
Abstract
Background:
Total ankle arthroplasty (TAA) has primarily been performed in the inpatient setting. However, with the advent of fast-tracked joint arthroplasty protocols, TAA has slowly been shifting to the outpatient setting. Therefore, this systematic review aims to evaluate outcomes of outpatient TAA and compare them to inpatient TAA.
Methods:
A literature search was performed on October 23, 2023, in the PubMed, Embase, and CENTRAL databases using the PRISMA guidelines. Studies were included if they reported on outcomes of outpatient TAA or compared outcomes between outpatient and inpatient TAA. Pooled odds ratios (ORs) and mean differences were calculated using a random effects model. Quality assessment was performed using the MINORS criteria.
Results:
12 studies were included, with 4 outpatient-only and 8 outpatient-inpatient comparative studies. Patients in the outpatient group were relatively younger, had a lower body mass index, and had fewer comorbidities relative to the inpatient group. For outpatient vs inpatient TAA, the pooled complication rate was 2.6% vs 3.6%, readmission rate was 2.5% vs 4%, and reoperation rate was 3.6% vs 5.5%. We found significantly lower odds of complications (OR = 0.47, CI: 0.26-0.85; P = .01), readmissions (OR = 0.63, CI: 0.54-0.74; P < .00001), and reoperations (OR = 0.66, CI: 0.46-0.95; P = .03) in the outpatient vs inpatient group.
Conclusion:
Although this analysis is limited by the dominance of data included from a single study, we found that outpatient TAA was generally performed on lower-risk patients and was associated with lower rates of complications, readmissions, and reoperations compared with inpatient TAA.
This is a visual representation of the abstract.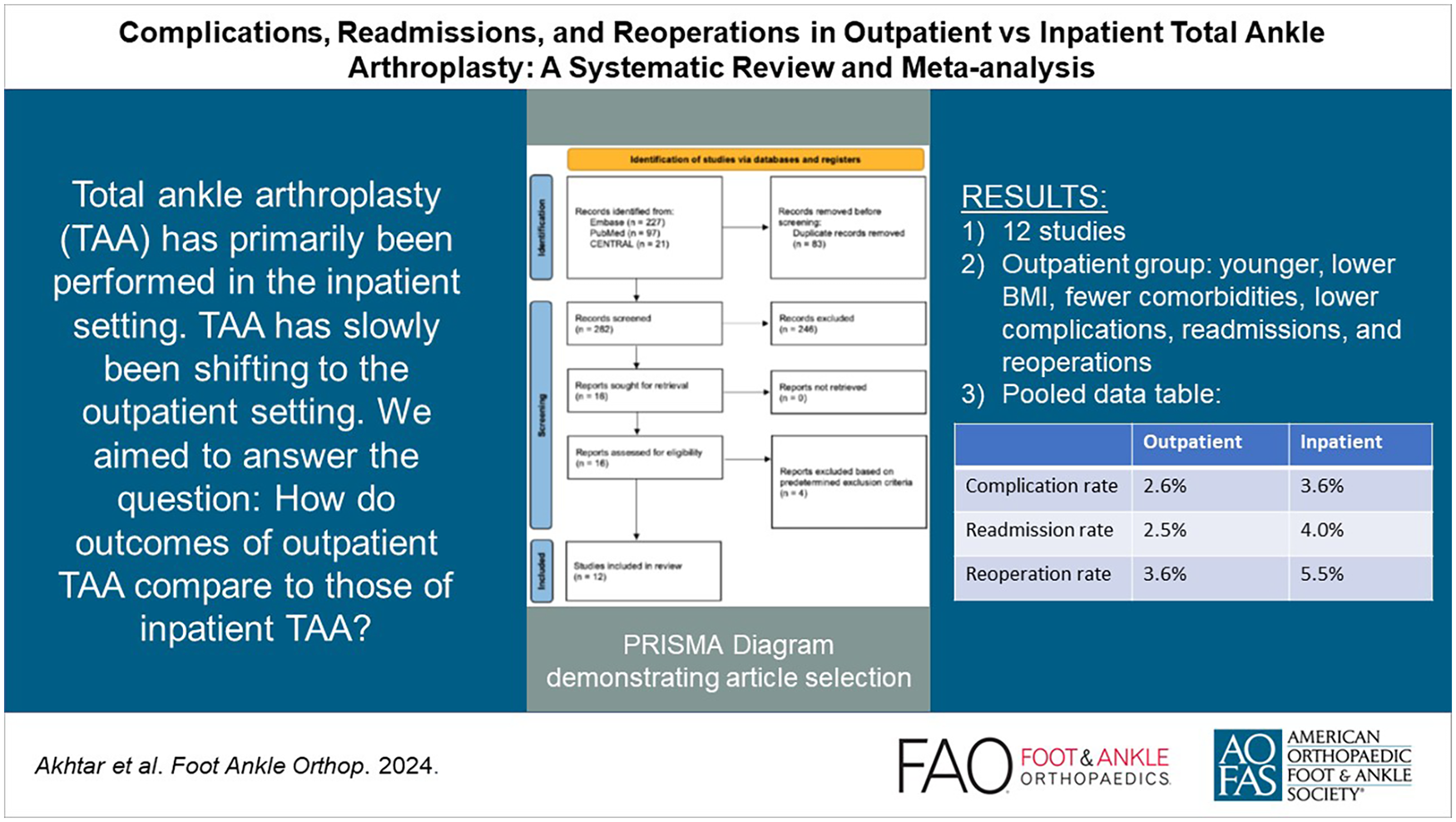
Introduction
Total ankle arthroplasty (TAA) has emerged as an effective surgical intervention to address end-stage ankle arthritis, aiming to alleviate pain, improve function, and enhance overall quality of life. Traditionally, TAA has been performed in an inpatient setting, requiring hospital admission postprocedure. However, recent advancements and shifting paradigms in orthopaedic surgery have prompted a reassessment of the optimal setting for TAA, with a growing trend toward outpatient surgery. 5
The primary goal of TAA is to address debilitating conditions that significantly impact ankle joint function such as osteoarthritis, rheumatoid arthritis, and posttraumatic arthritis. The procedure entails replacing the damaged ankle joint with an artificial implant, providing patients with improved joint mobility, a more natural physiological gait, and reduced pain. 22 Historically, this intricate procedure has been linked to inpatient care, necessitating postoperative monitoring and management of potential complications.
Recent studies challenge the traditional notion of inpatient TAA, suggesting that the procedure can be safely and effectively performed on an outpatient basis. This shift mirrors the evolution observed in total hip and knee arthroplasty, where outpatient procedures demonstrate equivalent or lower revision rates, failure rates, complication rates, readmission rates, and favorable patient-reported outcomes.4,12,14
A systematic review published in 2020 examined complication rates in patients who underwent TAA in the inpatient vs outpatient setting. 2 However, the meta-analysis was composed of only 4 studies and combined all events (complications, readmissions, revisions, etc) as one category when comparing the 2 patient populations. The present study aims to statistically compare events at a more granular level, with independent analyses for complications, readmissions, and revision rates.
Examining the transition of total hip and knee arthroplasty to the outpatient setting offers valuable insights into understanding the potential benefits of outpatient TAA. Although there are limited economic and financial data specific to TAA in the literature, the cost-effectiveness of outpatient total hip and knee arthroplasty is noteworthy. Potential cost savings associated with outpatient procedures stem from reduced hospital length of stay, decreased use of health care resources, and a shift toward more efficient and streamlined care models. 8
The primary objective of this study is to evaluate postoperative rates of complications, readmission, and revision surgery following outpatient TAA. A secondary objective is to compare complications, readmission, and revision surgery rates in outpatient vs inpatient TAA. We hypothesize that outpatient TAA would have low rates of complications, readmission, and revision surgery relative to inpatient TAA.
Methods
Search Strategy
A search following guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) was performed in 3 databases on October 23, 2023: PubMed, Embase, and the Cochrane Library. The query was performed using the Boolean search phrase “((ankle replacement) OR (ankle arthroplasty)) AND ((((same-day) OR (same day)) OR (ambulatory)) OR (outpatient)).” There were no restrictions set to the search. Studies were included if they solely reported on outcomes of outpatient TAA or if they compared outcomes between outpatient and inpatient TAA. Exclusion criteria included case reports, systematic reviews and meta-analyses, review articles, conference abstracts, studies performed in animals, articles not in English, expert opinions, letters to editors, and studies in which outcomes pertaining to outpatient ankle arthroplasty were not specified. This study was registered on PROSPERO (ID:
Study Selection
Two independent reviewers reviewed studies for eligibility criteria from the initial database search. A third senior author was available for any disputes. When multiple studies from the same author were found, only the one with the longest follow-up period was included to avoid counting the same patients multiple times. All included articles underwent rigorous reference search to determine whether additional studies could be added to the systematic review.
Data Extraction
Study variables extracted from each article included author, publication year, journal, level of evidence (LOE), study time period, study design, definition of inpatient and outpatient, patient demographic variables, complication rates, readmission rates, reoperation or revision surgery rates, patient-reported outcomes (PROs), operative time, tourniquet time, and concomitant procedures. All extracted data were compiled for analysis using Microsoft Word (Microsoft Office 2011; Microsoft, Redmond, WA).
Quality Assessment and Risk of Bias
The methodologic quality of studies was assessed using the Methodological Index for Non-randomized Studies (MINORS) which has a maximum possible score of 16 for noncomparative studies and 24 for comparative studies. Two authors scored each article in the systematic review. Each author scored the article individually before reviewing their scores, and any discrepancies were resolved by rereviewing the articles until a unanimous consensus was met. The risk of bias (ROB) was determined based on the overall MINORS score. The ROB was considered high if the MINORS score was 0 to 8 (0-16 for comparative studies), moderate if the MINORS score was 9 to 12 (16-20 for comparative studies), and low if the MINORS score was 13 to 16 (21-24 for comparative studies).
Statistical Analysis
Descriptive statistics (mean, percentage, SD, range, median) are reported in this review when applicable and when available. A meta-analysis consisting of an odds ratio (OR) for the complication rate, readmission rate, and reoperation rate was performed to compare outpatient vs inpatient TAA. Additionally, the pooled mean difference was calculated to compare operation time and tourniquet time between outpatient vs inpatient TAA. Forest plots depicting data from all studies, the overall significance, and the I 2 statistic to assess heterogeneity were created using Cochrane’s Reviewer Manager web application (RevMan; Computer program, version 5.4, The Cochrane Collaboration, 2020).
When determining an OR, if the events of complications, readmission, or revision were 0 in both the inpatient and outpatient group for a single study, this would have resulted in a division by 0 error, thus not allowing us to calculate the OR. If that were the case for any study in a specific meta-analysis, then a Haldane-Anscombe correction was performed in which 1 event was added and n = 1 patient was added to the total number of patients in each study, allowing us to approximate the OR with strong accuracy. This occurred in the meta-analyses for readmission and revision, but not complications.
Results
Article Selection Process
On the initial search of the 3 databases, 345 studies were identified, of which 83 duplicates were removed. The remaining 262 studies underwent full title and abstract review, of which 246 were removed based on our predetermined exclusion criteria. The remaining 16 studies underwent full-text review. Four of these studies were excluded as they did not fit our predetermined inclusion criteria. The remaining 12 were included in this systematic review (Figure 1).

PRISMA flow diagram depicting the article selection process.
Methodological Index and Risk of Bias Assessment
The mean ± SD (range) of the MINORS score for studies comparing outpatient vs inpatient TAA was 16.6 ± 2.4 (range, 13-20). For noncomparative studies evaluating outpatient TAA only, the MINORS score was 10.3 ± 0.4 (range, 10-11). Overall, the risk of bias was high for 2 studies and moderate for 10 studies. No study had a low risk of bias.
The moderate to high risk of bias is likely due to the fact that all studies had a retrospective design, were nonrandomized, had varying definitions of outpatient vs inpatient status, and compared patients with some significantly different baseline characteristics. However, it would have been pragmatically challenging to address the research question through studies with stronger designs, such as randomized controlled trials, because outpatient vs inpatient status varies from patient to patient and is most commonly based on their baseline characteristics.
Study Characteristics and Patient Demographic Information
A total of 8 studies published between 2017 and 2023 comparing outpatient vs inpatient TAA were included, with 1 study having an LOE of II and 7 studies having an LOE of III. There were 9989 patients (47.7% male; 52.3% female) in the outpatient group and 13 357 patients (50.2% male; 49.8% female) in the inpatient group. Four studies reported that patients in the inpatient group had a significantly higher age (P < .005).1,6,20,23 In contrast, 2 reported that both groups had similar ages (P = .17 and .88).10,15 One study reported that the outpatient group had a significantly higher proportion of patients between ages 50 and 59 years (P = .043), and the inpatient group had a significantly higher proportion of patients greater than 80 years (P = .046). 16 Three studies reported that patients in both groups had a similar body mass index (BMI; P > .05).1,6,10 One study reported that there was a significantly greater proportion of overweight patients (BMI: 25-29.9) in the outpatient group (P = .009), but otherwise, both groups had similar BMIs in the underweight, normal, and obese categories (P > .05). 16 Five studies reported comorbidity scores, with 4 reporting the ASA and 1 reporting the CCI. Two of the 5 studies found significantly worse comorbidities in the inpatient group.1,6 In contrast, 2 other studies found a similar rate of comorbidities between the 2 groups.10,15 One study found that ASA scores of 1 and 2 were significantly more common in the outpatient group (P = .039 and .003). In contrast, an ASA score of 3 was significantly more common in the inpatient group (P < .001). 16 Patients were evaluated 1-29.7 months after the index TAA (Table 1).
Key Features and Demographics of Studies Included in the Systematic Review and Meta-analysis.

Abbreviations: ASA, American Society of Anesthesiologists; ASC, ambulatory surgery center; CCI, Charlson Comorbidity Index; LOE, level of evidence; LOS, length of stay.
The MINORS score was out of 24 for comparative studies and 16 for noncomparative studies.
A total of 4 studies evaluating only outpatient TAA published between 2018 and 2022 were included, with 1 study having an LOE of III and 3 studies having an LOE of IV. There were 182 patients (48.4% male; 51.6% female) with a mean age of 61.5 years. The mean BMI across 3 studies (141 patients) was 28.6. Three studies reported comorbidities with the ASA score; for 131 patients, the ASA score was 1 in 19 patients, 2 in 68 patients, 3 in 41 patients, and 4 in 3 patients. Patients were evaluated 1-20.7 months after the index TAA (Table 1).
Complications, Readmissions, and Reoperation or Revision Surgery
Complications were defined as negative unforeseen events that deviated from the typical postoperative course, not including reoperation or revision surgery, which we created a separate category for in order to compare outpatient vs inpatient outcomes at a more granular level. Complications were reported in all 8 comparative studies. The overall complication rate was 2.5% (247/9989) in the outpatient group and 3.6% (479/13 357) in the inpatient group. Readmissions and reoperations were reported by 7 of the 8 comparative studies. The overall readmission rate was 2.6% (243/9464) in the outpatient group and 4% (532/13 291) in the inpatient group. The overall reoperation rate was 3.6% (337/9464) in the outpatient group and 5.5% (729/13 291) in the inpatient group. The meta-analysis found significantly lower odds of complications (OR: 0.47, 95% CI: 0.26-0.85, P = .01; Figure 2), readmissions (OR: 0.63, 95% CI: 0.54-0.74, P < .00001; Figure 2), and reoperations (OR: 0.66, 95% CI: 0.46-0.95, P = .03; Figure 2) in the outpatient vs inpatient group.

Forest plot for the odds ratio of outpatient vs (A) inpatient complications, (B) readmissions, and (C) reoperation/revision surgery.
Seven of the 8 studies reported whether complication rates were similar or significantly different between both groups. Three studies found a significantly lower rate of complications in the outpatient group,15,16,23 and 4 studies reported no significant differences between both groups.1,6,10,20 Six of the 8 studies reported whether readmission and reoperation rates were similar or significantly different between the 2 groups. Two studies found significantly lower readmission rates in the outpatient group,6,23 whereas 4 studies found no significant differences in readmission rates.8,10,15,16 One study found significantly lower reoperation rates in the outpatient group, 23 whereas 5 studies found no significant differences in reoperation rates.1,6,8,15,16
Four studies that only evaluated outpatient TAA reported complications, readmissions, and reoperations. The complication rate was 8.2% (15/182), the readmission rate was 0%, and the reoperation rate was 8.2% (15/182).
Across all the 12 studies included, the overall outpatient complication rate was 2.6% (262/10171), readmission rate was 2.5% (243/9646), and reoperation rate was 3.6% (352/9646) (Table 2).
Complications, Readmissions, and Reoperations.

Abbreviations: DVT, deep vein thrombosis; MI, myocardial infarction; SSI, surgical site infection; UTI, urinary tract infection.
Patient-Reported Outcomes and Pain Scores
Two comparative studies reported PROs or pain scores. The mean preoperative VAS pain score was 5.2 for the outpatient group (49 patients) and 6.2 for the inpatient group (129 patients). The mean postoperative VAS pain score was 2.3 for the outpatient group (114 patients) and 1.5 for the inpatient group (145 patients). Both studies reported no significant difference between both groups’ postoperative VAS pain scores (P = .73 and .72). Furthermore, Akoh et al 1 reported that preoperatively to postoperatively, the inpatient group had a significant improvement (P < .05) in the SF-36, VAS pain, AOFAS, SMFA function, and SMFA bother scores. However, the outpatient group only had a significant improvement (P < .05) in the SF-36, VAS pain, and AOFAS scores (Table 3).
Preoperative and Postoperative Patient-Reported Outcomes and Pain Scores.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle-hindfoot score; PRO, patient-reported outcome; SF-36, 36-Item Short Form Health Survey; SMFA, Short Musculoskeletal Function Assessment; VAS, visual analog scale.
PROs and pain scores are reported as mean ± SD (range) when available.
Two noncomparative outpatient-only studies reported the VAS pain score. The mean preoperative VAS pain score was 5.7 (25 patients), and the mean postoperative score was 1.5 (66 patients).
Operation and Tourniquet Time
Across 5 outpatient studies (211 patients), the mean tourniquet time was 113 minutes. In contrast, across 2 inpatient studies (139 patients), the mean tourniquet time was 144.1 minutes. Across 4 outpatient studies (664 patients), the mean operation time was 148.6 minutes. In contrast, across 3 inpatient studies (211 patients), the mean operation time was 187.3 minutes. Two studies were included in a meta-analysis comparing outpatient vs inpatient tourniquet and operation time. The tourniquet time was significantly lower in the outpatient group (P = .03; Figure 3), whereas the operation time was similar between the 2 groups (P = .59; Figure 3).

Forest plot for the mean difference of outpatient vs inpatient (A) tourniquet time and (B) operation time.
Discussion
In this systematic review, we evaluated 12 total studies, 8 of which compared outpatient vs inpatient TAA and 4 focused solely on outpatient TAA. The primary findings of this review are that outpatient TAA had lower rates and odds of complications, readmissions, and reoperations compared to inpatient TAA. However, patients undergoing outpatient TAA were relatively younger and had fewer comorbidities compared to inpatient patients, thus emphasizing the importance of appropriate patient selection.
The findings of our meta-analyses were similar to the findings in the included study by Wolfe et al 23 in which they reported significantly lower rates of infections, readmission within 90 days, and TAA failure requiring revision in the outpatient group. In the meta-analyses presented in Figure 2, the study by Wolfe et al 23 single-handedly comprised >80% of the total patients, which may have potentially skewed the results. Therefore, we performed a subanalysis in which we first removed the study by Wolfe et al 23 and then reevaluated the odds of complications, readmissions, and revision surgery in the outpatient vs inpatient group. The odds of complications (OR: 0.37, 95% CI: 0.16-0.83, P = .02) and readmission (risk ratio: 0.45, 95% CI: 0.22-0.92, P = .03) were significantly higher in the inpatient group, whereas the odds of revision (OR: 0.76, 95% CI: 0.37-1.54, P = .44) were now similar between the 2 groups.
Patients undergoing outpatient TAA had lower rates and odds of complications, readmission, and reoperations compared to inpatient TAA. The findings in the present review are consistent with the current literature regarding outpatient joint arthroplasty, including total hip (THA) and total shoulder arthroplasty (TSA). A 2020 study by Rosinsky et al 18 found no differences in readmission rates, complication rates, or 2-year revision rates between inpatient and outpatient THA. Trudeau et al 21 concluded that when adjusting for comorbidities, outpatient TSA was a safe option for a select cohort of patients. The findings of these studies should be interpreted through the lens of the patient population selected for outpatient procedures. Interestingly, Rosinsky et al 18 performed a matched trial where 91 outpatient procedures were compared to 91 inpatient procedures. There were no significant differences in age, BMI, comorbidities, or surgical time. However, the average length of stay was 6.8 hours in the outpatient group compared to 43.2 in the inpatient group, suggesting inpatients required greater postoperative supervision. Conversely, Trudeau et al 21 found the outpatient group was younger, less likely to have ASA scores of 3 or 4, and overall had fewer comorbidities, including diabetes mellitus, obesity, hypertension, and chronic obstructive pulmonary disease. This study also found in a non-risk-matched analysis that the outpatient group had lower rates of major or minor adverse effects and lower overall rates of readmission. In our review, 3 of the 8 comparative studies performed a subanalysis in which patients were matched such that no significant preoperative differences remained between outpatient and inpatient groups except for length of stay.6,16,23 Del Balso et al 6 found no significant differences in complications or reoperations but significantly higher 30-day readmissions in the inpatient group. Plantz et al 16 found no differences in operative complications, unplanned readmissions, reoperations, and mortality, whereas medical complications were significantly higher in the inpatient group. Wolfe et al 23 found that readmissions, arthroplasty failure, and infections were significantly higher in the inpatient group. Therefore, even when factors such as age, BMI, and comorbidities are controlled for, patients undergoing outpatient TAA have similar or better, but not worse, outcomes than inpatient TAA.
An important topic of discussion within the orthopaedic community is the proper selection of patients for inpatient and outpatient procedures. In the present review, generally older patients were found in the inpatient groups, with higher rates of comorbidities found in this group in several included studies. These findings call into question the characteristics of the ideal candidate for outpatient procedures. A 2019 study by Edwards et al 7 discussed in detail the criteria that physicians should consider when excluding patients for outpatient total knee arthroplasty (TKA). Medical factors included but were not limited to cardiovascular disease, chronic kidney disease, liver disease, pulmonary disease, and chronic steroid use. Psychosocial factors were also mentioned and included age >70 years, lack of social support, history of depression or anxiety, history of falls, and lack of transport. This study highlights the importance of evaluating patients holistically when selecting the ideal candidate for outpatient orthopaedic procedures. Similar considerations should be made when assessing a patient for outpatient TAA. Although comorbidities have been shown to increase the risk of readmissions, revisions, and mortality in total joint arthroplasty, 17 psychosocial factors should not be ignored. Heavy emphasis is placed on the patient to take postoperative rehabilitation protocols into their own hands, which can be difficult if they do not have adequate home support. Further investigation is therefore warranted regarding enhancing postoperative outcomes and rehabilitation protocols in outpatient TAA, taking all factors into account.
Efficiency in the OR and resource optimization have been topics of interest within the medical community for decades and are applicable in the discussion regarding outpatient and inpatient orthopaedic procedures. In the studies that included these metrics, the average tourniquet time and operation time were lower for outpatient groups compared with inpatient. One study made mention of cost differences between outpatient and inpatient TAA and found total costs to be significantly lower in the outpatient group. 1 A 2017 study by Huang et al 9 found that TKA patients who were discharged the same day yielded a median cost saving of approximately 30% compared with inpatients undergoing TKA. Savings primarily came from inpatient expenses such as pharmacy, patient meals, and the surgical ward. Although it is likely that outpatient TAA patients incur similarly decreased costs for a hospital or surgery center, further research is warranted.
This systematic review should be considered in the context of its limitations. First, studies had varying definitions of outpatient TAA. Some studies defined it as TAA performed in an outpatient surgery center, whereas others defined it as patients discharged on the same day or requiring overnight stay. Second, follow-up periods were generally limited to a few months after surgery, which may limit longer-term comparison of outcomes between outpatient and inpatient TAA. Third, some studies comparing outpatient vs inpatient TAA included patients with significantly different preoperative characteristics such as age, BMI, and comorbidity status. Outpatients may have done better postoperatively because of favorable preoperative conditions relative to inpatients. If everything except outpatient vs inpatient status was controlled for, it might have allowed for a more accurate comparison as to whether outpatient is superior to inpatient TAA. Finally, data on secondary outcome measures in this review such as patient-reported outcomes, pain scores, tourniquet time, operation time, and cost were limited. Therefore, although conclusions were derived from available data, they may not be as strong as the primary outcome measures including complications, readmissions, and reoperations.
Conclusions
Although the vast majority of the data included in this review stemmed from a single study, outpatient TAA had lower rates of complications, readmissions, and reoperations compared to inpatient TAA who were generally older with more comorbidities than those selected for outpatient TAA surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241264569 – Supplemental material for Complications, Readmissions, and Reoperations in Outpatient vs Inpatient Total Ankle Arthroplasty: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114241264569 for Complications, Readmissions, and Reoperations in Outpatient vs Inpatient Total Ankle Arthroplasty: A Systematic Review and Meta-analysis by Muzammil Akhtar, Daniel Razick, Deeksha Mamidi, Sonia Aamer, Fayez Siddiqui, Jimmy Wen, Sakthi Shekhar, Adithya Shekhar and Jason S. Lin in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.