
Abstract
Background:
Patients with poor glycemic control are at increased risk of postoperative complications. Hemoglobin A1c (HbA1c) has traditionally been used to assess preoperative glycemic control, but with limitations. More recently, fructosamine has been tested preoperatively in patients undergoing elective total joint arthroplasty. This study aims to assess whether preoperative serum fructosamine can be used to avoid adverse outcomes in patients undergoing foot and ankle surgery.
Methods:
This was a retrospective chart review of all patients who underwent foot and ankle surgeries at 2 level 1 trauma centers from January 2020 to December 2021. Of those, 305 patients were tested for HbA1c and fructosamine levels preoperatively. Adverse outcomes were assessed over 30 and 90 days. Outcomes of interest were surgical site infection, wound dehiscence, unplanned return to the operating room, unplanned readmission, and death. Data were analyzed using independent 2-sample t tests. A mixed effects model was used for multivariate analysis. P values less than .05 were considered statistically significant.
Results:
Preoperative serum fructosamine was significantly higher (P = .029) in those with complications within 90 days compared to those without. The mean preoperative fructosamine level was 269.2 µmol/L (SD = 58.85) in those who did have a complication vs 247.2 µmol/L (SD = 53.95) in those who did not. Clinically significant fructosamine threshold was determined using 2 different methods. Fructosamine was found to be non-inferior to HbA1c in accurately predicting postoperative complications.
Conclusion:
Fructosamine is a serum marker that reflects nearer term glycemic control than HbA1c. Elevation in preoperative fructosamine is associated with increased perioperative complications after foot and ankle surgery within 90 days. Preoperative fructosamine may be used in patient optimization and risk stratification when determining candidacy and timing for elective foot and ankle surgeries.
Level of evidence:
Level III, retrospective cohort study.
Introduction
It is well known within the general orthopaedic as well as foot and ankle literature that patients with poor glycemic control are at increased risk of postoperative complications. These complications include but are not limited to myocardial infarction, stroke, superficial and deep wound complications, and prosthetic joint infections.2,12,13,20 The preoperative evaluation of diabetic patients typically includes an assessment of their hemoglobin A1c (HbA1c) level. Wukich et al 24 has previously shown that HbA1c level ≥8 is an independent risk factor for surgical site infection.3,17
HbA1c is a weighted average of blood glucose over the life of a red blood cell, or 90-120 days. A patient’s plasma glucose over the preceding 30 days contributes to about 50% of the result, and 10% of the result comes from 90 to 120 days earlier. 18 In other words, the HbA1c level is dependent on the life cycle of the red blood cell and may take 3 months to reflect changes in glycemic control. Therefore, HbA1c may not accurately reflect the rapid fluctuations in a given patient’s plasma glucose level. This may result in some patients undergoing elective surgery when they are not truly optimized, and therefore at a higher risk of postoperative complications. Additionally, in the complex patient population that undergoes foot and ankle surgery, waiting 3 months to recheck the HbA1c may result in adverse outcomes for the patient, including development of wounds, infections, or further deconditioning.
Moreover, HbA1c has been shown to have a lower diagnostic performance in specific patient populations frequently encountered in foot and ankle surgery. They include but are not limited to elderly patients, non-Hispanic Blacks, male patients with hemoglobin <130 g/L, female patients with hemoglobin <120 g/L, patients with end-stage renal disease, patients with heavy alcohol use, patients with hemolytic anemia, athletes, and in those genetically predisposed to hyperglycation.5,6,9
Recently, fructosamine has been tested preoperatively in patients undergoing elective total joint replacements.21,22 It is a relatively inexpensive test performed using quantitative spectrophotometry. 11 Fructosamine measures the level of glycated serum proteins over a 14- to 21-day period. The shorter half-life of fructosamine compared to the HbA1c is reflective of the turnover of plasma proteins. This means that fructosamine can potentially give a better picture of the rapid changes in blood glucose than HbA1c can. By more accurately identifying patients with poor glycemic control, we may be able to decrease surgical site infections, readmissions, and major complications. Shohat et al21,22 has previously shown fructosamine ≥292 µmol/L to be predictive of developing adverse outcomes in arthroplasty. In their study, the high fructosamine group had higher rates of infection, periprosthetic joint infection, readmission, and reoperation.
To our knowledge, fructosamine testing has not yet been reported in foot and ankle surgery. We aimed to test the hypothesis that higher fructosamine levels would be associated with an increased incidence of postoperative complications. The purpose of this study was to determine if there is an association between fructosamine levels and postoperative complications in patients undergoing foot and ankle surgery. Secondarily, we aimed to identify a preoperative serum fructosamine value that can serve as a threshold for adverse outcomes in the perioperative period.
Methods
This study was approved by the university’s institutional review board. This was a retrospective chart review of all consecutive patients who underwent foot and ankle surgeries at 2 level 1 trauma centers from January 2020 to December 2021. Surgeries were performed by one of 3 fellowship-trained, board-certified foot and ankle orthopaedic surgeons. Medical records were reviewed to collect patient characteristics, including age, sex, body mass index (BMI), presence and type of diabetes, insulin dependence, need for dialysis, and smoking status. Current Procedural Terminology (CPT) code and laterality were recorded. Inclusion criteria was all foot and ankle procedures including but not limited to fracture fixation, mass excision, arthroplasty, deformity correction, and debridement. Adverse outcomes, as well as mortality rates over 30 and 90 days, were assessed. Outcomes of interest were wound dehiscence, superficial infection, deep infection, readmission, unplanned reoperation, and death. Exclusion criteria included patients who did not have HbA1c or fructosamine levels drawn preoperatively and patients with age <18 years. Prior to the study, an a priori power analysis was performed. It was determined that 200 patients would be needed to detect a clinically meaningful difference with an alpha level of 0.05 with a power of 0.8.
Statistical Analysis
We described our patients using summary statistics such as means, SDs, frequencies, and percentages. Independent 2-sample t tests were used to compare variables of interest between patients with and without postoperative complications. A receiver operating characteristic (ROC) analysis was conducted, and the F1-score incorporating sensitivity and specificity was calculated to determine a serum fructosamine cutoff that best predicts the complication at 30 days and any time within 90 days postoperatively. Based on the fructosamine cutoff, multivariable logistic regression was used to determine whether the serum fructosamine was a risk factor for the complication when controlling for sex, BMI, diabetes, and previous infection. A random effect was added to the logistic regression model to account for possible dependence between multiple records of the same patient. We reported an odds ratio (OR), its 95% CI, and the corresponding P value derived from PROC GLIMMIX in SAS, version 9.4 (Cary, NC), a commonly used procedure for the generalized linear mixed effects model.
Source of Funding
This research received no external funding.
Results
The records of 313 patients [55% (172/313) female; mean age 50.8 years] undergoing foot and ankle surgery were reviewed. Of those, 305 patients were tested for HbA1c and fructosamine levels preoperatively (within 14 days of surgery). The mean serum fructosamine level was 251.5 µmol/L (SD = 55.6). In addition, 43.7% (137/313) of the patients had diabetes: 41.5% with type 2 (130/313), and 2.2% (7/313) with type 1.
Within 90 days postoperatively, 61 patients [19.4% (61/313)] experienced a complication (surgical site infection, wound dehiscence, unplanned return to the operating room, unplanned readmission, and mortality). Those who experienced a complication within 90 days had a mean fructosamine level of 269.2 µmol/L (SD = 58.9), compared with the mean fructosamine level of 247.2 µmol/L (SD = 53.9) in those who did not (P = .029). The mean HbA1c was 6.15% in those who did experience a complication, vs 6.86% in those who did not (P = .004).
Forty-one of these patients had a preoperative diagnosis of diabetes and 26 of them were diagnosed with preoperative infection. This was significantly different from the cohort who did not suffer a complication within 90 days of operation. Age, sex, body mass index, race, and smoking status were not significantly different between those who had a complication within 90 days and those who did not (P = .093, .096, .098, .702, and .490, respectively) (Table 1).
Summary of Characteristic Variables by Whether There Was a Complication During 90 Days Postoperatively.

Boldface indicates significance.
We also looked at 30-day complication specifically. Within 30 days postoperatively, 41 patients experienced a complication. The fructosamine levels also differed significantly between those who experienced a complication at 30 days (271.0 µmol/L, SD = 55.2) and those who did not (248.5 µmol/L, SD = 55.1; P = .047). The mean HbA1c was 6.17% in those who did experience a complication within 30 days, vs 7.09% in those who did not (P = .002) (Table 2).
Summary of Characteristic Variables by Whether There Was a Complication During 30 Days Postoperatively.

Boldface indicates significance.
When analyzed as a continuous variable, elevated fructosamine was predictive of a postoperative complication at 30 days (OR = 1.01, 95% CI = 1.00, 1.010; P = .029) and during the entirety of the 90-day postoperative period (OR = 1.006, 95% CI = 1.000, 1.012; P = .047).
We then used 2 different methods to identify a cutoff value for preoperative fructosamine. The first method we used was similar to what Shohat et al21,22 did. In their total joint cohort, they found that fructosamine value of 292 µmol/L corresponded to the same percentile (94th percentile) as the HbA1c cutoff of 7%. In our cohort, we used HbA1c of 8% as the cutoff because it is widely used by foot and ankle surgeons in determining surgical candidacy. The cutoff corresponded to the 85.8th percentile and fructosamine value of 295.7 µmol/L.
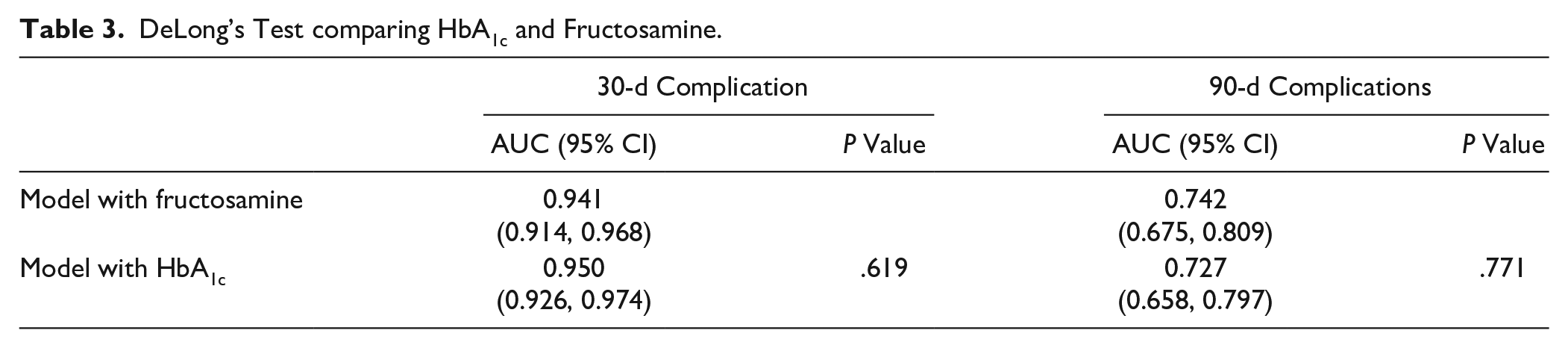
Alternatively, we also used the ROC curve to determine what we deemed may be a more statistically sound cutoff. The optimal fructosamine threshold determined by our ROC analysis was 238.5 µmol/L. Patients with fructosamine levels greater than 238.5 µmol/L are >3 times more likely to experience a 30-day complication (OR = 3.27, 95% CI = 1.60, 6.69; P = .005) and 4 times more likely to experience a complication within the 90 days (OR = 4.14, 95% CI = 1.71, 10.05; P = .006). DeLong’s test shows that fructosamine was non-inferior to HbA1c in the strength of its association with the rate of complications within 30 and 90 days, adjusting for potential confounders. Of the 176 patients who did not have a preexisting diagnosis of diabetes, 47 (26.7%) of them were found to have a fructosamine level greater than our threshold of 238.5 µmol/L (Table 3 and Figure 1).
DeLong’s Test comparing HbA1c and Fructosamine.

Receiver operating characteristic curve analysis comparing HbA1c and fructosamine, at 30 and 90 days.
We stratified our patient population based on whether their preoperative glucose control was good vs poor, as suggested by preoperative HbA1c level. In other words, the patients were grouped into 3 separate categories: those with no preoperative diagnosis of diabetes as control, those with diabetes with HbA1c level <8%, and those with diabetes with HbA1c ≥8%. The preoperative fructosamine level was found to be significantly different in all 3 groups according to 1-way analysis of variance and Tukey post hoc test (Figure 2).
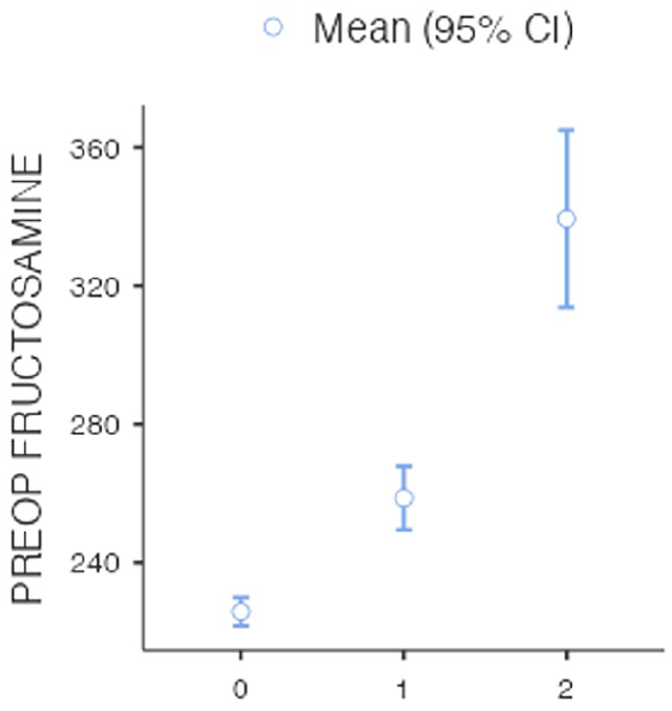
Preoperative fructosamine level based on status of diabetes (0 = no diabetes, 1 = well-controlled diabetes/HbA1c <8%, 2 = poorly controlled diabetes/HbA1c ≥8%).
Discussion
Inadequate glucose control has been associated with increased postoperative complications and patient mortality in both nonorthopaedic and orthopaedic surgical procedures.8,14,19,22 The impact of diabetes and glucose control has been well studied in arthroplasty, spine surgery, orthopaedic trauma, and arthroscopic shoulder surgery.1,3,4,10,17,23 Specifically, in foot and ankle surgery, complicated diabetes and poor long-term glycemic control (HbA1c ≥ 8%) is associated with increased risk of surgical site infection. 24 In the present study, we defined a complication as any of the following: surgical site infection, wound dehiscence, unplanned return to the operating room, unplanned readmission, or mortality. The overall complication rate in the present study [19.5% (61/313)] was consistent with other studies examining complications in a variety of foot and ankle surgeries.3,7,17
Currently, HbA1c is widely accepted and used as the preoperative screening tool for glycemic control in foot and ankle surgery. However, it is not without several limitations. First, HbA1c’s ability to predict complications other than surgical site infection in foot and ankle surgery has not been well studied thus far. Second, HbA1c has been shown to have lower diagnostic performance in pregnant women, non-Hispanic Blacks, and elderly patients. 5 Third, HbA1c is also limited by its inability to detect short-term variability in blood glucose. Rather, it reflects an average blood glucose over a 3-to-4-month period. Finally, the HbA1c level can be either falsely elevated or lowered by conditions affecting the life cycle of the red blood cell, including chronic kidney disease, chronic alcohol consumption, anemia, and acute blood loss. 9 Particularly important to the foot and ankle surgery population is chronic kidney disease, as it is highly prevalent in this surgical population, as well as is an independent risk factor for adverse outcomes. 16 Because HbA1c may not capture rapid fluctuations in plasma glucose, patients may undergo elective surgery when they are not truly optimized and are therefore at higher risk of postoperative complications. Alternatively, by waiting an additional 3-4 months to attempt to improve glycemic control and retest HbA1c, patients may be subject to unnecessary pain and functional disability while they await surgical clearance.
Fructosamine is a relatively inexpensive and accessible adjunct to HbA1c. At our institution, fructosamine costs approximately $30 and results are received within 3-5 days. Fructosamine is a measure of glycated albumin (among other glycated proteins) with a half-life of 16.5 days. This shorter half-life relative to HbA1c allows fructosamine to reflect plasma glucose levels over a short to intermediate time frame of 2-3 weeks. 5 Shohat et al 22 found that elevated fructosamine was associated with greater risk for developing periprosthetic joint infection, readmissions, and reoperations in patients undergoing arthroplasty. In our study, we also found that the mean fructosamine level was higher in patents who experienced a complication within 30 days as well as 90 days after surgery. Of the other variables, the presence of diabetes and preoperative infection were also found to be higher in patients who experienced a complication, which is to be expected.
Once we identified this association, we sought to determine an appropriate threshold for serum fructosamine that can be used clinically in determining surgical candidacy. Shohat et al20,21 used the HbA1c cutoff of 7% to determine an appropriate fructosamine correlate in percentile. According to their methodology, HbA1c of 7% corresponded to serum fructosamine level of 292 µmol/L. In contrast, we first performed univariate and multivariate analyses with fructosamine as a continuous variable. We then found the cutoff using the ROC plot as well as by mirroring their methodology, which gave us 2 different values (238.5 vs 295.7 µmol/L). We believe that the more statistically sound methodology was to use the ROC curve, as this compares the area under the curve of the HbA1c and fructosamine and their association with complications. We hypothesized that the method used in the Shohat et al21,22 paper, which is directing comparing the percentile of HbA1c and fructosamine in one particular cohort, is more likely to be inaccurate depending on the nature of the cohort. However, when we retrospectively analyzed for positive and negative predictive values of the 2 options for thresholds in our cohort, we found that the higher cutoff (295.7 µmol/L, which was the one identified using the percentile method) was more accurate. Specifically, at 30 days, the 295.7-µmol/L cutoff was correct 252 times and incorrect 61 times, whereas the 238.5-µmol/L cutoff was correct 190 times and incorrect 123 times. Similarly, within the 90-day period, the 295.7-µmol/L cutoff was correct 242 times and incorrect 71 times, whereas the 238.5-µmol/L cutoff was correct 192 times and incorrect 121 times. Interestingly, the F1 values calculated for both cutoffs are the opposite of this, showing that the higher cutoff has lower F1 value for both at 30 and 90 days (Figure 3). This may be because the data are not evenly distributed, and are not necessarily contradictory or surprising, as F1 scores may commonly be not the best index to determine “test accuracy.” Ultimately, we believe that in this data set, the higher threshold, or the one that was higher in positive predictive value, is the better threshold. In other words, one could argue that the percentile cutoff is the clinically more accurate cutoff that should be used if a surgeon were to use fructosamine to determine perioperative complication risk depending on glycemic control. However, we are including both of our methodologies for completeness sake.

F1 values for lower and higher fructosamine cutoffs at 30 and 90 days.
The current study has several limitations. The design is retrospective in nature, subjecting the results to selection bias, which was mitigated by including all consecutive patients who underwent foot and ankle surgery using CPT codes. In addition, we were unable to control for factors that might influence fructosamine levels. Any condition that alters protein metabolism like nephrotic syndrome, hepatic cirrhosis, and thyroid disease may impact the concentration of glycated proteins, potentially affecting the fructosamine level. 5 It is important to note, however, that HbA1c is affected by the same variables and confounders.
Moreover, because of the limited sample size, we were unable to perform subgroup analysis. It is likely that various types of procedures included in this study may have different rates of complications. For example, toe amputation for diabetic foot infection will inherently have higher a rate of complication than a hardware removal in an otherwise noninfected bone or total ankle replacement. This fact, however, does not undermine our data because HbA1c and fructosamine were compared under the same conditions and were found to be equally associated with complications. We specifically made the decision not to exclude patients who had preoperative infection. This is because a large proportion of the patient population who undergo foot and ankle surgery present with preoperative infection, whether that is a septic joint or diabetic foot. We believe that our results are more generalizable to the actual clinical population by including those with preoperative infection. Furthermore, because the patients with preoperative infection comprised close to 20% of our total population, we did not want to exclude them in order to keep our power and sample size sufficient. Further research in the future will be interesting with more specific inclusion and exclusion criteria based on surgery types as well as the presence or absence of preoperative infections. We still believe that our study holds value in that there is no other study looking at the association between fructosamine levels and postoperative complications.
Additionally, we did not analyze the impact of neuropathy on postoperative complications. Neuropathy has been an independent predictor of postoperative complications such as surgical site infections and nonunion.15,24,25
Finally, it is notable to mention that 47 of 176 (26.7%) patients without a preexisting diagnosis of diabetes were found to have fructosamine levels >238.5 µmol/L. It is very possible that at least some of these patients had diabetes but had not yet been diagnosed with the condition. It is a limitation of this study that we did not specifically confirm whether these patients actually had undiagnosed but clinically significant diabetes. But in the future, as fructosamine becomes more commonly used in clinical settings, we will definitely consider sending these patients for endocrinology workup. It will be interesting to conduct further studies to investigate the role of fructosamine in the initial diagnosis of diabetes, as well as its correlation with the HbA1c.
Despite these limitations, our study is, to our knowledge, the first to examine the relationship between serum fructosamine level and surgical outcomes in foot and ankle surgery. We believe that fructosamine may be a useful marker of perioperative glucose control in patients undergoing foot and ankle surgery. As previously discussed, there are several potential advantages of using fructosamine in addition to HbA1c, which warrants further investigation into its clinical utility. Although we have shown that elevated fructoasmine levels are associated with postoperative complications in foot and ankle surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241263093 – Supplemental material for Serum Fructosamine as an Indicator of Perioperative Complications in Patients Undergoing Foot and Ankle Surgery
Supplemental material, sj-pdf-1-fao-10.1177_24730114241263093 for Serum Fructosamine as an Indicator of Perioperative Complications in Patients Undergoing Foot and Ankle Surgery by Yu Min Suh, Margaret Fisher, Di Hu, Feng-Chang Lin, Dane Wukich, Josh Tennant and Trapper Lalli in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of North Carolina Institutional Review Board (#20-2700).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.