
Abstract
Background:
Diabetic foot ulcers (DFUs) are serious complications that induce a high risk of lower extremity amputations and mortality. Compared with the standard of care, few reports analyzed the outcome of surgical treatment mainly for diabetic toe deformities and ulcers. The aim of this study is to collate evidence on the outcomes of interphalangeal resection arthroplasty (IP-RA) in preventing and treating diabetic toe ulcers distal to the metatarsophalangeal joint.
Methods:
A search strategy has been developed including electronic databases from inception. Only ulcers distal to the metatarsophalangeal joints were included. Noninfected and infected ulcers were also included at any toe location (dorsal/side/plantar). Outcomes were defined as healing rate, time to heal, ulcer recurrence, ulcer transfer, postintervention infection, wound dehiscence, and additional surgeries including amputation. Proportional meta-analysis was conducted for frequency outcomes.
Results:
Six observational studies comprising 217 patients with 244 IP-RA procedures were included. The mean follow-up period was 23.4 ± 8.2 months. Weighted frequencies were as follows: healing rate (93.6%), ulcer recurrence frequency (4.3%), ulcer transfer frequency (15.4%), postoperative infection (10.5%), wound dehiscence (17.8%), revision surgery (5%), and amputation rate (3.4%). The mean healing time was 4.3 ± 1.8 weeks.
Conclusion:
This review suggests that IP-RA is effective in preventing and treating diabetic toe deformities and ulcers with a modest rate of complications for this specific and often challenging clinical presentation.
Introduction
Diabetic foot ulcers (DFUs) are known to cause severe complications, imposing higher morbidity, mortality, and health costs.3,21 Lower extremity amputations are one of the most devastating DFU complications yielding, even following minor amputations, high mortality rates. 27 The forefoot is known to be the commonest location for DFU and diabetic foot infections (DFIs).5,17 Many articles reported the efficacy of conservative surgery when treating forefoot diabetic ulcerations and infections.24,25,29,30
Besides the flexor tenotomy procedure, few reports analyzed the outcomes of conservative surgery in the prevention and treatment of diabetic toe deformities and ulcerations.22,23,28
A previous meta-analysis reported the outcomes of joint resection arthroplasty in treating DFUs, with the majority of the included articles being related to the Keller procedure or its variant. 22 This metatarsophalangeal joint resection arthroplasty is usually based on resecting the base of the first phalanx to treat plantar forefoot or digital ulcers of the hallux. Alternatively, interphalangeal resection arthroplasty (IP-RA) has been promoted to be a reasonable method to prevent and treat digital deformities and wounds located at the proximal or distal interphalangeal joints.7,8 Ulcer location seem to impact outcomes; for example, time to ulcer healing was found to increase progressively from toe to midfoot to heel and, likewise, the ulcer healing rate was higher when located in the toes compared to the midfoot and heel location. 13 On the other hand, minor amputations were performed most frequently for toe ulcers. 13 The aim of the study was to conduct a quantitative evidence synthesis on the outcomes of IP-RA when performed for preventing and treating diabetic toe deformities and ulcers.
Methods
Search Strategy
The following databases were included in the electronic search strategy: PubMed, CINAHL, Cochrane Library, and Google Scholar, from inception to October 2023. Specific Boolean terms were used: (“arthroplasty resection” or “joint resection” OR excision) AND (foot OR toe OR phalanx OR phalangeal) AND (ulcer OR ulceration OR wound OR deformity OR claw OR hammer) AND (diabetes OR diabetic). There were no restrictions applied on language or date.
Criteria for Study Selection
Studies with comparative design, observational studies, and case series were included. Review articles and single case reports were excluded. Interphalangeal resection arthroplasty was defined as one of the following procedures: resection of the head of the proximal or the middle phalanx and/or resection of the base of the middle or distal phalanx. Dorsal, side, and plantar ulcers on the toes around the proximal or distal interphalangeal joints were included. Ulcers facing the metatarsophalangeal joint were excluded. Noninfected and infected wounds of any stage were accepted for inclusion; the presence of osteomyelitis was not a criteria for exclusion.
Screening and Selection of Literature
Two reviewers independently screened the final list of hit records generated by the electronic search. After removal of duplicates, titles and abstract were checked and potentially relevant abstracts had their full manuscripts for selection. Reference lists of each selected study was further checked for possible additional relevant studies. Disagreement on eligibility was resolved by consensus.
Types of Outcome Measures and Outcome Definition
The following frequency outcomes were looked for: healing rate, time to heal, ulcer recurrence, ulcer transfer, postintervention infection, wound dehiscence, and additional surgeries including amputation. Recurrent ulcers are ulcers that developed at the same site of the original ulcer following intervention. A transfer ulcer would be an ulcer occurring at an adjacent toe following the procedure. Because we anticipated that half the studies were comparative and the comparators were different, we reported each comparison result for each outcome, when available.
Data Collection and Extraction
In preparing this review and with the prevision of dealing with different study designs, both PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines 11 and the MOOSE (Meta-analysis of Observational Studies in Epidemiology) statement 18 were used as checklists.
An Excel sheet was prepared for data extraction and to record all pertinent details of the included studies. A joint review to produce agreed accurate data was conducted following data extraction. Demographic data of the samples, characteristics of the ulcers (type, location, and infection status), surgical technique, and follow-up duration were all reported.
Quality Assessment
The quality of the studies was assessed to detect potential sources of bias from the study design using the Joanna Briggs Institute (JBI) critical appraisal tool. 12
Data Analysis
Statistical analysis was conducted based on study type, using StatsDirect (Cambridge, UK). Pooled mean ± SD values were reported for continuous variables. Proportion meta-analysis (MA) was used to look for weighted frequencies of outcomes. Heterogeneity was assessed by the inconsistency test (I2). Whenever the I2 value was more than 50%, the random-effect estimate was selected for reporting. The 95% confidence interval (CI) values were recorded. A subgroup analysis was performed to look for outcome differences between hallux and lateral toes (hallucal vs lateral toes groups). Because no studies reported all outcomes, the z-proportion test for 2 independent groups was used for frequency results and analysis of variance for mean results.
Results
Search Results
The electronic search generated 214 hit records and 12 were deleted for duplication. Screening of the titles and abstracts yielded an initial selection of potentially 14 relevant articles. After inclusion and exclusion criteria application, only 6 studies were included. Reference list checking did not lead to additional articles. No non-English article has been identified. In total, 6 studies were retained for the meta-analysis.2,4,7,8,16,19 Figure 1 shows the PRISMA flowchart.
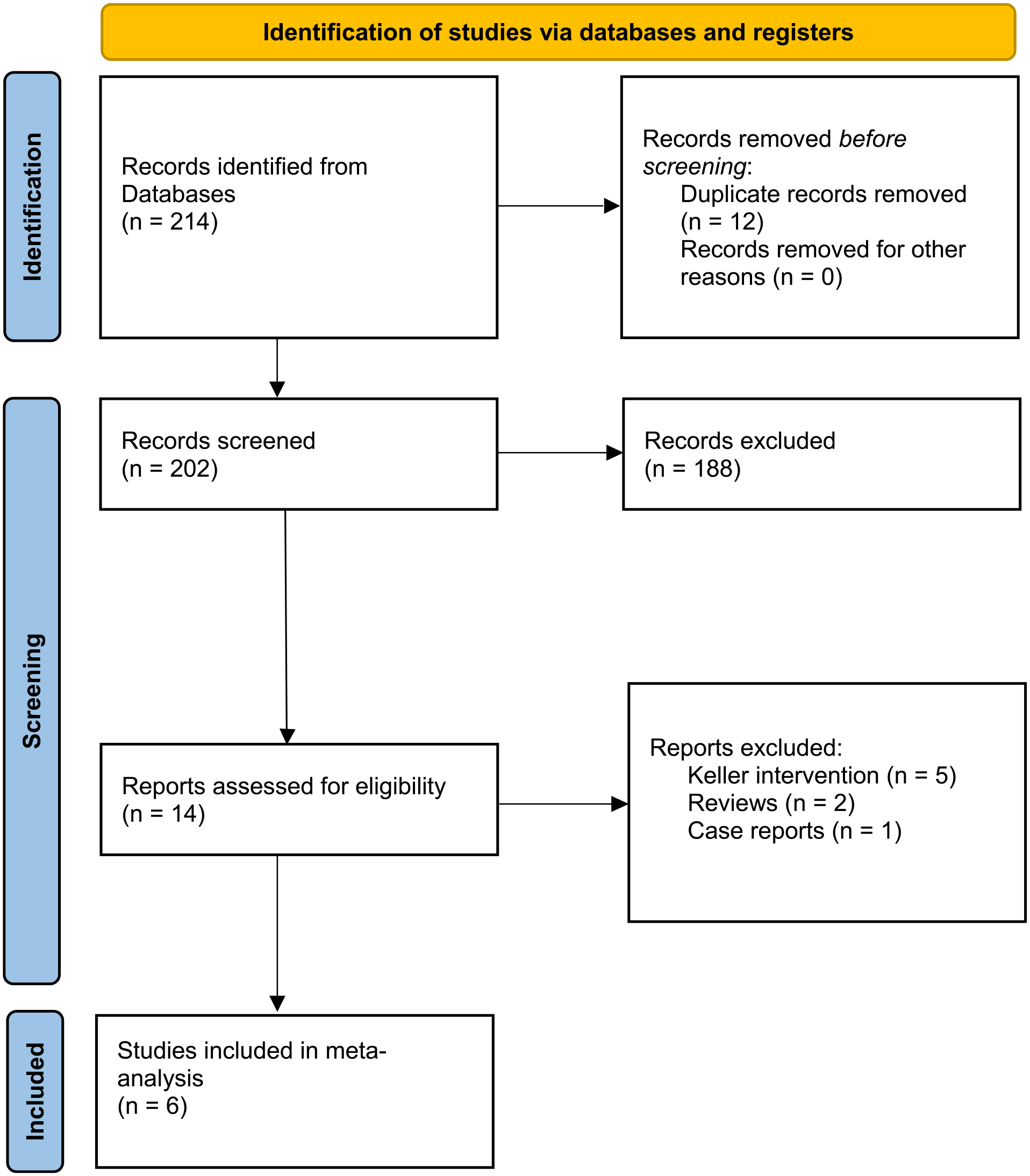
PRISMA flow diagram.
Characteristics of the Selected Studies
Of the 6 observational studies, 3 were case series and 3 retrospective comparative studies. The studies included a pooled sample of 217 patients with 244 IP-RA procedures. Armstrong et al reported outcomes of IP-RA between 3 groups; nondiabetic, diabetic without history of previous ulcers, and diabetic with history of previous ulcers. 2 Lew et al 8 reported comparative outcomes between 13 patients who underwent IP-RA and 13 controls treated with standard care, consisting of offloading with either total contact cast or modified shoes. Tardáguila-García et al 19 compared outcomes of IP-RA vs arthrodesis.
Three studies4,8,16 were limited to ulcers located in the hallux, 2 studies2,7 to the lateral (lesser) toes, and another one 19 to all toes. The mean age of the pooled sample was 59.7 ± 5 years. The mean follow-up period was 23.4 ± 8.2 months. Table 1 summarizes the characteristics of the included studies.
Characteristics of Included Studies.

Abbreviations: IPJ, interphalangeal joint; IP-RA, interphalangeal resection arthroplasty; SC, standard care; NA, not applicable; NR, not reported.
Risk of Bias Assessment
The majority of the included studies scored very well in the Joanna Briggs Institute appraisal tool, with a mean value of 8.5 of a maximum of 10. Table 2 shows details of quality appraisal for each study.
The Joanna Briggs Institute Critical Appraisal Tool.

Outcomes
Table 3 summarizes the outcomes of individual studies.
Outcomes of Individual Studies.
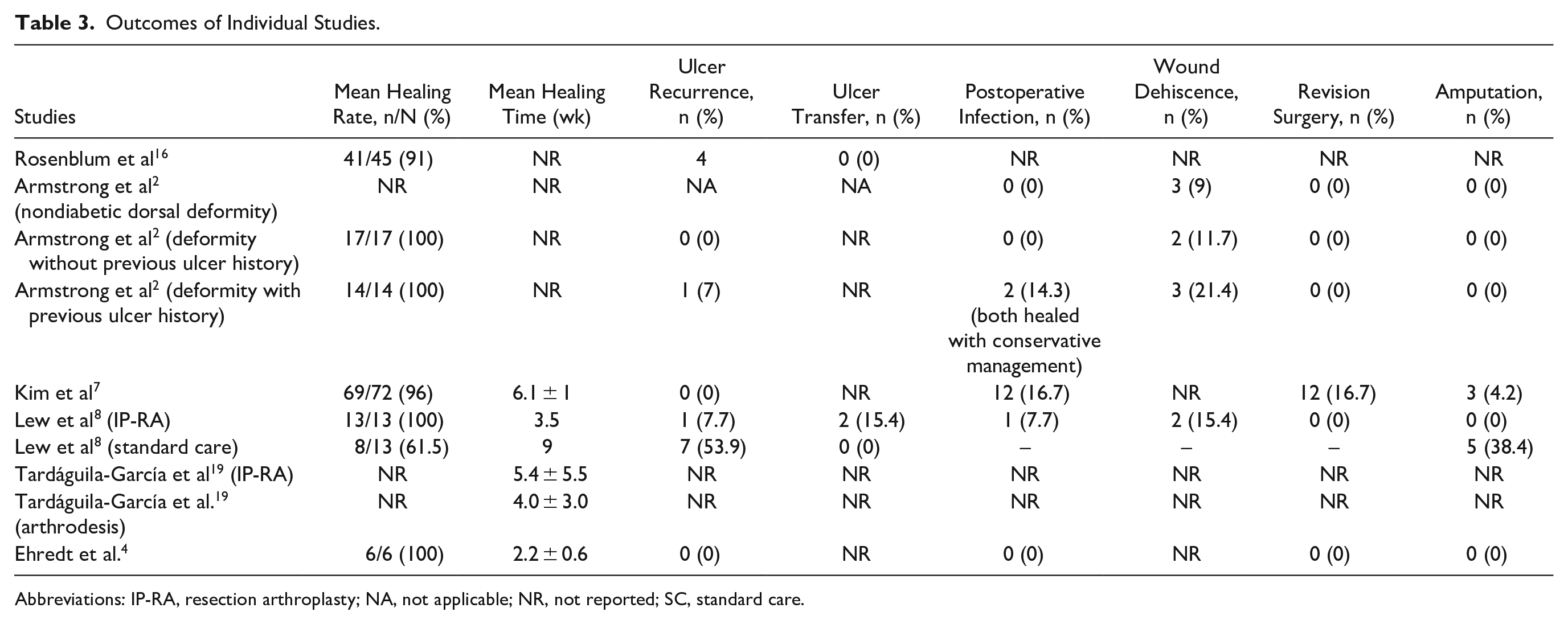
Abbreviations: IP-RA, resection arthroplasty; NA, not applicable; NR, not reported; SC, standard care.
Healing frequency
Five studies2,4,7,8,16 reported the healing rate with a pooled frequency of 93.6% (0.889 to 0.970, I2 = 11.6%). Armstrong et al 2 demonstrated no difference in healing between patients having a toe deformity with previous ulcer history compared with those without. Lew et al 8 found a difference in favor of the IP-RA group vs standard care (P = .06).
Healing time
Four studies reported on time to ulcer healing,4,7,8,19 with a mean pooled period of 4.3 ± 1.8 weeks. Lew et al 8 reported the comparative results between IP-RA and standard care, with a significantly longer time for the latter (P = .03). Tardáguila-García et al 19 compared the healing time between an arthroplasty group and an arthrodesis group (5.4 ± 5.5 weeks vs 4.0 ± 3.0 weeks, respectively; P = .2). These authors also stated that patients who received preventive surgery healed earlier (P = .004), whereas patients who received surgery for toe infection took longer to heal (P = .002).
Ulcer recurrence frequency
Five studies2,4,7,8,16 reported on ulcer recurrence with a weighted frequency of 4.3% (95% CI = 0.008 to 0.105, I2 = 51.3%). Lew et al 8 reported a significant difference in ulceration recurrence in favor of IP-RA (P = .04).
Ulcer transfer frequency
Only Lew et al 8 reported on ulcer transfer, where it occurred in 15.4% of the patients in the IP-RA group and none in the control group (P = .2).
Postoperative infection
Four studies2,4,7,8 reported on postoperative infection with a weighted frequency of 10.5% (95% CI = 0.038 to 0.198, I2 = 40%). Armstrong et al 2 reported that patients with a history of previous ulceration were significantly more likely to suffer a postoperative infection (P = .04).
Wound dehiscence
Three studies2,7,8 analyzed wound dehiscence with a weighted frequency of 17.8% (95% CI = 0.08 to 0.301, I2 = 0%). Armstrong et al 2 reported no significant difference in the prevalence of postoperative wound dehiscence between the diabetic and nondiabetic groups, and similarly between those with or without diabetic ulceration.
Revision surgery
Four studies2,4,7,8 reported on revision surgeries with a weighted frequency of 5% (95% CI = 0.002 to 0.149, I2 = 63%).
Amputation
Four studies2,4,7,8 reported on the amputation rate following IP-RA with a weighted frequency of 3.4% (95% CI = 0.009 to 0.072, I2 = 0%). Lew et al 8 reported a higher frequency in amputation following standard of care compared with IP-RA (P = .06).
Subgroup analysis
No significant difference was reported between hallucal and lateral toes groups for the healing rate (P = .4) and time to heal (P = .05). Significant differences were found for (1) ulcer recurrence outcome favoring the lateral toes group (P = .02), (2) the postoperative infection outcome (P = .008), and (3) revision surgery outcome (P = .01), both favoring the hallucal group.
Discussion
Patients with DFU are exposed to a dramatic increase in the risk of lower extremity amputation and mortality.3,21,27 In particular, patients with chronic nonhealing ulcers associated with toe deformities were more likely to experience toe amputation because of the high presence of concomitant osteomyelitis. 15 In the last 2 decades, conservative nonamputation surgery gained more attention and advocates in the management of DFUs.6,9,10,20 In line with this, our meta-analysis demonstrated higher efficacy in nearly all outcomes when compared to those reported following standard of care. Healing frequencies following standard of care as reported in the literature were found to be suboptimal, as only around half of the ulcers healed by 20 weeks.6,9,10,20 Although noncomplicated acute ulcers have a higher potential of healing, only 56% of chronic ulcers had shown complete healing by 20 weeks using standard of care. In comparison, most of our included studies comprised chronic ulcers, among which 93.6% healed. 6
The mean healing time of 1 month following IP-RA is considered significantly shorter than that reported with standard of care.1,6,9,10,14,20 This result along with the observed healing rate should motivate clinicians to opt for the surgery earlier and more readily when faced with toe ulcers. A recent evidence-based review calculated the optimal timing for surgical bone offloading to be at 3 months for nonhealing ulcers; 96% of DFUs healed in <1 month after conservative bone surgery, whereas 68% of ulcers healed within 3 months following standard of care. 26
Furthermore, the recurrence rate after this procedure during a mean follow-up of 2 years was very low compared with other conservative nonsurgical treatments. Although healing could reach 90% for noncomplicated DFUs using a total contact cast, the recurrence rate was found to be very high: 40% at 4.5 months 14 and 60% at 3 years. 1
In our review, 2 studies reported successful treatment of postoperative infection with conservative nonsurgical treatment.2,8 Kim et al 7 reported the outcome of revision surgery to treat postoperative infection; 9 (75%) were successful, whereas in 3 (25%) cases amputation was needed to control the infection. Additionally, the amputation frequency is found to be very low; Lew et al 8 reported the comparative outcomes between standard of care and IP-RA with an amputation frequency of 38.4% vs 0%, respectively.
Compared with previously published results following standard of care, conservative surgery has been shown to yield significantly better results and that for nearly every studied outcome. Our results confirm the conclusions of other surgical meta-analyses in the treatment of forefoot DFU.22 -25,28 -30
Only Lew et al 8 reported the ulcer transfer rate. Two newly formed ulcers were noted following IP-RA procedures. Such outcome warrants further investigation in the future with comparative trials.
In most cases, claw toe deformity induced ulcers on the dorsum of the toes, mainly over the proximal interphalangeal joint area. Rarely can it promote ulceration beneath the metatarsal heads or on the pulp area. Three of the included studies reported outcomes on dorsal ulcers associated or not with toe deformities.2,7,19 These dorsal wounds were all located in the lateral toes. On the other hand, studies including plantar ulcers were located on the hallux beneath the area of the IP joint.2,4,7,8,16 Although the period of time from the onset of diabetes to the formation of claw toe is not well investigated, it is admitted that most patients exceed a 10-year duration of diabetes.2,7
The subgroup analysis showed no difference between hallux and lateral toes in terms of healing frequency and time to heal. With respect to complications, ulcer recurrence was significantly lesser in the lateral toes group whereas postoperative infection and revision surgery were significantly lesser in the hallucal group. Nevertheless, many outcome results were yielded from 2 studies and the results should be taken with caution.
Several limitations could be noted. First and foremost, the quality of evidence of any meta-analysis depends on that of the included studies. Most studies were observational, with only 3 studies having a retrospective comparative design, albeit with different comparators. That could be inherent to the difficulty of conducting randomized controlled studies in surgical research. Additionally, the selected studies had a small sample of patients. Owing to the combination of cases noted in some studies, we were not able to differentiate outcomes based on dorsal/plantar, lateral/hallux toe locations, or the presence/absence of infection. Few studies included ulcers located at the tip of the toes but with no comparison with the standard flexor tenotomy procedure. Heterogeneity was mild for 3 outcomes, healing frequency, postoperative infection, and wound dehiscence, and was moderate for ulcer recurrence frequency and revision surgery.
Nevertheless, the pooled results of this meta-analysis are very encouraging and could serve as a solid base for future higher-quality research.
Conclusion
This review of a limited number of cases found that diabetic patients with chronic toe ulcers and deformities may benefit from the interphalangeal resection procedure. The healing frequency and speed of healing for chronic wounds would support the use of this procedure when treating diabetic toe ulcers and deformities. The relatively modest frequency of postoperative complications for this specific condition indicates that this surgery is relatively safe in diabetic patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241256373 – Supplemental material for Interphalangeal Resection Arthroplasty for the Prevention and Treatment of Diabetic Deformities and Ulcers of the Toes: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114241256373 for Interphalangeal Resection Arthroplasty for the Prevention and Treatment of Diabetic Deformities and Ulcers of the Toes: A Systematic Review and Meta-analysis by Kaissar Yammine, Joseph Mouawad, Mohammad Omar Honeine and Chahine Assi in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.