
Abstract
Background:
Racial minorities are more likely to develop type 2 diabetes and experience associated microvascular complications. Non-Hispanic Blacks and Hispanics initially present with more severe diabetic foot ulcers (DFUs) and peripheral artery disease (PAD), with an associated 10-fold increase in risk for lower extremity amputation within the first year after diagnosis. This study was designed to determine if race is associated with a failure to refer to specialists for DFU treatment, and the severity of DFU at the time of initial presentation.
Methods:
Patients were identified from the medical record based on a diagnosis related to diabetic foot complications between January 1, 2018, and June 1, 2023, in the family medicine, endocrinology, orthopaedic, or emergency clinics at a Midwest Academic Hospital serving rural and urban populations. Patients self-reported race, demographics, severity of ulcer based on Wagner ulcer scale at time of referral, eventual amputation status, and measures of social determinants of health including the national Area Deprivation Index (ADI) and Rural-Urban Commuting Area (RUCA) codes were manually extracted and analyzed for correlations with referral status.
Results:
A total of 597 patients were eligible for inclusion. Race was not associated with lower referral rates (P > .99) or source of referral (P = .58) to specialty clinic and ulcer severity at initial examination (P = .34). Patients who initially presented to the emergency department had more severe ulcers (P = .016), and higher severity was significantly associated with lower limb amputation vs mild ulcers (odds ratio = 38.8, P = .02). No significant differences in referral source or severity of ulcer at presentation were seen for sex, age, marital status, insurance type, rural status, ADI, time from referral to appointment, or eventual amputation.
Conclusion:
In this study, we found that patient race was not associated with severity of DFU at presentation or subsequent referral to a Midwest academic specialty orthopaedic clinic for care.
Introduction
Diabetic foot ulcer (DFU) is a common sequela of diabetes mellitus (DM). DM affects roughly 11.3% of US adults, with racial minorities, including African Americans, Native Americans, Asian Americans, Hispanic/Latinos, and Pacific Islanders, reported to have the highest risk for developing DM and associated microvascular complications including DFU.2,17,23,25 Diabetic neuropathy and peripheral artery disease (PAD) put patients at highest DFU risk. In total, approximately 25% of patients with DM develop a DFU during their lifetime.1,5,20 DFUs are associated with increased risk for wound complications, infection, and need for amputation, and are independent risk factors associated with premature death.3,4,12,18 Five-year mortality for DFU is comparative to that of cancer patients, whereas mortality after lower limb amputation (LLA) surpasses that of cancer. 4
For DFU patients, efficient referral to a specialist is paramount for optimizing treatment outcomes.11,15 When referral is delayed, patients are at increased risk for developing more complex DFUs, often requiring emergent hospitalization. 17 When wound care and revascularization procedures are ineffective or unavailable, LLA becomes necessary; in the United States, 11% to 30% of DFU patients undergo LLA.3,5,16,19 -21 Despite higher rates of DM and associated DFU in the African American population, this subset of patients is less likely to undergo revascularization procedures, and twice as likely to receive an LLA within the first year after diagnosis of DFU.5,7,17,20,25 Further, non-Hispanic Blacks and Hispanics initially present with more severe DFUs and PAD, with an associated 10-fold increase in risk for LLA within the first year after diagnosis.5,20,25 Patients who live in rural areas, those with a lower socioeconomic status, men, and those without commercial or Medicare insurance also face increased risks for LLA.5,11,20,25
Although the high rates and risk factors for DFU-related LLAs in minority groups have been well documented, associations between referral to an orthopaedic wound specialist and social determinants of health (SDOH) in this patient population have not been fully characterized. In order to improve patient outcomes, it is important to determine if race or other SDOH impact referral rates for DFU patients to receive specialty care. If non-White race is associated with lower rates of referral for specialty care, it will signify need for additional education among clinicians to resolve disparities. To that end, the goal of this study was to characterize referral rates and associated patient demographics for DFU patients presenting to a Midwest academic hospital for treatment. This study was designed to determine (1) the associations of race and living status with rates of referral to specialists for DFU treatment, and (2) the severity of DFU at the time of initial presentation.
Materials and Methods
With institutional review board approval (IRB no. 2097348), electronic medical records (EMRs) were searched for family medicine, endocrinology, emergency department, and orthopaedic specialty clinic appointments coded for diabetic foot ulcer (International Classification of Diseases, Tenth Revision [ICD-10], code E11.621). Patients were included for analyses when they were at least 18 years of age, and their DFU clinic visit occurred between January 1, 2018, and June 1, 2023, in the family medicine (FM), endocrinology, orthopaedic, or emergency departments (ED) at a Midwest Academic Hospital serving the surrounding 26-county area. Patients younger than 18 years were excluded, or patients who had a diabetic foot ulcer as an ancillary finding during other routine care without a plan to discuss or address the ulcer with the patient noted in the EMR.
Study Population Variables
Patient demographic information was obtained through the EMR, and the following information was extracted: patient age, gender, self-reported race, address, insurance information, and marital status; initial visit service: FM, endocrinology, emergency department (ED), or orthopaedics/podiatry; and date of referral for specialist treatment for DFU. Patients who presented to orthopaedics/podiatry for DFU-related concerns without referral were also identified. Race was defined as White” or race other than White. Insurance was characterized into commercial, Medicaid, Medicare, and self-pay. Marital status was defined as married or not married. The national Area Deprivation Index (ADI) 22 was collected for each patient based on their address, 22 with a score closer to 100 representing areas with worse socioeconomic disparity.
DFU severity at onset was categorized using the Wagner ulcer scale 24 (Table 1) when EMR data were available. The Wagner severity grades were used to assign patients to relative severity groups as mild = grade 0-1, moderate = grade 2-3, or severe = grade 4-5.
Wagner Classification 13 for Diabetic Foot Ulcer.

Data and Statistical Analysis
Descriptive statistics were calculated to report means, ranges, standard deviations, and percentages. Patients were first grouped by referral to an orthopaedic specialty provider for diabetic foot complications (yes or no) and compared based on patient sex, age, marital status (married vs not married), insurance category (commercial, Medicaid, Medicare, self-pay), and race (White, self-reported race other than White). Patients were then grouped based on whether they were seen at all at an orthopaedic specialty provider (referred by the FM or endocrinology department vs self-referral), and the entire cohort of patients seen at the orthopaedic specialty provider was compared to those that were not. Chi-square or Fisher exact tests were used to assess for significant differences in proportions. Odds ratios were calculated when significant differences were identified. Normality and variance tests were performed, and unpaired t tests were used when assumptions were met, and ranked sum tests when assumptions were not met, to assess differences between cohorts. Statistical significance was set a priori at P <.05.
Results
Referral Source
The EMR search identified a total of 685 potentially eligible patients and 89 were subsequently excluded due to the lack of a DFU. Of the 596 patients included in the analysis, 97 patients (16.3%) were seen at orthopaedic specialty clinics. No differences in orthopaedic referral status were identified based on race, sex, age, primary insurance payer, rural status, or marital status (Table 2). Referral source to the specialty clinic (ED/self-referral vs FM or endocrinology department) was not significantly different based on race (P = .58), rural status (P = .18), marital status (P = 1), insurance type (P = .45), age (P = .11), time from referral to appointment (P = .45), or eventual amputation (P = .43). (Table 3).
Demographics of the Study Population. a

Abbreviation: URM, underrepresented minority.
The table includes demographics analyzed, patients with a diabetic foot ulcer seen at the family medicine or endocrinology department, patients who were referred to an orthopaedic specialty clinic from family medicine, endocrinology, self-referral, or the emergency department, and P values that represent the differences between both groups.
Demographics of the Patients Seen at Orthopaedic Specialty Clinic With a Diabetic Foot Ulcer.

Abbreviations: FM, family medicine; Endo, Endocrinology; URM, underrepresented minority.
Ulcer Severity
Patients who initially presented to the ED and subsequently saw an orthopaedic specialty clinic were more likely to have more severe ulcers vs mild ulcers (OR 4.4, CI 1.62-12.12, P = .004) or moderate severity ulcers vs mild ulcers (OR 5.1, CI 1.18-21.91, P = .03) compared to patients referred by the FM or endocrinology department. Among the 56 patients seen in the ED, 23.2% of the ulcers were mild, 57.1% were moderate, and 19.6% were severe. For patients initially seen at the FM or endocrinology department, 58% (18 of 31) had mild ulcers, with 32.3% and 9.7% presenting with moderate and severe ulcers, respectively. Of the 10 patients who self-referred or were referred by a specialty other than the ED, FM, or endocrinology department, 2 were mild, 6 were moderate, and 2 were severe (Figure 1). Ulcer severity was the only variable analyzed that was significantly associated with subsequent LLA, with severe ulcers significantly associated with LLA vs mild ulcers at presentation (OR = 38.8, P = .02). Moderate ulcer at presentation was not significantly associated with eventual LLA vs mild ulcer at presentation (P = .23). Race was not associated with ulcer severity at the time of presentation, as underrepresented minorities (URMs) and White patients had similar severity grades among the different referral sources (P = .34, Figure 2), and race was not associated with subsequent LLA in this study population (P = .36). Ulcer severity was not significantly different based on rural status (P = .20), sex (P = .85), age (P = .71), marital status (P = .62), state ADI (P = .99), national ADI (P = .52), time from referral to appointment (P = .25), or insurance type (P = .07).
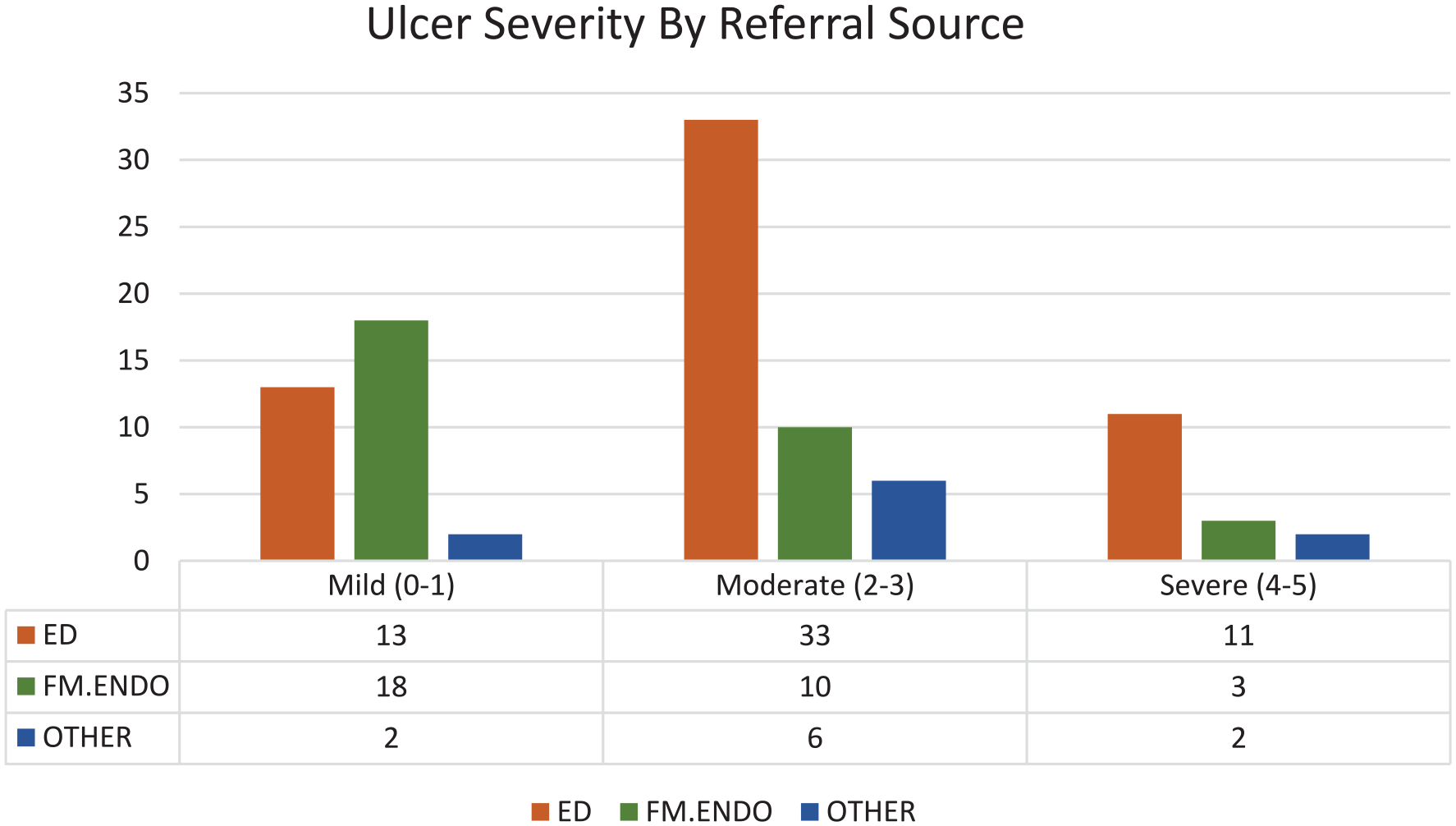
Number of patients from different referral sources and their grouped ulcer severity score based on the Wagner Scale. P = .016.

Referral source for those seen at the orthopaedic specialty clinic.
Discussion
The findings from this study elucidate important patient characteristics and influences on specialty referral patterns for DFU patients that can affect treatment outcomes. Interestingly, referral from the FM or endocrinology department were the only variables analyzed that significantly affected presentation and specialty referral patterns, and DFU severity at presentation was the only factor analyzed that was significantly associated with subsequent need for LLA. In our patient population, race and other SDOH analyzed were not significantly associated with specialty referral, severity of DFU at presentation, or subsequent need for LLA. Taken together, these results suggest that specialty referral patterns and the associated effects on DFU severity and need for LLA for a Midwest academic hospital differ from what has previously been reported for more urban centers. As such, further analyses may identify other aspects of the care continuum that could be addressed and generalized across settings in order to improve care and outcomes for patients at risk for, or affected by, DFUs.
In 1991, Lavery et al 13 reported on hospitalization for LLA related to DM in the state of California, analyzing 8169 patients and concluding that African Americans had the highest incidence of LLA when adjusting for age. In a population of 643,287 patients enrolled in Medicare fee for service between 2012 and 2017, Miller et al 20 noted an increase in African American individuals receiving LLA within a year of DFU diagnosis, but did not find national ADI to have a significant influence on the timing of LLA. Gibson et al 11 performed a retrospective analysis to identify outcomes of care in patients with DFUs and reported that patients using commercial or Medicare insurance who received care from podiatrists were significantly older than those who did not. DFU patients receiving care from podiatrists also had a longer length of time to amputation, suggesting alternative treatment options were provided prior to LLA.
Diabetic foot care often begins with primary care providers to ensure adequate assessment and education. African Americans do not use primary care at equivalent rates to White patients, leading to higher rates of emergency department visits and associated inferior health outcomes.6,9,10 Although Medicare and Medicaid have reduced systematic segregation in medical facilities, the African American population continue to underutilize medical care. 9 Limited access and medical mistrust among the African American community enhances these disparities, and solutions continue to be explored to reduce this gap. 6 Residential segregation impacts access to private primary care physicians and specialists, as many are absent in highly segregated African American communities. 6 Safety net facilities, commonly providing care to Medicaid beneficiaries and the uninsured, 26 are more likely to be present in the neighborhoods that are more densely African American, leaving these communities with inferior and less specialized care. 6
Interestingly, patients in the present study who were referred for orthopaedic specialty care that included podiatrists did not indicate significant influences of race or other SDOH on specialty referral, severity of DFU at presentation, or need for LLA. This could be explained by limited diversity in our patient population compared with those previously reported, possibly masking a true difference among races. Previous studies have occurred in urban populations, whereas our facility serves a 26-county rural and urban area. If patients are referred, attending appointments may be limited because of scant public transportation and distance needed to travel. This may impact the ability of all patients to attend specialty referral appointments.
Community outreach and integration into underserved and minority communities may help facilitate closure of this health care gap. Mobile medical clinics are an invaluable way to build medical trust among racial minorities, as patients with DM have been found to visit mobile medical clinics more often, highlighting the importance of preventative care, primary care, and health care screening to ensure equitable care among all individuals.8,14,23 Primary care providers and orthopaedic surgeons should work together as a multidisciplinary team to improve clinical outcomes and reduce disparities related to DFUs and LLAs. To implement this, occasional grand rounds within orthopaedic surgery and primary care can be combined to discuss patient referral, nonsurgical, and surgical treatment options. In our patient population, patients in worse socioeconomic disparity, or higher national ADI, were more likely to be referred to foot and ankle specialists from the ED. Having a group of medical students, nurses, residents, primary care physicians, and specialty physicians from our institution volunteer their time a few times a year to offer free services in the higher-ADI communities may help reduce the disparities.
This study was not without limitations. Inherent to a retrospective review is the limitation associated with data availability and accuracy. This study method is subject to confounding and selection bias. Data extraction included patients with type 2 diabetes who did not have a foot ulcer or who had previously healed ulcers outside of the time frame, which were manually reviewed in the chart and excluded by researchers. Patients may have primary and secondary insurance, or changes to insurance within the time frame studied. Race and ethnicity are self-reported, with some patients opting out. To reduce this limitation, multiple researchers reviewed the data extraction for accuracy and completeness. Disease prevalence may vary among regions within the United States. Additionally, the Midwestern city where this research took place is relatively homogenous and does not match the US population racial makeup. As such, results may not be supported when this study is conducted in larger, more diverse communities. However, the results are representative of rural Midwest communities and can be applicable to those patient populations. Our study did not account for those who died within the study period, whether during hospitalization for surgery or other medical comorbidities. Future research should include larger cohorts and should examine time to surgery and type of surgery done to examine if difference occurs based on race throughout the country. Expanding the population scope to include surrounding cities with more heterogeneity in their population may also help validate findings.
In conclusion, the results of this study indicate that patient race was not associated with severity of DFU at presentation or subsequent referral to a Midwest academic specialty orthopaedic clinic for care. In this patient population, DFU severity at presentation was the only factor significantly associated with subsequent LLA. Future research analyzing other SDOH and its impact on DFU and LLA, as well as implementing physician involvement in communities to educate populations on DFU care is needed to improve patient outcomes following DFU.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241281335 – Supplemental material for Association of Race With Referral Disparities for Patients With Diabetic Foot Ulcers at an Institution Serving Rural and Urban Populations
Supplemental material, sj-pdf-1-fao-10.1177_24730114241281335 for Association of Race With Referral Disparities for Patients With Diabetic Foot Ulcers at an Institution Serving Rural and Urban Populations by Mubinah Khaleel, Ashwin Garlapaty, Sam Hawkins, James L. Cook, Kyle Schweser and Kylee Rucinski in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Missouri Institutional Review Board (approval 2097348).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.