
Abstract
Background:
In foot and ankle surgery, adequate surgical exposure often requires multiple incisions to be used near one another, thus creating a skin bridge. As the skin bridge becomes narrower, the wound edge vitality is potentially compromised and therefore the wound’s ability to heal. The impact of local, host, and surgical factors on wound healing are well documented in the literature; however, little is known about the role of the skin bridge. The aim of this study is to determine if there is a recommendable safe skin bridge in elective foot and ankle surgery.
Methods:
A prospective study was performed on 56 patients with 60 feet who had elective foot surgery. The length of each incision and distance between the incisions were recorded. The wounds were assessed for complications at 2, 4, and 6 weeks after surgery. Patient demographics and host risk factors were documented.
Results:
The average incision length was 5.5 (range: 3-8.5) cm. The average skin bridge was 3.9 (range: 2-6.8) cm. Five (8.3%) of the 60 feet developed a wound complication. Four (80%) of these patients had a known comorbidity. Two patients had diabetes and 2 were smokers. The incidence of relevant comorbidities was 5.5% (n = 3) for patients without a wound complication (P < .001). Age did not differ significantly between patients with and without a wound complication. Patients with a wound complication had significantly longer incision lengths (P = .047). There was no significant independent association between skin bridge width and risk of wound complications (P > .05) with skin bridge widths of 2 cm or larger.
Conclusion:
In this relatively small cohort of 60 elective operative foot surgeries, we did not find increased wound complications in skin bridges 2 cm or larger, when meticulous surgical technique is practiced and host risk factors are optimized.
Level of Evidence:
Level III, prospective case control study.
This is a visual representation of the abstract.
Keywords
Introduction
Attinger et al 1 described 4 principles that need to be adhered to when performing surgical incisions in and around the foot and ankle. These principles are that the incision should (1) provide adequate exposure, (2) maintain soft tissue perfusion on either side of the wound, (3) spare sensory and motor nerves, and (4) be placed parallel to tension lines. 1 Additionally, surgical procedures around the foot and ankle require meticulous soft tissue handling, with avoidance of soft tissue stripping and excessive retraction, and often necessitates more than 1 incision for adequate exposure. 8 The distance between 2 incisions is termed the skin bridge. The skin bridge is of great importance, as a skin bridge that is too narrow poses a threat to the perfusion of that skin area and thus may compromise the wound’s ability to heal.1,2,9 Devitalized wound edges put the surgical site at risk of a host of complications, including wound dehiscence, skin necrosis, and superficial and deep sepsis.
The acceptable skin bridge width to avoid such complications in elective foot and ankle surgery has been a controversial topic, with current guidelines being derived from evidence reported in surgical trauma management around the ankle.9,14 These data are largely irrelevant in elective foot and ankle surgery as traumatic injuries around the foot and ankle require specific management of the traumatized soft tissue first, by staging the management to allow the soft tissue to recover. 21 In nontraumatized elective cases, the skin and underlying tissue has not been subjected to a primary injury and therefore should be able to tolerate and heal with a relatively narrower skin bridge. 2
There are well documented local, host, and surgical factors that influence wound healing. Although many of these have been extensively researched and invaluable in understanding the capacity for surgical wounds to heal, there is no literature to date regarding the impact of the distance between 2 or more incisions in elective foot and ankle surgery.
The commonly used “safe” skin bridge in foot and ankle surgery is 7 cm or more. This was first mentioned in 1979 in the second edition of the AO trauma manual 18 and has been echoed in numerous subsequent publications since then as an arbitrary safe distance 21 without substantial scientific backing. This traditional practice has come under recent scrutiny in the literature, with a prospective cohort concluding that skin bridges used in pilon fractures can be as narrow as 5 cm without significant risk of wound complications. 9 Because of the paucity of relevant literature on the topic, this measurement was adopted in elective foot and ankle surgery.
The aim of this study is to determine if a safe skin bridge in elective foot surgery can be determined.
Materials and Methods
A prospective study of patients who underwent elective foot surgery at a single institution was performed. Approval was obtained from the local ethics committee.
All the patients aged >18 years who had elective foot surgery requiring more than 1 incision were included. Patients who had previous surgery or trauma to the foot were excluded. Demographic data included age, gender, medical comorbidities, and smoking history (Table 1). Procedure-related data included procedure performed, number of incisions, skin bridge width, incision length, and tourniquet time (Table 2). The study included 56 patients, 40 female and 16 male, with a total of 60 feet. The mean age of the patients was 52 (range: 26-78) years.
Patient Demographics and Comorbidities.

Procedures Performed With Number of Incisions, Skin Bridge Width, Incision Length, and Tourniquet Time per Procedure.

Abbreviations: MP, metatarsophalangeal; MT, metatarsal; PVNS, pigmented villonodular synovitis; TMT, tarsometatarsal.
All surgeries were performed by 2 senior foot and ankle surgeons. Skin preparation and draping techniques and wound closure in layers were generally uniform for all the cases. All forefoot procedures were dressed using a wool and crepe bandage whereas mid- and hindfoot procedures were immobilized in a below-knee plaster backslab. Patients were instructed to elevate the foot above the heart level for the first 2 weeks to minimize swelling. Patients who had forefoot surgery were allowed to weightbear as tolerated in a forefoot-offloading wedge shoe at day 1 after surgery. Patients who had midfoot and hindfoot surgery were nonweightbearing for a period according to the specific procedure they had.
Incisions Used for Common Procedures
Below we describe the incisions made for common procedures in the foot. Depending on the presenting pathology, various combinations of these incisions are used. Table 2 presents the procedures performed with associated incision parameters.
1. Forefoot a. Hallux metatarsophalangeal (MP) fusion: Dorsomedial incision over the MP joint. This incision is commonly made just dorsal to the junction between dorsalis pedis and medial plantar angiosomes. b. Hallux valgus correction: i. Long chevron and scarf osteotomy: First metatarsal (MT) medial border incision (commonly placed at the junction between the dorsalis pedis and medial plantar angiosomes) and a first web incision (within the dorsalis pedis angiosome). ii. Lapidus: First MT medial border incision (commonly made at the junction between the dorsalis pedis and medial plantar angiosomes), a first web incision (within the dorsalis pedis angiosome), and a dorsal incision across the first tarsometatarsal (TMT) joint (placed within the dorsalis pedis angiosome).
c. Lesser toes and neuromas: Second and third toes are approached through a second web incision. Fourth and fifth toes are approached through a fourth web incision. All these incisions are made within the dorsalis pedis angiosome.
2. Midfoot a. First TMT fusion: Dorsomedial incision across the first TMT joint. This incision is made just dorsal to the junction between the dorsalis pedis and medial plantar angiosomes. b. Second and third TMT fusion: Dorsal incision between the second and third TMT joints. The incision is made within the dorsalis pedis angiosome. c. Fourth and fifth TMT excision arthroplasty: Dorsolateral incision between the fourth and fifth TMT joints. The incision is made within the dorsalis pedis angiosome. d. Navicular-cuneiform fusion: Medial incision across medial navicular cuneiform joint (at the junction between the dorsalis pedis and medial plantar angiosomes) and a dorsal incision across the middle navicular cuneiform joint (made within the dorsalis pedis angiosome).
3. Hindfoot a. Triple fusion: Dorsal incision across the talonavicular joint in line with the lateral border of the second MT (made within the dorsalis pedis angiosome) and lateral sinus tarsi incision across the subtalar and calcaneocuboid joints (made at the junction between lateral calcaneal and anterior communicant angiosomes extending distally to the junction between the lateral planar and dorsalis pedis angiosomes). b. Calcaneal osteotomy and lateral column lengthening osteotomy: Oblique incision directly posterior to the peroneal tendons (made at the junction between the lateral calcaneal and anterior communicant angiosomes) and longitudinal incision centered over the angle of Gissane (at the junction between the lateral calcaneal angiosome and both medial calcaneal and lateral plantar angiosomes).
Patients were followed up at week 2, 4, and 6 after surgery to assess for wound complications. Wound exposure was performed at each visit and the wound assessed for any signs of complications, which were then classified according to the Gililland et al 7 classification: grade 1, suture line erythema or exposed suture material; grade 2, delayed wound healing due to a seroma, hematoma, skin necrosis or exposed suture; grade 3, wounds requiring more than 12 weeks of wound care, vacuum dressings, or return to operating room.
Statistical Analysis
Power analysis was assessed using sample size estimation for descriptive studies from a 95% CI formula. A proportion of 15% was estimated from a review of cases over the proposed time period with a precision of 5%. Thus, the sample size was calculated to be 49. Descriptive data are reported as medians and interquartile ranges for continuous data (because of the small sample size, nonparametric tests were performed) and proportions for categorical data. Mann-Whitney U tests compared incision length and bridge distance between patients with and without a wound complication. Chi-square tests assessed the association between wound complication and sex and comorbidities. A logistic regression model was fitted to determine the association between skin bridge width and risk of wound complications, incision length and wound complications, and type of procedure and wound complications.
Results
The average incision length was 5.5 cm (SD = 1.4), ranging from 3 cm to 8.5 cm. The average skin bridge was 3.9 cm (SD = 1), ranging from 2 to 6 cm.
Five of the 60 feet (8.3%) developed a wound complication. Two patients had forefoot surgery and 3 patients had midfoot surgery. Three developed a grade 1 complication at week 2 (2 had mild erythema and 1 had small blisters), 1 developed a grade 2 wound complication at week 2 (superficial infection managed with local dressings), and 1 developed a grade 2 complication at week 4 (superficial infection requiring oral antibiotics). Four (80%) of these patients had a known comorbidity. Two patients had diabetes and 2 were smokers. The incidence of relevant comorbidities was only 5.5% (n = 3) for patients without a wound complication (χ2 = 24.72, P < .001). Age did not differ significantly between patients with and without a wound complication (Table 3). There was no association between wound complication and gender (χ2 = 1.98, P = .159). The mean tourniquet time for all patients was 113 minutes (SD = 20.39). The mean tourniquet time for patients who developed a wound complication was 115 minutes (SD = 7.07) vs 113 minutes (SD = 20.90) for patients who did not develop a wound complication. There was no statistically significant difference in mean tourniquet times between the 2 groups (P = .900).
Comparison Between Incision Length, Skin Bridge, and Age and Impact on Wound Complications.

Table 4 shows the results of the univariable and multivariable logistic regression showing the association between skin bridge, incision length, and risk of wound complications. The models show that there was no significant independent association between skin bridge width and risk of wound complications, as well as type of procedure and wound complications. (P > .05). However, there was a significant adjusted association between incision length and risk of wound complications (P = .047); that is, patients with a wound complication had a longer wound incision. No trend toward increased wound complications was identified in skin bridges 2 cm or larger in size.
Association Between Skin Bridge, Incision Length, and Risk of Complication. a

Boldface indicates significance (P < .05).
Discussion
The “safe” skin bridge to avoid wound complications in elective foot and ankle surgery has been a controversial topic, with current guidelines being derived from evidence found in surgical trauma management around the ankle.9,12,18 Although the relevance of these data in elective foot and ankle surgery is marginal, the understanding of safe skin bridges in a trauma setting does elicit some relevant considerations for this study. What has become evident in the literature is that a sufficiently wide skin bridge is important to prevent wound complications, along with numerous other factors (local, host, and surgical) that contribute to a wound’s ability to heal.1,3
Identifying these potential risk factors begins with risk stratifying a patient preoperatively by identifying systemic host factors that may compromise the wound’s ability to heal. Nonmodifiable systemic conditions such as age, renal disease, liver disease, microvasculopathy, and peripheral neuropathy have been established as risk factors. 3 More importantly, modifiable conditions such as diabetes mellitus, smoking, malnutrition, obesity, and concurrent steroid use need to be corrected or optimized prior to surgery.
A relative risk increase of 1.59-fold for postoperative infection has been described for every 1% increase in HbA1c above 7.0% in foot and ankle surgery 10 An elevated body mass index greater than 30 has also been shown to be a significant risk factor for wound complications and postoperative infections. 20 The proposed mechanisms for this include diminished tissue perfusion and oxygen delivery and impaired immune function. 20 Impaired wound healing due to malnutrition is also well described and is qualified and quantified with laboratory tests, including a serum albumin of <3.5 g/dL (35 g/L), transferrin of <200 mg/dL, and a total lymphocyte count of <1500 mm3. 5 Tobacco smoking has been associated with massively increased rates of wound complications, with one retrospective cohort reporting a wound complication rate of 36.4% in smokers undergoing forefoot surgery compared to a rate of 8.5% for nonsmokers. 17 Cessation of smoking 6 weeks prior to surgery and for at least 3 months after surgery diminishes a patient’s risk for postoperative wound complications. 19 These modifiable and nonmodifiable host risk factors were evident in the current study as 4 of the 5 patients who had wound complications had comorbidities (2 smokers and 2 diabetes patients).
Intraoperative factors that have been shown to have an impact on wound healing include duration of the procedure, tourniquet inflation time, prophylactic antibiotic use, skin preparation solution, and soft tissue handling.4,13,15 Rates of wound complications increase with surgical duration and tourniquet time over 90 minutes. 4 The current study found no correlation between tourniquet duration and risk of wound complications. Interestingly, the method of wound closure with staples, interrupted nonabsorbable sutures, or subcutaneous absorbable sutures showed no significant difference in rates of wound dehiscence, inflammation, discharge, necrosis, allergic reaction, or superficial infection.6,11,22
With regard to the actual placement of incisions, angiosomes of the foot and ankle are frequently taken into consideration for planning purposes. An angiosome is a block of tissue (skin, subcutaneous tissue, fascia, muscle, and bone) that is fed by the same source artery. There are 6 distinct angiosomes in the foot and ankle arising from the 3 main arteries (Figures 1 and 2). 1

Angiosomes of the foot and ankle.

Arterial supply of the foot and ankle.
Based on this model, the safest incisions in patients with a normal blood supply are those made between the watershed area of 2 adjacent angiosomes. This leaves the tissues on either side of the incision with intact blood supplies. Incisions outside of these junctions create devascularized islands with compromised blood supply, which may result in compromised wound healing. Therefore, incisions along the central raphe of the Achilles tendon, glabrous junction on the lateral aspect of the foot, and along the midline of the sole of the foot are ideal incisions when utilizing this principle.1,2
An exception to this rule was proposed by Attinger et al1,2 in the forefoot where there are numerous and extensive anastomoses between the dorsal and plantar arteries. This arterial network, they suggested, should provide adequate perfusion to surgical wounds in the forefoot with relatively narrow skin bridges even if made outside of the angiosome junctions. Findings in the current study support this hypothesis as the incisions at the forefoot were frequently made outside of the angiosome junctions with skin bridges as narrow as 2 cm with no associated increased risk of wound complications.
Angiosome-based incisions are not always possible as they may not allow for adequate exposure to perform certain procedures. Hammit et al 8 reported on a prospective case series of 17 patients who underwent a Dwyer calcaneal osteotomy and peroneal tendon repair and/or lateral ankle ligament reconstruction using dual incisions instead of the traditional single incision. The average skin bridge was 2.3 cm, with one of the 17 patients developing wound dehiscence that resolved after 10 days with oral antibiotics. These authors proposed that vascular anatomy should be taken into consideration when planning skin incisions but not dictate skin incision placement. Our results echoed these findings, suggesting that skin incisions with relatively narrow skin bridges that are placed away from angiosome junctions still maintain the ability to maintain vascularity and vitality, allowing adequate wound healing.
The probable reason for incisions made outside of the junction between 2 angiosomes being able to remain vascularized and heal is due to choke vessels becoming patent. Choke vessels are arterial-arterial connections at watershed areas that offer a neighboring angiosome a safety conduit should its primary source artery become compromised. Choke vessels take between 3 and 10 days to become patent once adjacent blood flow ceases, during which time the incision is at the highest risk of ischemia-related wound complications (Figure 3).1,2,16 The choke vessel mechanism along with the abundant anastomotic blood supply of the foot may explain why this study found no increased rate of wound complications with skin bridges as narrow as 2 cm. We did, however, identify a trend in increased wound length increasing the risk of developing a wound complication irrespective of the skin bridge size. This finding may be due to the fact that longer incisions are required for more extensive pathology, which in turn requires more soft tissue stripping.
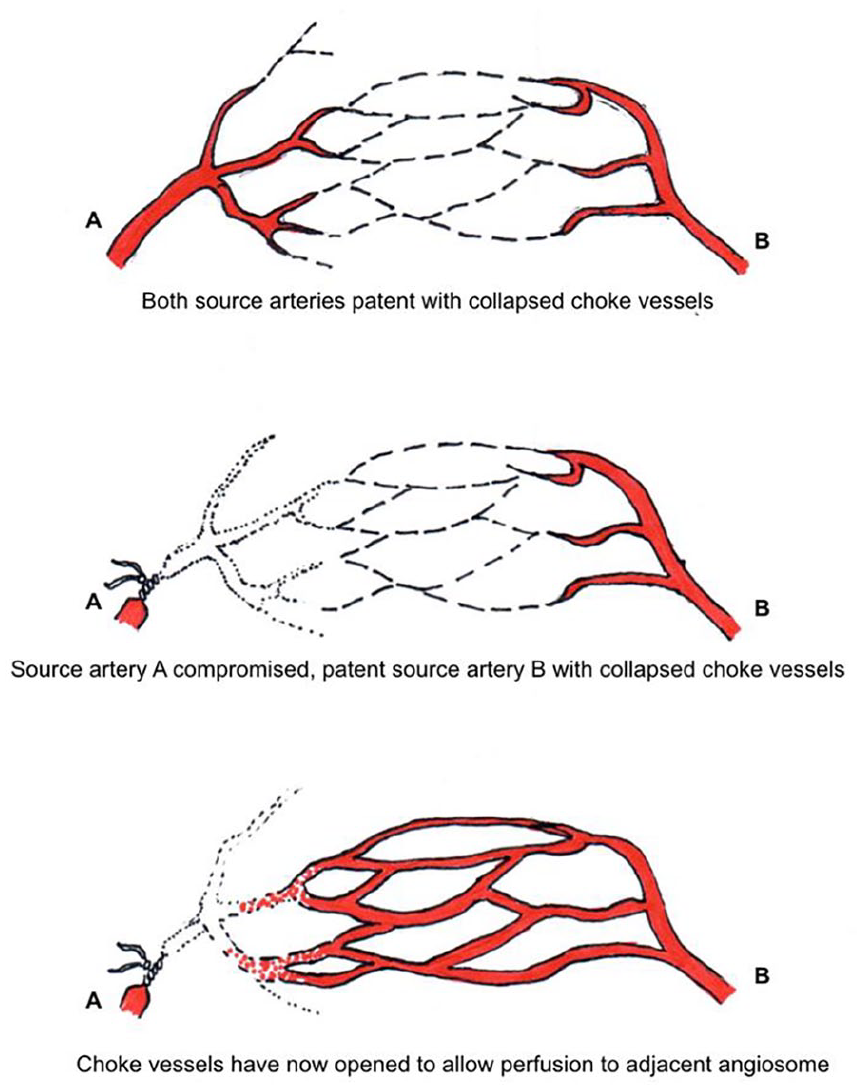
Choke vessels.
The limitation of this study is the relatively small cohort size. A larger cohort may elicit a stronger correlation between skin incision length, skin bridge, and wound complications.
Conclusion
Consideration of the vascular anatomy of the foot and ankle is vital in surgical planning, but the foot does seem to be able to compensate for and tolerate skin incisions placed in relatively close proximity to each other. The current study found no trend toward increased wound complications with skin bridges 2 cm or larger. When meticulous surgical technique is practiced and host risk factors optimized, a skin bridge width of 2 cm may be safe in elective foot surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241256552 – Supplemental material for A Prospective Evaluation for a Possible Safe Skin Bridge in Elective Foot Surgery
Supplemental material, sj-pdf-1-fao-10.1177_24730114241256552 for A Prospective Evaluation for a Possible Safe Skin Bridge in Elective Foot Surgery by Graeme Moore, Nikiforos P. Saragas and Paulo N. F. Ferrao in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Witwatersrand Human Research Ethics Committee (Clearance Certificate No. M2210102)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.