of these findings is unclear, though, given the minimal differences between groups for PROMIS measures. There was no relationship between ADI and FAAM scores.
Conclusion:
More socially deprived patients presented to the clinic with marginally less function and greater pain. Although statistically significant, the clinical significance of these relationships is unclear and merits further exploration. We plan to continue to study the connection between social deprivation and patient outcomes in specific clinical conditions as well as before/after surgical interventions.
Level of Evidence:
Level IV, retrospective cases series.
Introduction
Social deprivation is a concept that encapsulates various psychosocial and medical aspects of patient care.1,9,10,15,33,38 Greater social deprivation has been linked to poorer outcomes from an increasing number of health conditions. For example, social deprivation has been associated with increased cardiac disease, colorectal cancer, musculoskeletal pain, weight gain, and mortality rates.17,24,37,41,50,52 The Area Deprivation Index (ADI) was developed as a method to measure social deprivation based on zip code from data provided by the Health Resources & Services Administration (HRSA) and has been shown to be a good index for comparative metrics.22,26,27,40
The study of social deprivation in orthopaedic care has recently gathered interest.18,31,36,47,53 Increased levels of social deprivation have been negatively linked to outcomes from orthopaedic procedures in both pediatric and adult patients.18,23,34 Further, patients with musculoskeletal complaints from higher socially deprived areas were linked to worse baseline depression, anxiety, pain interference, and physical function.3,5,16,19,21,32,42,49,54 An examination of joint replacement patients found that increasing social deprivation correlated with worse preoperative disease severity and postoperative outcomes.6,13,25 Higher social deprivation levels have also been linked to decreasing access to care. 43 However, limited studies have analyzed patient outcomes and social deprivation in orthopaedic foot and ankle patients. 7
In this study, we retrospectively analyzed new patient visits to orthopaedic foot and ankle surgeons and compared various patient outcome metrics according to social deprivation measures based on ADI scores.26,27,40 We hypothesized that, in agreement with previous work, patients with greater social deprivation would present to clinic with greater pain and less function compared to patients with less social deprivation.
Materials and Methods
Data
Following institutional review board approval, retrospective data were collected from all new patients presenting to the University of Utah to one of 4 fellowship-trained foot and ankle surgeons. New patients completed questionnaires for the Foot and Ankle Ability Measure (FAAM) data as well as the Patient Reported Outcome Measurement Information System (PROMIS) pain interference (PI) and physical function (PF) scores as set by the guidelines of these metrics.8,30 We considered for inclusion all adults (older than 18 years) and new orthopaedic outpatient visits from 2016 to 2017. Only the first new patient visit was included if patients saw multiple providers within the study period. Patients with incomplete questionnaires, those lacking a listed address, and those with only a listed post office box were excluded. Demographic data were collected via electronic chart review.
Social deprivation scores were assigned to each patient using the 2020 ADI based on their zip code.26,27,40 Of note, ADI data have only been released in 2015, 2020, and 2022 by the Neighborhood Atlas. We selected the ADI data from 2020 to most accurately reflect our study time frame. ADI allows for ranking of neighborhoods by socioeconomic disadvantage including factors for education, housing quality, employment, and income.26,27,40 The ADI is based on a measure created by the Health Resources & Services Administration (HRSA) that places neighborhoods based on zip codes into national percentile rankings from 1 to 100 based on level of “disadvantage.” However, because ADI is not an individualized measure to each patient, the assumption is that a patient living within a zip code with a higher ADI will in fact have social deprivation (and vice versa).
Statistical Methods
We summarized categorical foot and ankle patient factors as counts with percentages, and continuous patient characteristics as means with standard deviation SD, medians with 25th and 75th percentiles (interquartile range) and range. We summarized them overall and stratified by the nationally defined median ADI (50 points). Of note, in the ADI literature, various groupings have been used including quartiles, tertiles, and quantiles. Given the imbalance in our data set (ie, far greater proportion of less socially deprived patients to more socially deprived patients), we felt that quantiles (2 groups) would be most appropriate for our analyses. 20 Continuous variables were compared with median ADI using a Wilcoxon rank sum test, and categorical variables were compared using a chi-squared test.
We used univariable and multivariable regression to examine the impact of social deprivation as measured by continuous ADI on function outcomes including the PROMIS-PF, PROMIS-PI, and FAAM. In the event of floor or ceiling effects, the Tobit model extension of linear regression was used to estimate unbiased relationships.2,48 We considered a ceiling or floor effect to be present if ≥15% of subjects had the highest or lowest possible score. 45 The multivariable models were adjusted for patient characteristics including age, sex, race and ethnicity, marital status, and employment status. We reported coefficients, 95% CIs, and P values from the models. All analyses were performed using R, version 4.1.0, with a .05 significance level using 2-tailed tests.
Results
From 2016 to 2017, there were 3101 cumulative patient visits to the 4 fellowship-trained orthopaedic foot and ankle surgeons. In total, 1536 patients were excluded. Compared with our study cohort (n = 1565), excluded patients were more likely to be male (47.6%, P < .001), unemployed (31.8%, P < .0001), and single (28.5%, P < .0001). Of the excluded patients, 726 were due to incomplete zip code information. Of those with missing zip code data, 17 were due to PO box issues. The remainder of the excluded patients (n = 810) were due to missing or incomplete outcomes data. For those excluded patients with zip code data but missing outcomes scores (n = 810), ADI scores were lower compared with our included study cohort (mean 28.2, SD 16.3, P < .001). The mean difference in ADI scores was 2.6.
Therefore, our included sample size was N = 1565. Patient characteristics can be seen in Table 1. Comparing patient characteristics between the least and most deprived areas, as determined by a nationally defined median split, we found that patients from the most deprived areas were less commonly White, non-Hispanic (77.7% vs 89.3%, P < .001), less commonly married (49.6% vs 68.1%, P < .001), and more commonly unemployed (15.6% vs 10.6%, P < .001). Furthermore, patients from the most deprived areas had greater pain (median 62.7 vs 61.2, P = .001) and reduced physical function (median 37.1 vs 38.6, P = .021) compared with those from the least-deprived areas (Table 2).
Summary of Patient Characteristics (N = 1565).
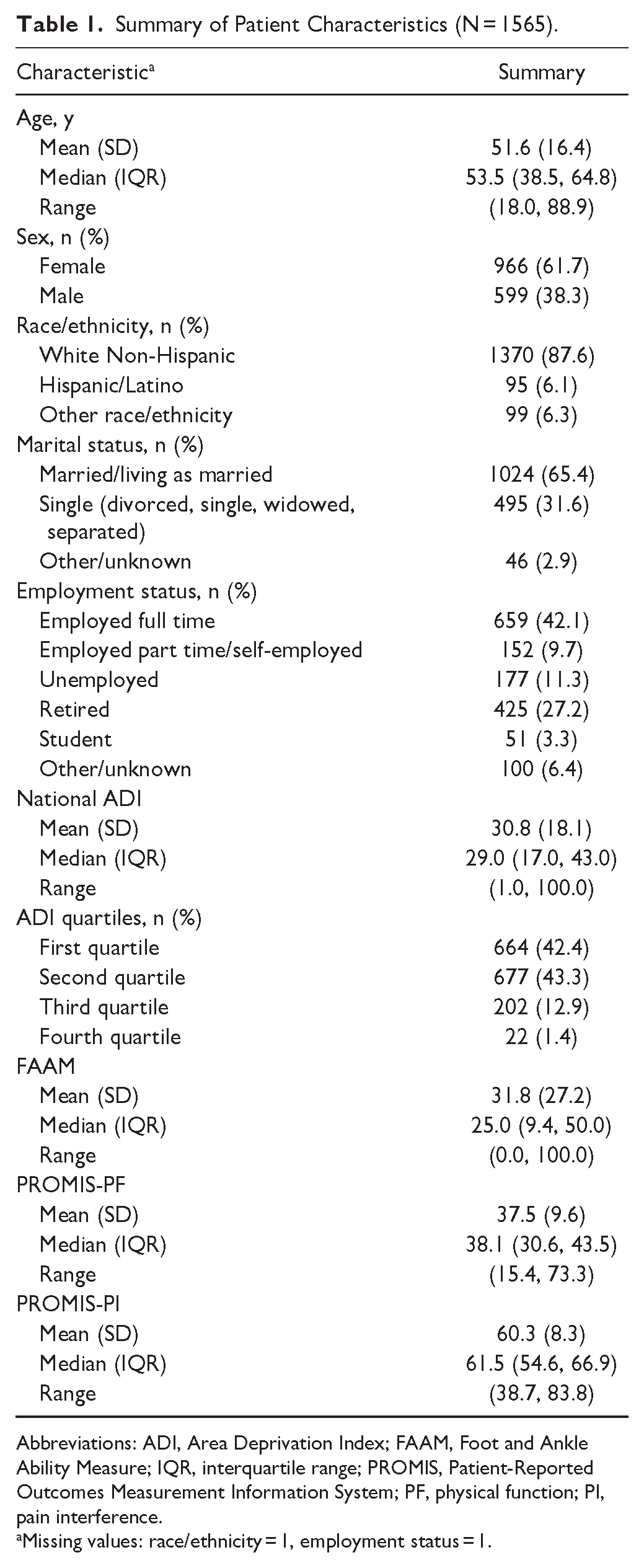
Abbreviations: ADI, Area Deprivation Index; FAAM, Foot and Ankle Ability Measure; IQR, interquartile range; PROMIS, Patient-Reported Outcomes Measurement Information System; PF, physical function; PI, pain interference.
Missing values: race/ethnicity = 1, employment status = 1.
Patient Characteristics Stratified by Least and Most Deprived Using the Nationally Defined Median Split at a Score of 50.

Abbreviations: FAAM, Foot and Ankle Ability Measure; IQR, interquartile range; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System.
Missing values: race/ethnicity = 1/0, employment status = 1/0.
Wilcoxon rank sum test.
χ2 test.
Table 3 presents the results of univariable and multivariable linear regression models that compared social deprivation (measured using ADI values at the national level) and other patient characteristics to the PROMIS-PF outcome. The univariable analysis showed that a ten-point increase in ADI was only associated with an average decrease of 0.67 (95% CI: −0.93, −0.40, P < .001) in PROMIS-PF score, indicating that higher social deprivation was weakly, at most, related to lower physical function. Unemployed patients had an average PROMIS-PF score that was 3.12 points lower (95% CI: −4.70, −1.54, P < .001) compared with fully employed patients. In the multivariable analysis, after adjusting for patient demographics, a 10-point increase in ADI was only associated with an average decrease of 0.53 points (95% CI: −0.81, −0.26, P < .001) in PROMIS-PF score, whereas unemployed patients had an estimated PROMIS-PF score that was 2.90 points lower (95% CI: −4.49, −1.31, P < .001) than fully employed patients (Table 3).
Univariable and Multivariable Linear Regression Results to Access the Impact of ADI on PROMIS–Physical Function.

Abbreviations: ADI, Area Deprivation Index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Table 4 displays the results of univariable and multivariable linear regression models that investigated the association between social deprivation (measured using ADI values at the national level) and other patient characteristics with the PROMIS-PI outcome. The univariable analysis showed that a 10-point increase in ADI was associated with an average increase of 0.59 points (95% CI: 0.36, 0.81, P < .001) in PROMIS-PI score, indicating that higher social deprivation was weakly related to more pain. For unemployed patients, PROMIS-PI score was on average 2.06 points higher (95% CI: 0.7, 3.42, P = .003) than for those with full-time employment. In the multivariable model, there was an average increase of 0.43 points (95% CI: 0.20, 0.66, P < .001) in pain interference for every 10-point increase in ADI, after adjusting for patient demographics. For unemployed patients, the estimated PROMIS-PI score was 1.91 points higher (95% CI: −0.54, 3.28, P = .006) than for full-time working patients, adjusting for patient characteristics (Table 4).
Univariable and Multivariable Linear Regression Results to Access the Impact of ADI on PROMIS-Pain Interference.

Abbreviations: ADI, Area Deprivation Index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Discussion
Social deprivation quantifies socioeconomic variations that can impact health outcomes and includes factors such as poverty, education, access to transportation, employment, and living situation.4,29,35,39,54 Increasing attention is being paid to the potential impact of social deprivation on orthopaedic outcomes, but limited studies have explored this in the foot and ankle community. This study retrospectively analyzed more than 1500 new patient visits to orthopaedic foot and ankle surgeons and assessed whether there was a relationship between patient-reported outcomes (specifically, PROMIS and FAAM scores) with social deprivation levels. In this study, relationships between ADI and PROs were weak, at most—more socially deprived patients (ie, lower social deprivation scores) presented to the clinic with statistically less function (ie, lower PROMIS-PF) and greater pain (ie, higher PROMIS-PI).
However, although we found statistically significant differences, the clinical significance of these findings is unclear. Our results fall below the minimal important change or minimal clinically important difference thresholds for the various metrics used (ie, FAAM, PROMIS-PI, and PROMIS-PF). For example, between the least and most deprived median ADI split of patients, the median scores differences was 1.5 for both PROMIS-PF and PROMIS-PI. Although these values were statistically significant, prior studies have identified minimal clinically important difference values of 5 for high responsiveness and a range of 3-4 for moderate clinical meaningfulness within PROMIS domains results.28,44,54 Minimal important change values from other studies were shown to be relevant within a value range of 2-6 with a change score of 4-5 as the best cutoff points.46,54 It is possible that as we explore relationships between outcomes and social deprivation within specific clinical pathologies (ie, hallux valgus, ankle arthritis), the statistically significant difference may become more clinically apparent. But in the data we present here, the differences in pain and function between high and low social deprivation groups are essentially equivalent. Patients with greater social deprivation present similarly in pain and function as do patients with lower social deprivation.
Our findings coincide—and conflict—with previous literature comparing social deprivation and pain/function in other orthopaedic populations. Court-Brown et al demonstrated that social deprivation was associated with greater fracture incidence in the most deprived 10% of society. 14 In 2019, Wright et al conducted a cross-sectional study analyzing 7500 patients presenting to a high-volume academic orthopaedic center. They found that patients with the highest social deprivation, regardless of orthopaedic subspecialty, had worse PROMIS-PF, PROMIS-PI, anxiety, and depression scores. 54 Another study of 307 unicompartmental knee replacements discovered that patients with more social deprivation had less knee mobility before surgery, and postoperatively, had decreased ability to walk long distances. 6 Further, pediatric congenital hand patients from more socially deprived areas presented with worse PROMIS-PI, peer relations, anxiety, and depression. 51 These findings of social deprivation correlating with higher pain and lower function were mirrored for other orthopaedic surgical outcomes such as radial head and neck fractures, total hip arthroplasty, pediatric upper extremity fractures, and certain surgical complications.18,23,34,53 Taken together, our study adds conflicting evidence to the body of literature on social deprivation in orthopaedic conditions. 7
This study has clear limitations. Our cohort was, relative to communities across the county, relatively racially/ethnically homogenous. It is unclear, then, how generalizable our data are. Further study into study populations with greater racial and ethnic diversity may better elucidate further differences in social deprivation, as has been shown in other studies.11,12 Additionally, we did not study a single clinical condition but pooled all foot and ankle diagnoses for presentation to clinic. Exploring the impact of social deprivation on specific, common foot and ankle conditions could help to clarify the relationships between outcomes and social deprivation. Because PROMIS metrics assessing pain and function are not specific to foot and ankle problems, we were unable to control for other sources of pain or functional impairments that could have accounted for their baseline levels of increased pain and decreased function. Lastly, ADI scores are based on zip code “neighborhoods” and are not patient-specific measures—an individual patient’s circumstances and social deprivation may not be fully reflected in their ADI score. Further, the 2020 ADI data that we used was constructed from 5-year estimates (2015-2020) from the US Census’ American Community Survey form—but our study time frame was from 2016 to 2017. Our analyses cannot account for patient mobility (ie, changing addresses) or the possibility that ADI data outside our study time frame (2015, 2018-2020) unknowingly altered our findings.
Conclusion
The impact of social deprivation has garnered increasing attention in orthopaedics on how it may relate to patient-reported pain and function. Although we report here statistically higher pain and lower function at baseline in patients with greater social deprivation, the clinical significance of these relationships may be weak but merits further exploration. Effectively, patients presenting to foot and ankle clinics have similar pain and function levels regardless of their social deprivation status.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241290202 – Supplemental material for Influence of Social Deprivation on Patient-Reported Outcomes in Foot and Ankle Patients
Supplemental material, sj-pdf-1-fao-10.1177_24730114241290202 for Influence of Social Deprivation on Patient-Reported Outcomes in Foot and Ankle Patients by Kade Wagers, Blessing Ofori-Atta, Angela Presson and Devon Nixon in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Utah. Approval number IRB_00071733. The title for the IRB is “EXEMPTION UMBRELLA: Value of the treatment of musculoskeletal disorders at the University of Utah Covered Entity for lower extremity pathologies.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1TR002538.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.