
Abstract

Introduction
Trimalleolar ankle fractures consist of simultaneous fractures involving the lateral, medial, and posterior malleolus. 3 Although there are clear indications of when to surgically repair the lateral and medial malleolus, surgical fixation of the posterior malleolus in a trimalleolar fracture has historically been disputed because of poor understanding of the size and configuration of the posterior malleolar fragment along with anatomic constraints limiting visualization. 6 Operative treatment aims to reestablish stability while restoring the articular surface of the tibial plafond. Current techniques of posterior malleolus repairs include indirect or direct open reduction and internal fixation (ORIF). These techniques allow adequate visualization of the extra-articular portion of the posterior malleolus, but they do not allow for visualization of the articular surface. Trimalleolar fractures have a worse prognosis in comparison to other rotational ankle fractures. 4 Thus, techniques improving the articular reduction are essential.
Recently, arthroscopic-assisted ORIF has been used for acute ankle fractures, 2 providing direct visualization for fracture reduction with minimal soft tissue trauma. Here, we describe a novel surgical technique for trimalleolar fractures using dry arthroscopy to directly visualize and assist with the reduction of the posterior malleolar fracture through the same incision used to repair the medial malleolus. The posterior malleolus is reduced with intra- and extraarticular techniques and fixated with the posterior-to-anterior screw construct, which is more mechanically stable than the anteroposterior lag screw construct. 1 The single, posterior-to-anterior screw construct, as used in this technique, has been shown to provide adequate fracture healing and alignment in posterior malleolus fractures. 5 Although rarely necessary, a second posterior-to-anterior screw can be used if the fragment is large enough. This technique maximizes visualization and ensures that the fragments are anatomically reduced, optimizing patient outcomes.
Technique
Example preoperative radiographs and computed tomography of a trimalleolar fracture repaired using the following technique can be seen in Figures 1 and 2. A well-padded “bean bag” is used as a bolster to place the extremity into a “sloppy” lateral position. All vital structures and bony prominences are well-padded and protected. A padded tourniquet is applied over the proximal thigh.

Example (A) anteroposterior and (B) lateral radiographs of a trimalleolar ankle fracture repaired using the described dry arthroscopic technique.

Preoperative computed tomography scan images of (A) axial, (B) coronal, (C) lateral sagittal, and (D) medial sagittal of a trimalleolar ankle fracture repaired using the described dry arthroscopic technique.
The lateral malleolus is approached through a longitudinal incision along the posterior edge of the lateral malleolus. The lateral malleolus in all cases is fixed in a standard fashion with a contoured fibular plate (Figure 3). Then, a curved incision is made over the medial malleolus to begin the posterior malleolus reduction and repair. Blunt dissection is performed down to the periosteum, protecting the saphenous vein and nerve. The medial malleolar fracture is directly visualized. It is then displaced, and one K-wire is placed into the deltoid insertion point on the talus and another into the distal tibia. A pin spreader is then used to open the talocrural joint (Figure 4). Hematoma is evacuated to directly visualize the posterior plafond impaction. Working through the initial lateral incision, a window is made between the peroneal tendons and the flexor hallucis longus, protecting the sural nerve. If needed, a freer elevator is placed into the posterior fracture between the posterior malleolus and the plafond. The freer can be used to reduce fragments “from above.” Fragments can be also be slowly disimpacted from within the joint with small reduction picks and elevators. After manual disimpaction, a 2.7 mm 30° arthroscope is placed through the displaced medial malleolar fracture to directly visualize the alignment of the intra-articular fragments (Figure 5). The alignment of fragments was considered adequate as seen in Figure 6. Once the articular fragments have been provisionally realigned, the main portion of the posterior malleolus is reduced with a ball spike pusher (Figure 7). This “fine tunes” the reduction obtained by ligamentotaxis through the lateral malleolus reduction, taking caution to avoid overreduction.

Anteroposterior fluoroscopy with lateral malleolus plate in place.

Lateral fluoroscopy showing a pin spreader being used to open the talocrural joint.
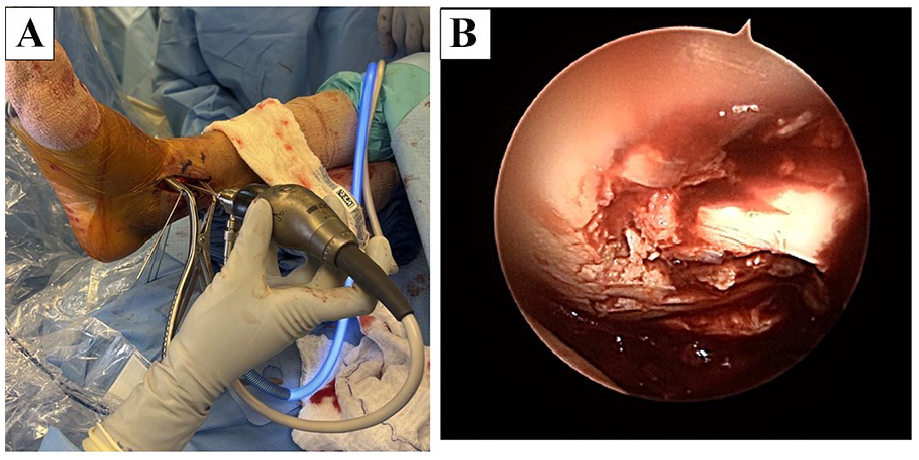
(A) Intraoperative image showing the arthroscope orientation with respect to the pin spreaders through the medial malleolus incision. (B) Dry arthroscope image showing the pre-reduction posterior plafond intraarticular fragments.

Lateral (A) fluoroscopy image and (B) dry arthroscopy image showing the fragment positioning following arthroscopic disimpaction.
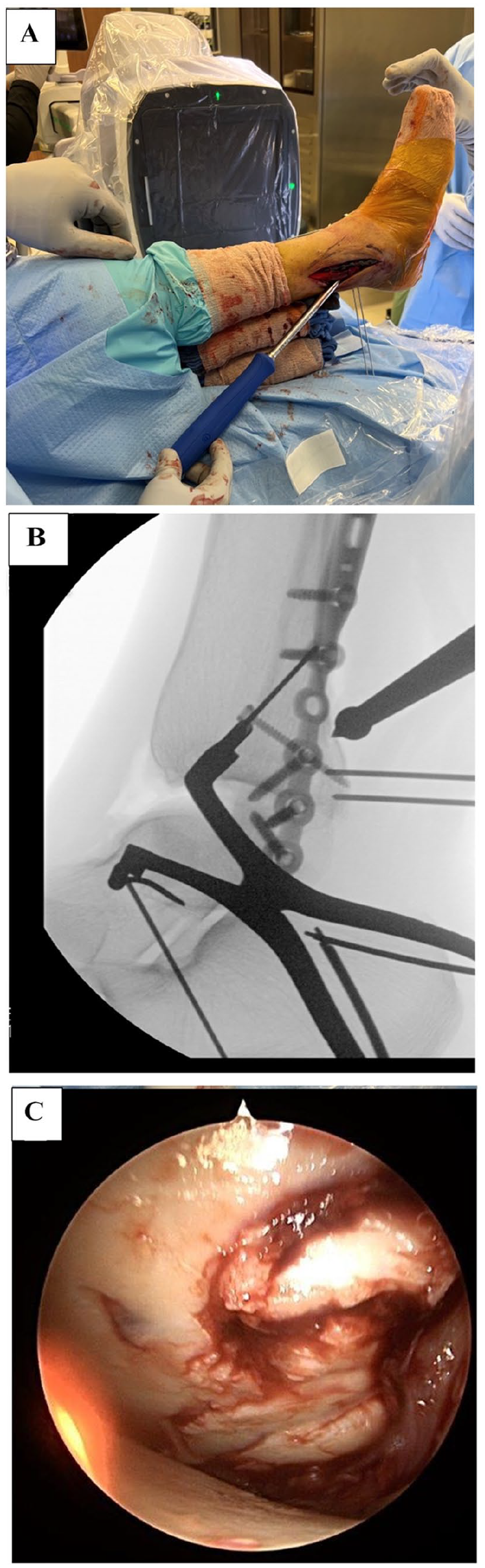
(A) Intraoperative image showing placement of the ball spike pusher through the lateral incision. Lateral (B) fluoroscopic and (C) arthroscopic images show the ball spike pusher provisionally realigning the main portion of the posterior malleolus fracture.
After adequate alignment of the articular fragments and the main portion of the posterior malleolus, 2 guide wires are advanced through the posterior lateral approach across the fracture to control rotation during screw placement (Figure 8A). A cannulated screw can be placed through the posterior window between the peroneal and flexor hallucis longus tendons or through a separate incision just lateral to the Achilles tendon, depending on fracture morphology (Figure 8, B and C).
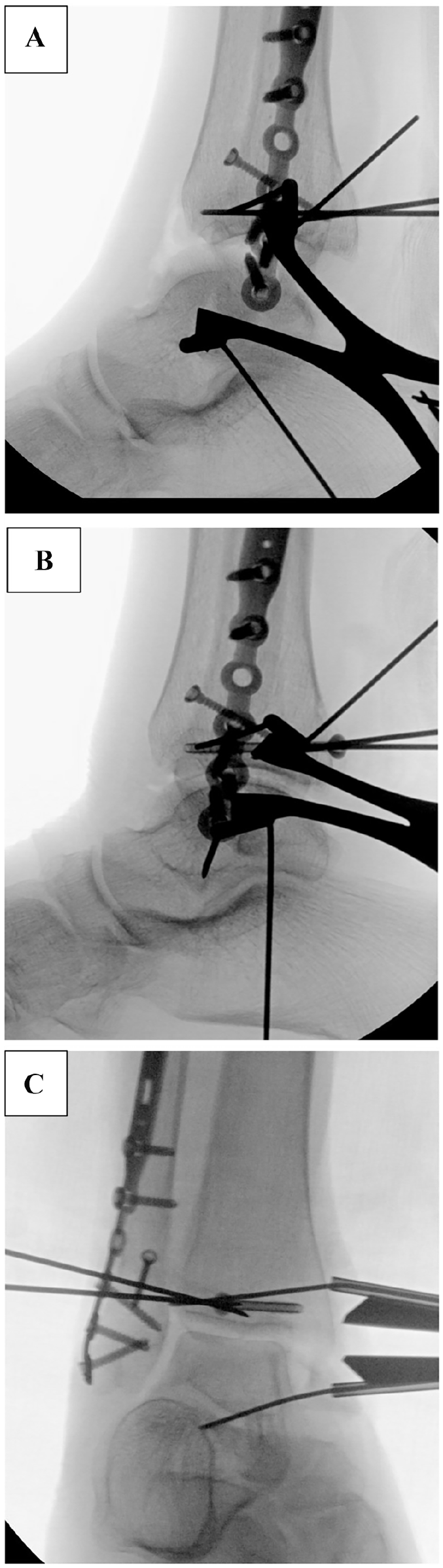
(A) Lateral fluoroscopic view showing the 2 guidewires advanced through the posterior lateral approach across the fracture line. (B) Lateral and (C) anteroposterior fluoroscopy images show the cannulated screw advanced through the posterior window.
If using a separate incision, a small incision is made just lateral to the distal Achilles tendon, and blunt dissection is performed to protect the sural nerve. The second wire is placed through this incision just above the articular surface. Once adequate wire position is confirmed with fluoroscopy, the cannulated screw is placed. Prior to compressing the posterior malleolus, the intra-articular fragments are held in position with a freer elevator or using the talus articular surface as a template by removing all distraction. The screw is tightened, taking care not to crack the posterior malleolus. This holds the intra-articular fragments through a “press-fit” technique. Final inspection is performed with the dry arthroscopic technique, and the stability of the fragments is ensured after the posterior malleolus lag screw is advanced. The medial pins are removed, and the medial malleolus is then reduced and fixated in a standard fashion. The syndesmosis is stressed and repaired in a standard fashion if needed. Final fluoroscopic imaging and computed tomography images can be seen in Figures 9 and 10.

Final (A) anteroposterior and (B) lateral fluoroscopy images following medial pin removal and medial malleolus reduction and fixation.
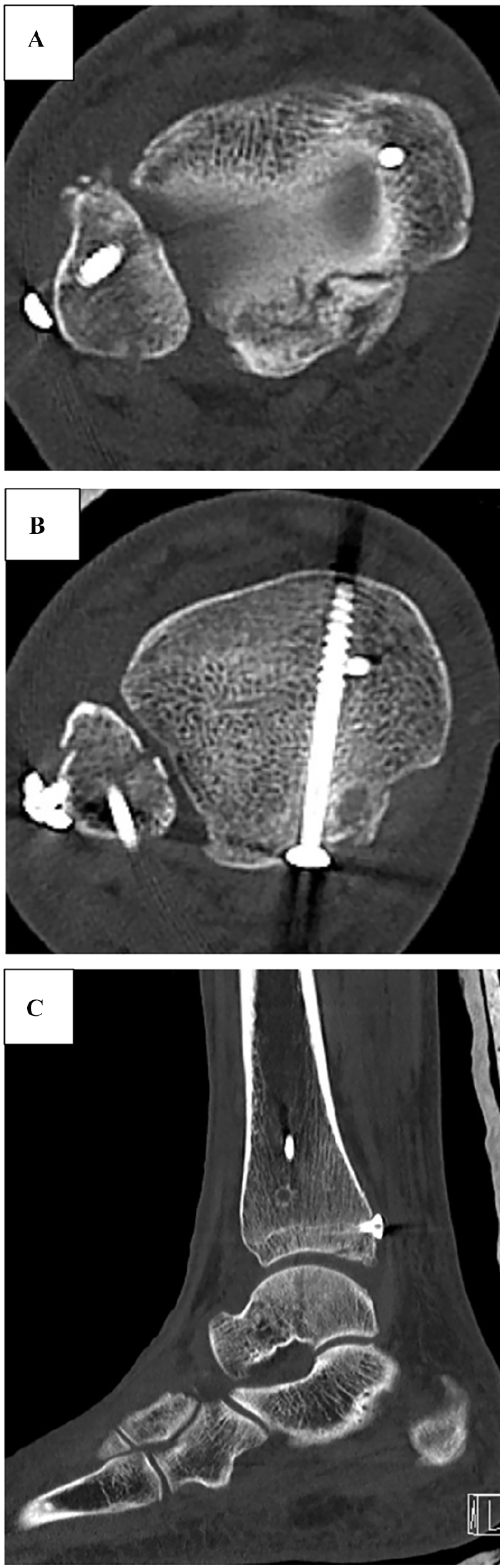
Postoperative computed tomography of the repaired trimalleolus fracture in the (A) distal axial, (B) proximal axial, and (C) sagittal planes.
Discussion
The dry arthroscopy technique described above allows for direct visualization of the posterior malleolus fracture that is superior to standard techniques. With increased visualization of fracture fragments, the articular surface can be repaired with accuracy, which may lead to lower risks of post-traumatic arthritis and improved function. 7
A limitation to this technique to repair the posterior malleolus is that the medial malleolus must also be fractured in order to obtain visualization with the arthroscope. Although standard arthroscopic techniques can be used when the medial malleolus is not fractured, that is not the focus of this technique article. The risks and limitations of this nontraditional technique are likely lower than traditional arthroscopic techniques, as the risk of fluid extravasation does not exist. In addition, any surgeon can use a dry arthroscopic technique without additional, formal training. Surgical time is minimally increased, and there is a learning curve for this technique compared with ORIF alone. However, articular reduction may be obtained by use of this technique. Although the extra-articular posterior malleolar fracture site is directly visualized through the standard posterior lateral approach, surgeons may struggle to obtain adequate reduction of the articular surface. In addition small articular, intercalated fragments are usually not reduced adequately without direct manipulation. Because the same incision sites from the medial and lateral malleolus repair are used, there is a minimally increased risk of postoperative complications. This technique should be considered for any patient with trimalleolar fracture with a complex posterior malleolar component with displaced articular fragments. No complications specific to this technique have been encountered to date. Future work should compare long-term patient outcomes between this technique and standard repair techniques.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241258098 – Supplemental material for Reduction of the Posterior Malleolar Component of Trimalleolar Fractures Using Dry Arthroscopic Visualization and Manipulation by Working Through the Medial Malleolus Fracture
Supplemental material, sj-pdf-1-fao-10.1177_24730114241258098 for Reduction of the Posterior Malleolar Component of Trimalleolar Fractures Using Dry Arthroscopic Visualization and Manipulation by Working Through the Medial Malleolus Fracture by Christopher Warburton, Olivia F. Perez, Jacob L. Cohen and Steven D. Steinlauf in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.