
Abstract
Background:
There has been increasing interest in the use of percutaneous or minimally invasive osteotomy techniques for bunionette correction. The aim of this systematic review was to investigate the clinical and radiographic outcomes following percutaneous or minimally invasive surgery for bunionette deformity correction.
Methods:
A systematic review following PRISMA guidelines was undertaken. All clinical studies published in MEDLINE, Embase, PubMed, and the Cochrane Library Database from inception until December 2023 reporting on the use of percutaneous or minimally invasive osteotomy techniques for bunionette deformity correction were included. The primary outcome was radiographic deformity correction. A meta-analysis of clinical and radiographic outcomes was performed to assess the mean difference following surgery. Risk of bias was assessed using the ROBINS-I tool.
Results:
A total of 942 potential studies were identified, of which 18 were included encompassing 714 feet in 580 patients. There were no comparative studies identified. The majority of studies (n = 14/18) used an unfixed distal osteotomy technique. All studies showed a statistically significant improvement in clinical outcomes (American Orthopaedic Foot & Ankle Society ankle-hindfoot score and visual analog scale for pain) and radiologic outcomes (fourth-fifth intermetatarsal angle and fifth metatarsophalangeal angle). Complication rates ranged from 0% to 21.4%. The nonunion rate was 0% to 5.6%. Overall risk of bias was low to moderate. The most common complication was development of a hypertrophic callus that tended to resorb over time without needing further surgical intervention.
Conclusion:
The results of this systematic review must be considered in light of the methodologic limitations of the studies analyzed—including additional procedures performed at the same time as the bunionette correction, lack of comparative studies, and heterogeneity of the case series included. Despite these limitations, our review suggests that percutaneous techniques for bunionette deformity correction are generally clinically safe and associated with improvement in radiographic alignment and patient-reported outcome measures.
Keywords
Introduction
A bunionette or Tailor’s bunion is a deformity of the fifth metatarsal characterized by lateral deviation of the metatarsal and varus deviation of the toe leading to a bony prominence that can cause pain and difficulty with footwear.7,12 The prevalence of bunionette deformity is 14% with a higher incidence in females and older patients.6,22 Bunionette deformity is typically classified into 3 subtypes based on the underlying anatomy and morphology (Figure 1).5,7

Illustration of Coughlin classification of bunionette deformity. 7
The traditional surgical management for a bunionette deformity has been an open lateral approach using a range of osteotomy techniques including sliding, transverse, oblique, and scarf among others.3 -5,21 A systematic review from 2018 found that significant deformity correction could be achieved with all osteotomies; however, patient satisfaction was higher with distal osteotomies. 21
There has been increasing interest in the use of percutaneous or minimally invasive techniques for forefoot deformity and bunionette correction.18,23,30 First described by de Prado and Isham, percutaneous techniques use a high-torque, low-speed burr to perform the osteotomy. 23 A number of case series have found positive results in terms of deformity correction, complication profile, recurrence, and clinical outcomes.3,16,23,25 There are potential advantages of percutaneous techniques for bunionette correction including smaller wounds, fewer hardware-related complications, and quicker recovery.3,20,25 The learning curve for percutaneous bunionette correction is small compared to other percutaneous deformity correction procedures, so this technique can be easily adopted in clinical practice.20,24 There are, however, no randomized or comparative studies investigating open vs percutaneous osteotomy techniques. A recent consensus in percutaneous bunionette correction found that the majority of surgeons use no fixation for the osteotomy, avoiding lateral condylectomy alone as this fails to correct the deforming forces (Figure 2). 23

Deforming forces affecting the fifth metatarsal contributing to bunionette deformity.
The aim of this systematic review was to investigate the clinical and radiographic outcomes following percutaneous or minimally invasive surgery for bunionette deformity correction. We hypothesize that percutaneous techniques for bunionette correction will enable deformity correction with an acceptable complication rate.
Methods
Study Design
This study was performed according to the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. 29 Details of the protocol for this systematic review were prospectively registered on PROSPERO (CRD42024497258).
Search Strategy
In January 2024, 2 independent reviewers conducted a systematic literature search using MEDLINE, Embase, PubMed, and the Cochrane Library Database from inception till December 2023 to identify relevant papers. The search strategy was as follows: Bunionette or (Tailor’s Bunion) or ((metatarsal osteotomy) AND (Fifth)). Any disagreements were resolved through discussion.
Participants
We included patients of all ages who underwent percutaneous or minimally invasive (defined and specified as incision length <1 cm) osteotomy techniques for bunionette deformity correction. There was no exclusion based on pathology or specific operation.
Study Criteria
The inclusion criteria include English-language studies in full text that report on outcomes related specifically to percutaneous or minimally invasive osteotomy techniques for bunionette correction and the following study designs: randomized controlled trials, observational cohort studies, and case series. Our exclusion criteria were as follows: case reports, biomechanical studies, in vitro studies, and studies failing to report postoperative clinical or patient-reported outcomes.
Data Extraction
Results from the database searches were collated and duplicates removed. Papers were screened using study title and abstract and inclusion/exclusion criteria to assess suitable articles for inclusion. Full-text articles were reviewed for inclusion and citations screened to identify any additional studies. To minimize bias, data were anonymously extracted by 2 authors independently using a purpose-designed proforma with disagreements resolved with discussion.
Variables
Study characteristics were extracted including study design, numbers of patients, follow-up, country, and patient age. Study outcomes extracted include pain (visual analog scale pain score), clinical patient-reported outcomes (American Orthopaedic Foot & Ankle Society lesser toe metatarsophalangeal-interphalangeal scale), radiographic deformity correction (fourth-fifth intermetatarsal angle, fifth metatarsophalangeal angle, metatarsal shortening), technical procedural data, union rates, and complications.
Risk-of-Bias Assessment and Study Quality
The studies included in the analysis were assessed for bias within their methodology. Nonrandomized trials were assessed using the ROBINS-I tool (risk of bias in nonrandomized studies of interventions). 31 The studies were independently assessed by 2 authors and any disagreements resolved by discussion. The ROBINS-I tool is structured into 7 domains. The results are then judged on their overall risk of bias based on the responses to each domain.
Statistical Methods
All data analysis were conducted using R and Microsoft Excel. Studies that presented pre- and postoperative outcomes were included in a meta-analysis using a random effects model. Where data were presented in mean and range format, an estimate of the standard deviation to facilitate meta-analysis was performed following the technique described by Wan et al. 34 Results were considered statistically significant at a P value of <.05.
Results
A total of 942 potential studies were identified from the electronic databases search. After removing 151 duplicates, a further 698 were excluded by reviewing their titles and abstracts. We then reviewed the remaining 93 full-text articles and excluded 77 of these for reasons shown in Figure 1. We identified 16 studies and searched a further 507 citations identifying a further 2 articles for inclusion (Figure 3). The study characteristics of included studies can be seen in Table 1. All studies were retrospective case series and included 714 feet in 580 patients. There were no comparative studies identified. There were 6 main percutaneous osteotomy techniques described in the included studies (Figure 4). Most osteotomies were unfixed, with 14 of 18 studies not using fixation. The remaining 4 studies all used K-wire fixation to maintain reduction.

PRISMA flow diagram of included studies.
Characteristics of Included Studies Reporting Percutaneous Osteotomy Techniques for Bunionette Deformity Correction.

Abbreviation: n.s., not specified.

Percutaneous osteotomy techniques for correction of bunionette deformity.
Radiographic Deformity
Radiographic deformity correction was reported in all studies and shown in Tables 1 and 2 and Figure 5. There was significant improvement in both fourth-fifth intermetatarsal angle and fifth metatarsophalangeal angle.
Radiographic Deformity Outcomes of Included Studies Reporting Percutaneous Osteotomy Techniques for Bunionette Deformity Correction.

Abbreviation: n.s., not specified.

Forest plot demonstrating change in fourth-fifth intermetatarsal angle (A) and fifth metatarsophalangeal angle (B) following percutaneous bunionette deformity correction.
Clinical Patient-Reported Outcome Measures
Clinical patient-reported outcome measures patient-reported outcome measures with pre- and postoperative scores were available in 11 studies. The American Orthopaedic Foot & Ankle Society lesser toe metatarsophalangeal-interphalangeal scale score was the most frequently reported, with all studies reporting improvement (as shown in Table 3 and Figure 6).
Clinical Outcomes of Included Studies Reporting Percutaneous Osteotomy Techniques for Bunionette Deformity Correction.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society lesser toe metatarsophalangeal-interphalangeal scale; FAAM, Foot and Ankle Ability Measure; FFI, Foot Function Index; JSSF, Japanese Society for Surgery of the Foot; MOXFQ, Manchester-Oxford Foot Questionnaire; n.s., not specified; VAS, visual analog scale.

Forest plot demonstrating change in (A) American Orthopaedic Foot & Ankle Society lesser toe metatarsophalangeal-interphalangeal scale (AOFAS) and (B) visual analog scale (VAS) pain scores following percutaneous bunionette deformity correction.
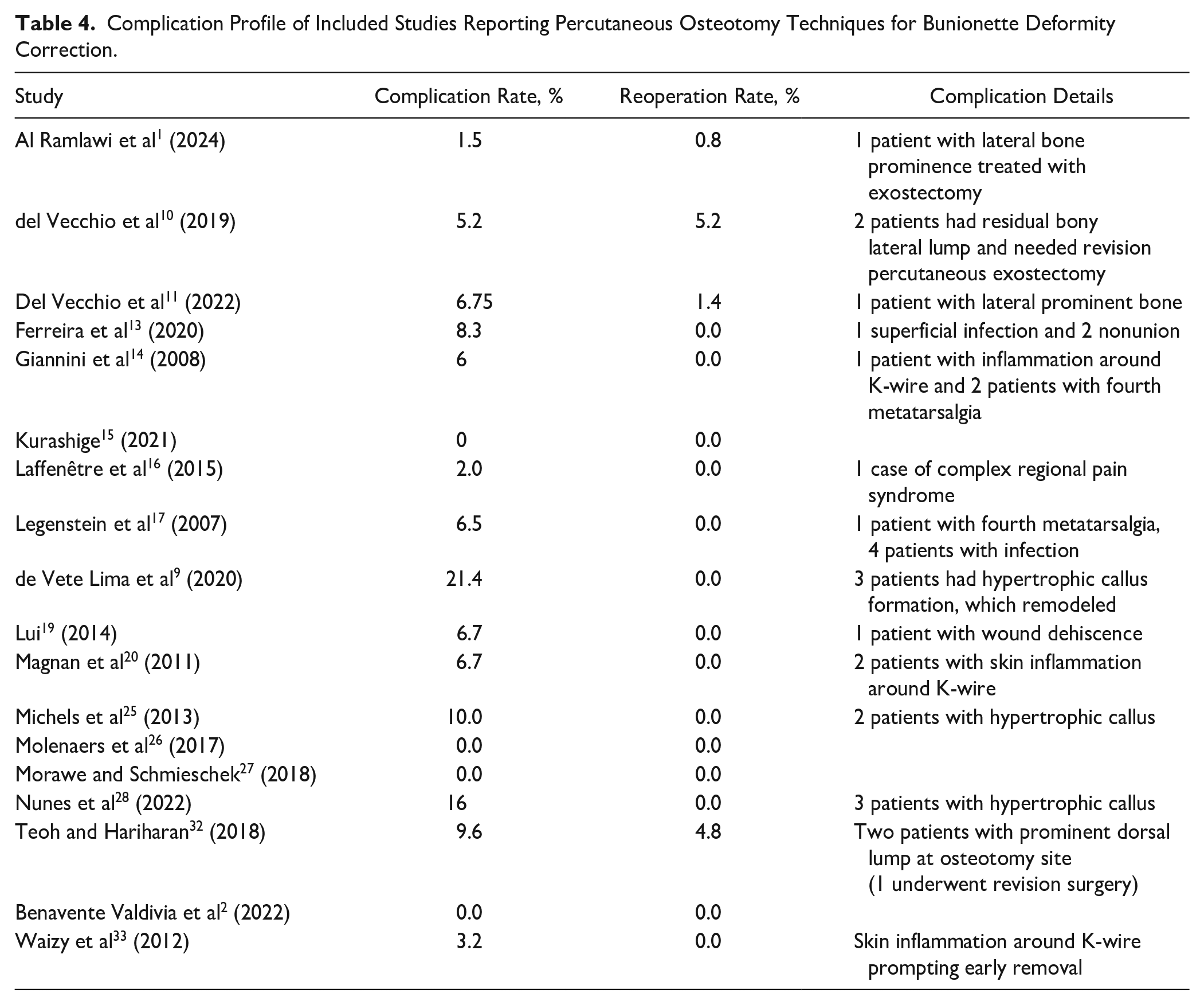
Complications
Complication data was reported in all studies. The complication rate ranged from 0% to 21.4% as seen in Table 4. The nonunion rate ranged from 0% to 5.6%. A number of studies using unfixed osteotomy techniques reported patients presenting with hypertrophic callus at the site of the osteotomy. Further breakdown of the nonunion rate found that distal osteotomies were associated with a higher rate of nonunion and hypertrophic callus formation compared to proximal osteotomies.
Complication Profile of Included Studies Reporting Percutaneous Osteotomy Techniques for Bunionette Deformity Correction.
Risk of Bias and Study Quality
All studies were assessed using the ROBINS-I critical appraisal tool as seen in Figure 7. The majority of the studies were assessed as low-moderate risk of bias. The most frequent confounder in the literature was the incorporation of additional forefoot procedures such as hallux valgus correction, which could bias the clinical outcomes.

ROBINS-I risk of bias assessment for included studies.
Discussion
The results of this systematic review suggest that percutaneous techniques for bunionette deformity correction are clinically safe and effective with significant improvement in radiographic alignment and patient-reported outcome measures. This review highlights the variability in osteotomy technique and mode of fixation. The majority of studies use a distal osteotomy technique, with only 2 studies reporting variability in the location of the osteotomy depending on deformity, for example, in types 1 and 3, surgical approach often performed distally, at the level of the neck of the fifth metatarsal. In type 2 deformities, surgical access was at or just distal to the apex of the deformity.27,28
There is currently a lack of consensus regarding the optimal osteotomy technique and method of fixation for percutaneous bunionette correction. 23 The most common percutaneous osteotomy technique currently used is a distal oblique osteotomy at 45 degrees (Table 1). The K-wire fixation was most frequently used to stabilize the osteotomy in studies using fixation but came with the increased risk of skin inflammation. In a meta-analysis of other different osteotomies to treat symptomatic bunionette, Martijn et al 21 observed a total of 48 major complications (6%), and after subdividing the complications by the osteotomy site, a greater number of complications were observed in proximal and diaphyseal osteotomies than in distal osteotomies.
The radiographic deformity correction that can be achieved with a percutaneous technique is significant regardless of type of bunionette deformity or osteotomy technique. The improvement in fourth-fifth intermetatarsal angle of 6 degrees using percutaneous osteotomy techniques was identical to that achieved using open techniques. 21 Similarly, clinical outcomes universally improved following percutaneous bunionette correction. The improvement in clinical outcomes is similar to that seen with open technique. 21
The most frequent complications observed were irritation from K-wires in fixed osteotomies14,20,33 or hypertrophic callus in unfixed osteotomies.1,9 -11,25,28,32 The hypertrophic callus is likely due to the residual instability of nonfixed osteotomies and can be easily treated if symptomatic. 28 Interestingly, 3 studies16,25,32 reported that this callus resolved without surgical intervention over time, which is a phenomenon observed by the authors of this study as shown in Figure 8.

Pre- and postoperative radiographs (Left: right preoperative, 6 weeks, 6 months, and 12 months) of a bunionette treated with percutaneous distal osteotomy demonstrating hypertrophic callus formation and subsequent resorption without further surgical intervention.
Readers should be cautious when interpreting these results because in some studies, bunionette correction was performed alongside other forefoot deformity procedures (which may bias the results) and, furthermore, the American Orthopaedic Foot & Ankle Society lesser toe metatarsophalangeal-interphalangeal score is not a validated measure. Future studies should use validated patient-reported outcome measures such as the Manchester-Oxford Foot Questionnaire in isolated bunionette deformity, ideally with a comparative group. 8
The traditional open approach to bunionette correction has been shown in multiple studies to be clinically effective at improving deformity and patient-reported outcome measures.21,35 There are, however, a number of complications associated with the open approach, including wound and hardware-related issues, in particular prominent metalwork.21,35 There is a possibility that using a percutaneous approach with an unfixed osteotomy may reduce the risk of these particular complications whereas a smaller incision may facilitate faster return to activity. Unfortunately, there are no comparative or randomized studies of open vs percutaneous bunionette correction to confirm or refute this and, instead, we rely on aggregate meta-analyses.
In a recent systematic review, Martijn et al 21 found that most complications occurred in the proximal (22%) and diaphyseal (21%) osteotomy groups, followed by the distal group (11%). They also showed that bone complications (eg, delayed union, nonunion, avascular osteonecrosis, and fracture) occurred most frequently after proximal osteotomies (9%). This study found that lower rates of complications compared with open procedures showed a higher complication rate, ranging from 6% to 27.2%. 21 These are related to stress fractures, dorsal angulation of the fifth toe, wound disorders, and osteosynthesis intolerance, among others.
Strengths and Limitations
This systematic review explored the use of percutaneous or minimally invasive osteotomy techniques for bunionette deformity correction. We have followed a systematic approach to identify all relevant studies and used validated tools for the risk of bias assessment. Our search strategy and inclusion criteria were broad to ensure that we captured all relevant studies. However, there are limitations to this systematic review owing to the methodologic limitations of the studies included—most notably the additional procedures performed at the same time as the bunionette correction. As there were no comparative studies included, it is not possible to comment on the superiority or equivalence of open vs percutaneous techniques. Other important limitations include the retrospective nature of the included studies as well as the methodologic issues associated with small case series. Finally there was substantial variability between the studies, which makes interpretation of the results challenging.
Conclusion
Based on this systematic review of a heterogenous collection of retrospective case series we found that it appears that percutaneous techniques for bunionette deformity correction clinically safe and associated with improvement in radiographic alignment and patient-reported outcome measures. There is a clear need for comparative robust methodologic studies investigating open and percutaneous osteotomy techniques for bunionette correction.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241263095 – Supplemental material for Minimally Invasive Surgery For Management of Bunionette Deformity (Tailor’s Bunion) Using Fifth Metatarsal Osteotomies: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114241263095 for Minimally Invasive Surgery For Management of Bunionette Deformity (Tailor’s Bunion) Using Fifth Metatarsal Osteotomies: A Systematic Review and Meta-Analysis by Thomas L. Lewis, Peter Lam, Yousif Alkhalfan and Robbie Ray in Foot & Ankle Orthopaedics
Footnotes
(Correction October 2024):
In the previously published version, Table 1 contained a transcribing error: the study characteristic data for Benavente Valdivia et al. was incorrectly listed under Waizy et al., and vice versa. Additionally, the citation for Valdivia et al. in Figures 5, 6, and 7 should read Benavente Valdivia et al. 2022. This error was due to the visualization software used. The meta-analysis content is correct. The corrected Table 1 and Figures 5, 6, and 7 are included in this updated version.
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.