
Abstract
Background:
Overcompression of the distal tibiofibular syndesmosis during open reduction and internal fixation of ankle fracture may affect multidirectional flexibility of the ankle bones.
Methods:
Ten cadaveric lower limbs (78.3±13.0 years, 4 female, 6 male) underwent biomechanical testing in sagittal, coronal, and axial rotation with degrees of motion quantified. The intact force (100%) was the force needed to compress the syndesmosis just beyond the intact position, and overcompression was defined as 150% of the intact force. After intact testing, the anterior inferior tibiofibular ligament (AITFL), interosseus membrane (IOM), and posterior inferior tibiofibular ligament (PITFL) were sectioned and testing was repeated. The IOM and AITFL were reconstructed in sequence and tested at 100% and 150% compression.
Results:
Overcompression of the syndesmosis did not significantly reduce ROM of the ankle bones for any loading modality (P > .05). IOM+AITFL reconstruction restored distal tibiofibular axial rotation to the intact condition. Axial rotation motion was significantly lower with AITFL fixation compared with IOM fixation alone (P < .05). The proximal tibiofibular syndesmosis demonstrated significantly higher motion in axial rotation with all distal reconstruction conditions.
Conclusion:
As assessed by direct visualization, overcompression of the distal tibiofibular syndesmosis did not reduce ROM of the ankle bones. Distal tibiofibular axial rotation was significantly lower with IOM+AITFL fixation compared with IOM augmentation alone. Distal tibiofibular axial rotation did not differ significantly from the intact condition after combined IOM+AITFL fixation. Dynamic fixation of the distal tibiofibular syndesmosis resulted in increased axial rotation at the proximal tibiofibular syndesmosis.
Clinical Relevance:
These biomechanical data suggest that inadvertent overcompression of the distal tibiofibular syndesmosis when fixing ankle fractures does not restrict subsequent ankle bone ROM. The AITFL is an important stabilizer of the distal tibiofibular syndesmosis in external rotation.
Level of Evidence:
controlled laboratory study.
This is a visual representation of the abstract.
Keywords
Introduction
The optimal technique for stabilizing the injured syndesmosis and restoring normal range of motion (ROM) of the tibia, fibula, and talus after open reduction and internal fixation of ankle fractures remains a clinical challenge. Multiple constructs have been described for fixation of the distal tibiofibular syndesmosis, with pros and cons to each method. These constructs include rigid 1- or 2-screw fixation constructs and dynamic suture button fixation constructs.6,10,20,23 Some authors have reported improved resistance to external rotation through the distal syndesmosis after repair, reconstruction, or augmentation of the anterior inferior tibiofibular ligament (AITFL) instead of or in addition to suture button fixation of the IOM.13,14,31,32 However, there is a risk of overcompression of the syndesmosis with all of these fixation constructs.
As a component of reduction, the optimal compressive force to be applied across the syndesmosis during fixation of ankle fractures remains unknown. There is debate as to whether the syndesmosis can be overcompressed and whether overcompression affects ROM of the tibia, fibula, and talus. Previous biomechanical studies have reported that the syndesmosis can be overcompressed, thereby limiting ankle range of motion, particularly in dorsiflexion, 18 whereas others have refuted the possibility of overcompression and subsequent limitations on ROM. 28 More recent biomechanical investigations have demonstrated that syndesmotic overcompression can occur but does not affect ankle ROM.9,21,24 Clinical experience suggests that the syndesmosis can be overtightened and result in loss of dorsiflexion, pain, and/or radiographic evidence of anterior subluxation of the talus.1,7,15 However, the quantitative compressive force needed to accurately reduce but not overtighten the syndesmosis and the effect of overcompression on the multidirectional range of motion of the ankle bones remains poorly defined. Further, direct arthroscopic visualization of the syndesmosis would provide improved ability to evaluate syndesmotic reduction.
Using direct arthroscopic visualization in a cadaveric model of distal syndesmosis injury, the current investigation aimed to quantify the effect of intentional syndesmotic overcompression on the multidirectional flexibility properties of the tibia, fibula, and talus, and the role of multiple syndesmotic fixation constructs of the distal and proximal tibiofibular syndesmosis. We hypothesized that overcompression of the syndesmosis would result in significantly lower ROM of the tibia, fibula, and talus and that reconstruction of the AITFL in addition to the IOM would significantly reduce multidirectional flexibility under external rotation loading compared to fixation of the IOM alone.
Materials and Methods
Specimen Preparation
Ten fresh frozen cadaveric lower extremities were used (6 male, 4 female, average age 78.3 ± 13.0 years, range 60-94 years). The specimens were obtained from the State Anatomy Board, stored at −20 °C, and thawed 24 hours before use. Standard anteroposterior and lateral plain radiographs were obtained to exclude specimens with osseous pathology or abnormality. Bone mineral density (BMD) was measured for each tibia and fibula using a Lunar Prodigy Scanner 8743 (GE Medical Systems).
In preparation for testing, the proximal portion of the tibia was secured using compression screws in a cylindrical tubing foundation. Care was taken to avoid penetration into the proximal tibiofibular joint. Distal fixation was achieved using 2 compression screws placed between the metatarsals to secure the forefoot to the testing platform. Cable ties passed through the calcaneus were used to secure the hindfoot. Seven optoelectronic motion detection markers were placed on the proximal and distal tibia, proximal and distal fibula, talus, proximal cylindrical tubing, and platform base (Figure 1). Markers were fixed to each bone with metal strips that were flexible enough to bend out of the way during subsequent arthroscopic examination but rigid enough to mitigate micromotion or vibration that might affect data capture. Each marker was equipped with 3 noncollinear infrared light-emitting diodes (IREDS) designed for use with an optoelectronic motion measurement system (Optotrak Certus, Northern Digital Inc, Waterloo, Ontario, Canada) (Figure 1). This system allows for tracking of rigid body motion within an accuracy of 0.1 degrees of rotation and resolution of 0.01 degrees. 3

Intact specimen loaded on the 6-degree-of-freedom musculoskeletal simulator.
Multidirectional Flexibility Testing
Three-dimensional multidirectional flexibility testing was performed using a custom 6-degree-of-freedom musculoskeletal simulator configured with the OptoTrak Certus motion analysis system. The apparatus includes 3 independent stepper motors, harmonic drives, and electromagnetic clutches that apply pure unconstrained rotational moments about the x (sagittal), y (axial), and z (coronal) axes. The optoelectronic system combined with aluminum plates containing infrared light emitting diodes (IREDS) markers used in the current study are rigid enough to minimize errors while performing slow rate kinematic analysis.4,5 Observers monitored the test system continuously for change in positioning of system components. A relative angulation accuracy of 0.04 degrees between 2 rigid bodies has been reported with this system, considered to be negligible error in terms of the angulation being measured. 16
To determine multidirectional flexibility, 6 nondestructive pure moment loads were applied as follows: sagittal (±7.5 Nm), coronal (±4 Nm), and axial rotation (±7.5 Nm) at an angular displacement rate of 3 degrees/second. Moment loads were based on physiologic limits of the nonweightbearing ankle and extrapolated pure moment ranges from previous unconstrained cadaveric evaluations. 8 Testing was repeated for 3 loading and unloading cycles. Data from the third cycle was used for analysis to account for the natural viscoelasticity of the soft tissues.
Kinematic multidirectional flexibility testing was used to quantify the angular rotation (degrees) of the proximal tibiofibular, distal tibiofibular, tibiotalar, and talofibular regions. ROM was calculated as the sum of the neutral and elastic zones and defined as the peak total ROM (Euler angle rotation) at the third loading cycle for each testing condition. Absolute motion values (degrees) were quantified for all loading modalities. Translation was not measured.
Ankle Arthroscopy and Syndesmotic Compression
After each specimen was loaded in the simulator, ankle arthroscopy was performed with the ankle at neutral position (Figure 2). Neutral ankle position created the most reproducible and stable specimen configuration in the musculoskeletal simulator and facilitated arthroscopic probing of the syndesmosis. Only the relative differences in motion between bones was recorded. The syndesmosis was measured using spheres ranging in diameter from 2.0 to 8.5 mm and mounted on K-wires. The spheres were used to probe the tibiofibular joint 5 mm posterior to the anterior aspect of the tibiofibular joint. 11 Gentle force was used to pass incrementally larger spheres into the intact joint. The largest-diameter sphere that could be passed beyond its equator into the tibiofibular space was defined as the intact position of the syndesmosis. A C-clamp modified with a force transducer was used to quantify compressive force across the distal tibiofibular syndesmosis (Figure 3). The clamp was placed 5 cm proximal to the ankle joint to provide space for suture button fixation across the syndesmosis. To mitigate rotational malreduction, the medial tine of the clamp was placed at the center point between the anterior and posterior edge of the medial tibia and the lateral tine was centered accordingly on the fibula. To mitigate craniocaudal malalignment, the clamp was applied in a plane parallel to the ankle joint.

Arthroscopic image of an intact specimen undergoing probing of the anterior portion of the syndesmosis with a custom-manufactured sphere mounted on a K-wire.

Specimen undergoing syndesmosis compression. A C-clamp configured with a load cell was used to quantify the compressive force applied across the distal tibiofibular syndesmosis.
The force required to compress the syndesmosis just past the intact position such that the appropriate sphere could not be passed was defined as the intact force (100% compression). Overcompression of the syndesmosis was defined as 1.5× the intact force (150% compression). Compression or overcompression was maintained during the knotting of the sutures with continuous confirmation of the load cell readout (streaming data). A needle driver was used by an assistant to secure the 2 initial knots while the third knot was placed. Further, to ensure that the initial knots remained tight and the applied compression was maintained. All reconstructions were performed by a board-certified orthopaedic foot and ankle surgeon using standard clinical technique.
Treatment Groups
The treatment groups included the intact condition, destabilized, and a series of reconstructions. In the destabilized condition, the AITFL, IOM, and PITFL were transected from the level of the ankle joint extending 5 cm proximally. The proximal tibiofibular joint was left intact, and the deltoid ligament was left intact medially. After destabilization testing, the syndesmosis was sequentially reconstructed and tested with 5 different combinations of compression, IOM fixation, and AITFL fixation: (1) IOM fixation at 100% compression (IOM 100), (2) IOM fixation at 150% compression (IOM 150), (3) IOM and AITFL fixation at 150% compression (IOM+AITFL 150), (4) IOM and AITFL fixation at 100% compression (IOM+AITFL 100), and (5) AITFL fixation alone at 100% compression (AITFL 100). The syndesmosis was reconstructed with the ankle in neutral position for each testing condition.
For the IOM 100 construct, fixation of the IOM was performed with a flexible, custom suture button construct. A 3.5-mm hole was drilled from lateral to medial through the fibula and tibia parallel to the ankle joint, with a starting point on the fibula measured 2 cm proximal to the ankle joint. Using palpation and visual inspection, the drill hole was angled anteriorly toward a center point on the medial tibia face between the anterior and posterior edges of the tibia. The drill hole technique was performed after destabilization to model what is typically performed intraoperatively by the senior author. The modified C-clamp was used to reduce the syndesmosis to 100% compression. Reduction was confirmed by visual inspection of the fibula within the incisura. Clinical and cadaveric studies have demonstrated a lower rate of syndesmosis malreduction when using suture button fixation because the flexibility of the construct allows positioning of the fibula in its natural resting position within the incisura.25,29 The IOM was then fixed with No. 5 FiberWire (Arthrex, Inc, Naples, FL) secured to custom metal buttons on the medial cortex of the distal tibia and lateral cortex of the distal fibula and tightly secured (Figure 4). The buttons were 1 cm in diameter with 2 parallel drill holes for passage of the suture material. The C-clamp was removed and multidirectional flexibility testing was performed.
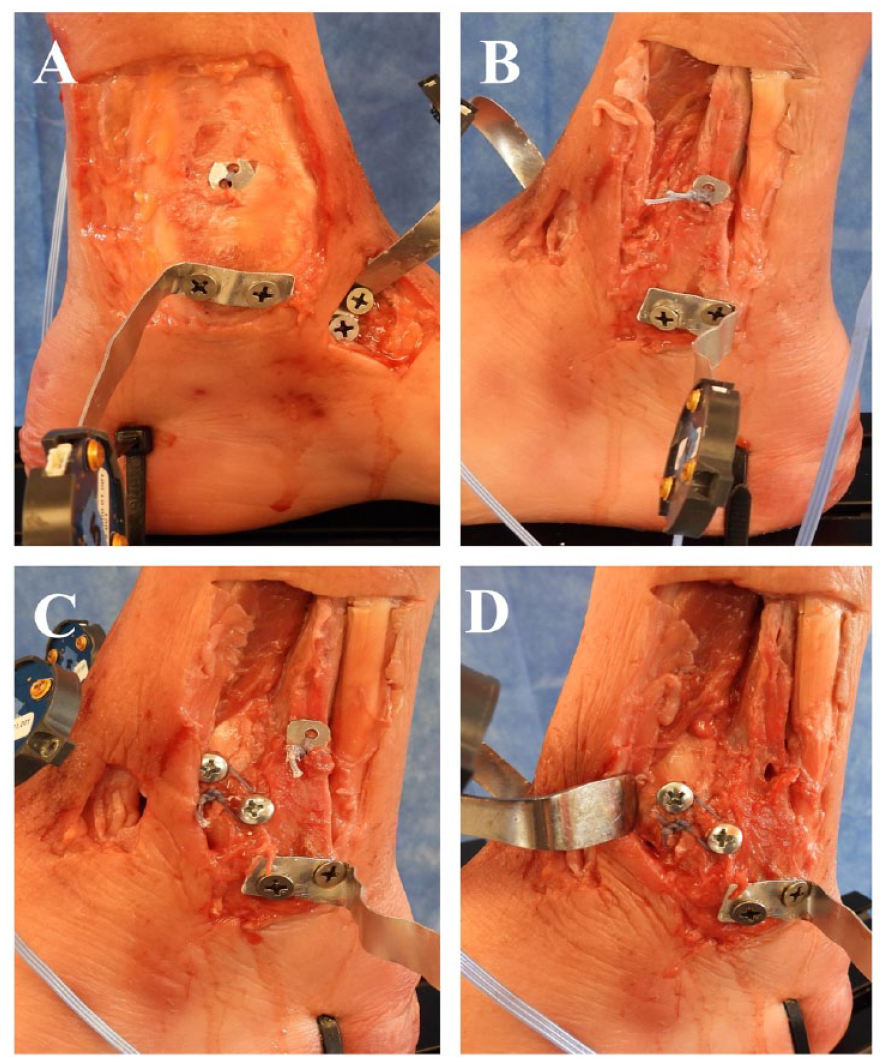
(A) Medial and (B) lateral photographs depicting IOM augmentation using a custom suture button implant directed from the fibula to the tibia and angled 30 degrees anteriorly. Lateral photographs depicting the (C) IOM plus AITFL and (D) AITFL alone conditions. The AITFL reconstruction used a custom suture augmentation directed from the fibula to the tibia in line with the native fibers of the of the AITFL and secured with screws at the ligament footprint in the respective bones.
For the IOM 150 construct, the previous IOM fixation was removed and the syndesmosis was reduced to 150% compression using the modified C-clamp. IOM flexible fixation was performed as described and tightened securely. The C-clamp was removed and multidirectional flexibility testing was repeated. For the IOM+AITFL 150 construct, the previous IOM reconstruction was augmented with a No. 10 one-inch roundhead screw perpendicular to the tibial cortex at the tibial footprint of the AITFL on the anterolateral distal tibia. An identical screw was placed at the AITFL footprint on the anterior distal fibula. A No. 5 FiberWire suture was then wrapped around the screw heads circumferentially and tied securely. The screws were then further tightened to the bone to reinforce the suture fixation (Figure 4), and multidirectional flexibility testing was repeated. For the IOM+AITFL 100 condition, the previous IOM and AITFL fixation devices were removed and the syndesmosis was reduced to 100% compression using the modified C-clamp. The custom flexible IOM and AITFL reconstructions were performed as described above and multidirectional flexibility testing repeated. Finally, for the AITFL alone group at 100%, IOM augmentation was removed and flexibility testing repeated.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics v22 (Armonk, NY, USA). For the 6 motions in 3 planes, ROM was calculated as the sum of the neutral and elastic zones and defined as the peak total ROM (Euler angle rotation) at the third loading cycle. The change in degrees angulation of the tibia, fibula, and talus for each specimen was measured in degrees and expressed in absolute values. A Mauchly test of sphericity was used to assess the assumption of sphericity. A 1-way analysis of variance with repeated measures and Bonferroni post hoc analyses were performed to compare ROM between treatment groups. All data are shown as mean value plus or minus 1 SD, and statistical significance was indicated at P <.05.
Results
Radiography
Plain film radiography indicated no osseous pathology requiring exclusion from the current study. Bone mineral density scans yielded an average of 1.056 ± 0.295 g/cm2 for the tibia and 0.614 ± 0.234 g/cm2 for the fibula.
Compressive Force
The average force needed to compress the syndesmosis without overreduction (intact force, 100% compression) was 71.0 ± 22.2 N.
Multidirectional Flexibility Analysis
The absolute ROM values (mean ± SD) and significant results (P < .05) for all 4 regions of interest (distal tibiofibular, proximal tibiofibular, tibiotalar, and talofibular) of the intact, destabilized, and reconstructed conditions are shown in Table 1.
Range of Motion Data: Absolute Values (Degrees) a .
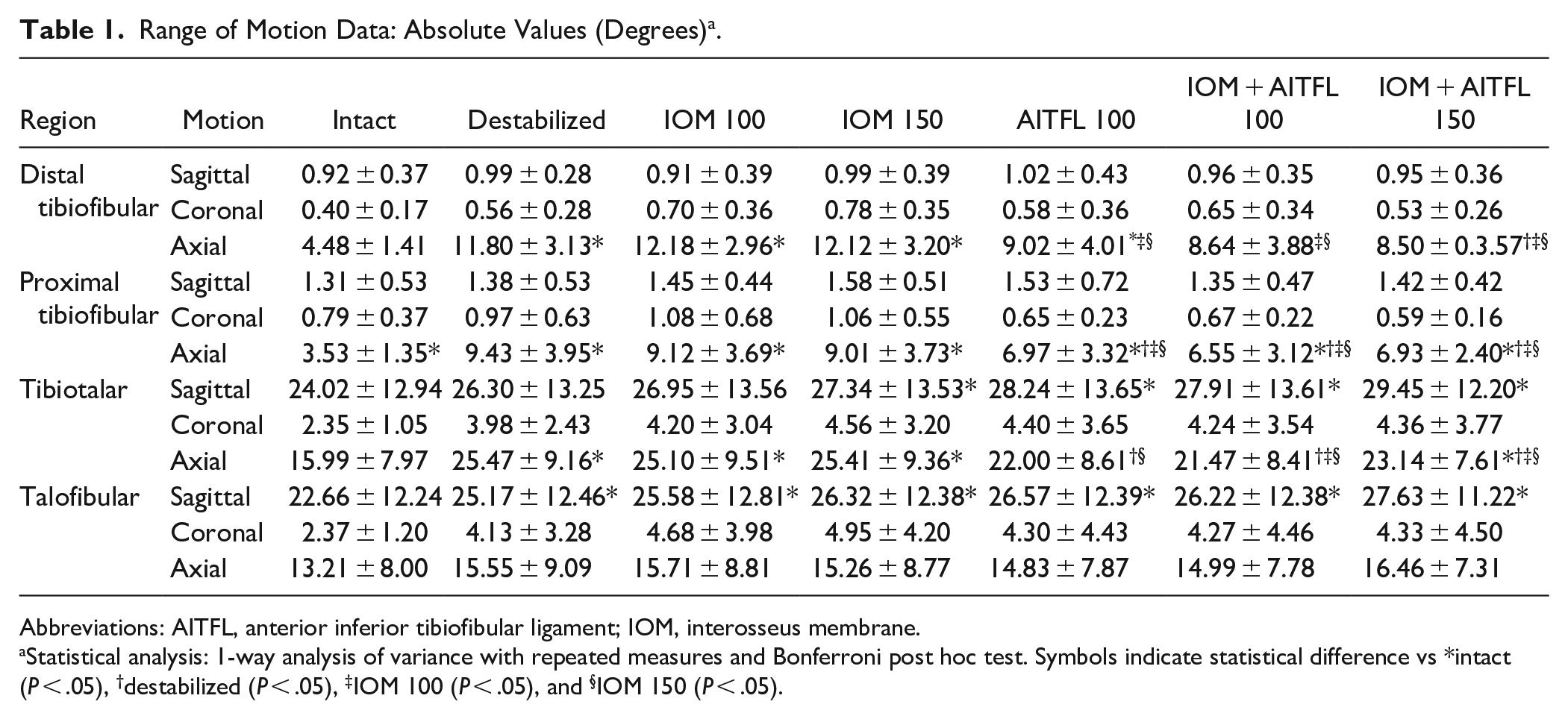
Abbreviations: AITFL, anterior inferior tibiofibular ligament; IOM, interosseus membrane.
Statistical analysis: 1-way analysis of variance with repeated measures and Bonferroni post hoc test. Symbols indicate statistical difference vs *intact (P < .05), †destabilized (P < .05), ‡IOM 100 (P < .05), and §IOM 150 (P < .05).
Distal Tibiofibular Syndesmosis Flexibility
Axial rotation demonstrated the greatest level of intrinsic flexibility, with 4.48 ± 1.41 degrees of intact motion compared with 0.92 ± 0.37 degrees in sagittal rotation and 0.40 ± 0.17 degrees in coronal rotation. Following destabilization, the IOM + AITFL 150 group exhibited the greatest reduction in motion in axial rotation, with statistically significant decreases compared to the destabilized (P = .020), IOM 100 (P = .003), and IOM 150 groups (P = .001). No statistically significant differences were observed between constructs in sagittal or coronal loading modes (P > .05) (Figure 5A).
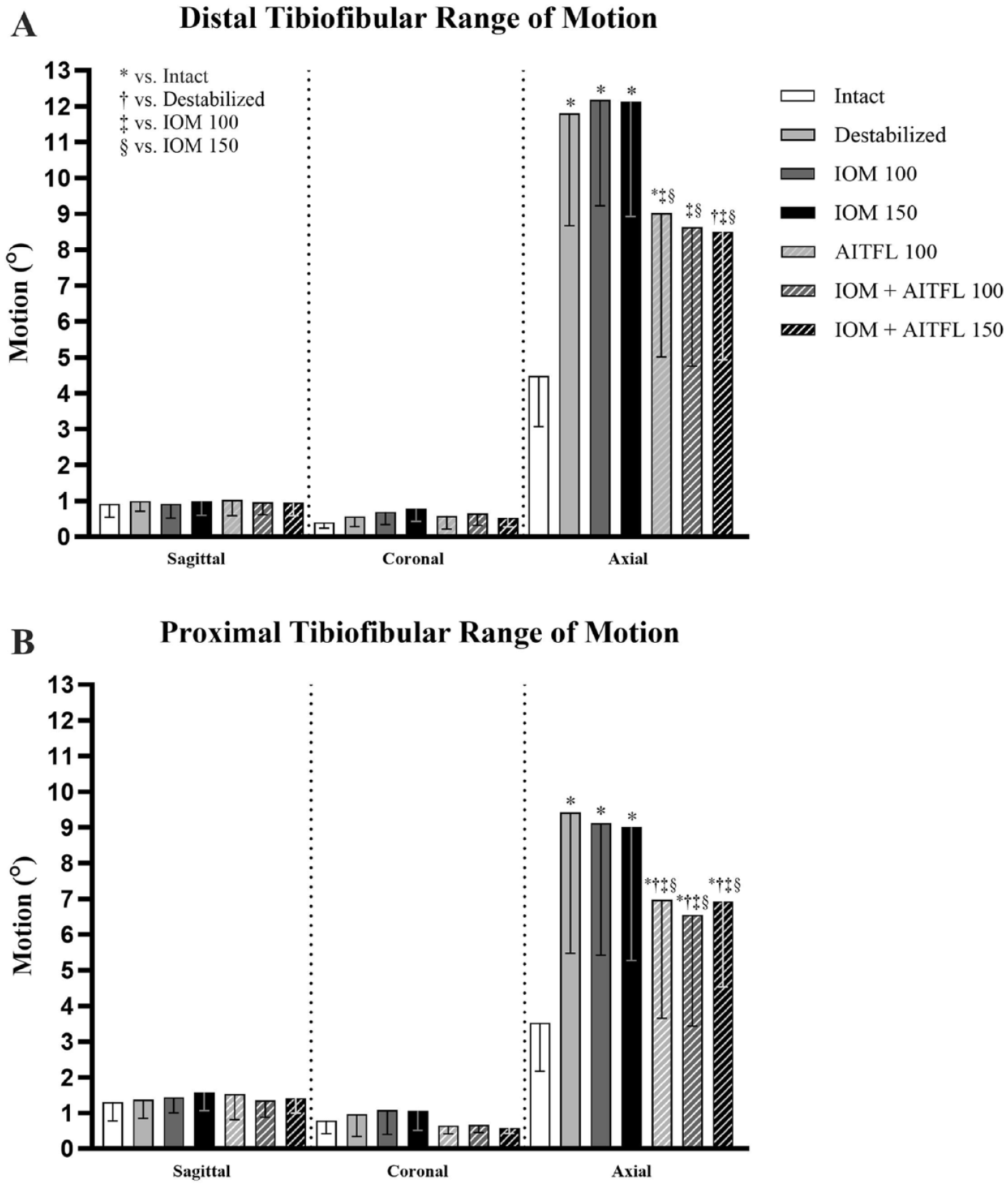
(A) Distal and (B) proximal tibiofibular range of motion in sagittal, coronal, and axial rotation. Bar height represents mean values (°) and error bars minus 1 SD. Symbols indicate statistical difference vs *intact, †destabilized, ‡IOM 100, and §IOM 150. Significance is indicated at P < .05.
Proximal Tibiofibular Syndesmosis Flexibility
Motion trends for the intact proximal tibiofibular region were similar to those for the intact distal tibiofibular region, with 3.53 ± 1.35 degrees of axial rotation compared to 1.31 ± 0.53 degrees in sagittal plane and 0.79 ± 0.37 degrees in coronal rotation. Axial rotation in the destabilized group and all reconstruction groups was significantly higher than in the intact condition (P < .05). All three AITFL reconstruction groups had significantly lower axial rotation compared to the destabilized, IOM 100, and IOM 150 groups (P < .05). No statistically significant differences were observed between constructs in sagittal or coronal loading modes (P > .05). (Figure 5B).
Tibiotalar Flexibility
The mean intact motion at the tibiotalar junction was 24.02 ± 12.94 degrees in sagittal, 2.35 ± 1.05 degrees in coronal, and 15.99 ± 7.97 degrees in axial rotation. Significantly higher sagittal motion was observed for the IOM 150, AITFL 100, IOM + AITFL 100, and IOM + AITFL 150 groups compared to the intact group (P < .05). In axial rotation, the AITFL 100, IOM + AITFL 100, and IOM + AITFL 150 groups had significantly lower syndesmosis motion compared with the destabilized group (P < .05). No statistically significant differences were observed in coronal rotation (Figure 6).

Tibiotalar range of motion in sagittal, coronal, and axial rotation. Bar height represents mean values (degrees) and error bars minus 1 SD. Symbols indicate statistical difference vs *intact, †destabilized, ‡IOM 100, and §IOM 150. Significance is indicated at P < .05.
Talofibular Flexibility
The mean intact motion at the talofibular junction was 22.66 ± 12.24 degrees in sagittal, 2.37 ± 1.20 degrees in coronal, and 13.21 ± 8.00 degrees in axial rotation. Significantly higher sagittal rotation was observed for all groups compared to the intact condition (P < .05). No statistically significant differences were observed in coronal or axial rotation (Figure 7).

Talofibular range of motion in sagittal, coronal, and axial rotation. Bar height represents mean values (°) and error bars minus 1 SD. *Statistical difference vs intact. Significance is indicated at P < .05.
Discussion
As has been previously reported, overcompression of the distal tibiofibular syndesmosis did not result in significantly lower multidirectional ROM of the tibia, fibula, or talus compared to the intact condition. As expected, tibiofibular axial rotation was significantly lower with combined AITFL and IOM fixation compared to IOM fixation alone. The novel finding of significant change in axial rotation at the proximal tibiofibular syndesmosis suggests a dimension of change with tibiofibular destabilization and syndesmosis compression that warrants further study for potential clinical implications.
Using direct arthroscopic visualization as opposed to radiographic criteria, the current study supports the findings of previous studies on syndesmosis reduction force. In a biomechanical study assessing the effects of varying tension on a suture button construct in fixation of the distal tibiofibular syndesmosis using static loads in a custom frame, the authors found that 8 to 12 kg of tension provided the greatest stability at the distal tibiofibular articulation, but also tended to overcompress the syndesmosis on stress computed tomography. 17 In another biomechanical study that also used computed tomography to assess syndesmosis reduction, a clamp with load cell was used to apply various loads across the distal tibiofibular syndesmosis. 22 The syndesmosis was then fixed statically with a screw. The authors identified 100 N as the optimal force needed to achieve reduction, and overcompression (medialization of the fibular) was identified with forces of 140 and 160 N. The forces required to reduce the syndesmosis in those studies were in the same range as the intact force identified in the current study.
The current study results are similar to those of a cadaveric study that found no effect on ankle dorsiflexion with foot plantarflexion and maximal compression of the syndesmosis. 28 The previous investigation differed from the current study in that rigid screw fixation was implanted vs dynamic suture fixation. Schon et al 24 observed radiographic overcompression of the syndesmosis when the syndesmosis was reduced with a clamp and reconstructed with a suture button device. Overcompression occurred in foot plantarflexion, foot neutral position, and foot dorsiflexion, but did not affect subsequent ankle ROM. In the current study, the syndesmosis was fixed with the ankle at neutral position as opposed to plantarflexion or variable positioning.9,19,24 Nonetheless, the findings of the current investigation corroborate these previous studies and suggest that ankle position at the time of syndesmosis fixation has no effect on syndesmotic overcompression or subsequent ROM. The current study and previous reports conflict with clinical observations of postoperative pain, loss of ankle dorsiflexion, and anterior subluxation of the talus with syndesmotic overcompression.7,15
The current data also corroborate the importance of the AITFL in stabilizing the distal tibiofibular syndesmosis when external rotation force is applied and suggest that isolated suture button fixation of the IOM may not provide sufficient biomechanical stability. A cadaveric study identified the AITFL as the primary restraint to external rotation force. 2 Repairing and augmenting the AITFL with suture tape restored rotational kinematics and stability of the ankle joint in an isolated syndesmosis injury model. 13 Other biomechanical studies have reported that adding AITFL augmentation to a transfibular suture button construct improved stabilization of the syndesmosis against external rotation force compared with isolated suture button fixation of the IOM.26,30 Repairing or augmenting the AITFL alone or in combination with suture button fixation of the IOM has also been reported clinically with good functional outcomes and fewer complications than screw fixation of the syndesmosis.14,31,32
Compared to the intact condition, significantly higher axial rotation was observed at the proximal tibiofibular syndesmosis for the destabilized group and all reconstruction groups. Data on proximal tibiofibular ROM after ankle injury are still taking shape. A cadaveric syndesmosis injury 3D-motion study assessed relative motion of the fibula and tibia in the intact condition, after sectioning of the syndesmotic ligaments, and after various screw configurations to fix the syndesmosis. 12 The authors noted that proximal fibula motion was less than and more variable than distal fibula motion. The fibula head rotated internally with foot plantarflexion and externally with foot dorsiflexion. The magnitude of increased proximal syndesmotic motion identified at the proximal tibiofibular joint in the current study was greater than previously reported.12,27 Direct comparisons are limited because the current study used different motion analysis techniques and dynamic fixation constructs vs rigid screw fixation. However, although the clinical relevance of these findings is not known, the current results suggest that there may be increased stress at the proximal tibiofibular joint after dynamic fixation of distal syndesmotic injuries.
This study has limitations. Cadaveric tissue is an imperfect representation of living tissue and does not account for healing. Physiologic weightbearing load was not applied to the ankle joint during testing. Fixation constructs in this study were approximations of the type of dynamic fixation constructs used clinically and may not have the same biomechanical characteristics. For stability purposes, the deltoid ligament was not sectioned, which could have affected the relative ROM of the ankle bones after disruption of the syndesmosis. A rigid fixation construct (screws) was not created and might have provided a useful comparison to the biomechanical properties of dynamic fixation constructs. Although attempts were made to standardize clamp placement across specimens, minor variations in the clamp position between specimens and plastic deformation of the fibula during clamping might have affected the applied forces and reduction of the syndesmosis. To model the intraoperative condition, the drill hole for IOM fixation was performed after destabilization and by using visual inspection and palpation as opposed to a vector guide or radiography. This technique may have led to variation in drill hole location across specimens and increased the risk for syndesmotic malreduction. Parts of the fixation constructs were reused for 2 of the testing conditions (IOM + AITFL 150% and AITFL 100%), which could have resulted in loosening of the fixation after the initial round of testing. This study cannot establish whether the lack of statistical difference in tibiofibular axial plane rotation between combined AITFL and IOM fixation and the intact condition is clinically relevant. Moment loads were extrapolated from calculations in spine research because, to our knowledge, unconstrained moment loading in the foot and ankle has not been reported. Because of testing system constraints, only angular rotation and not translation was quantified.
In conclusion, as assessed by direct visualization, overcompression of the distal tibiofibular syndesmosis did not reduce ROM of the ankle bones. Distal tibiofibular axial rotation was significantly lower with IOM+AITFL fixation compared with IOM augmentation alone. Distal tibiofibular axial rotation did not differ significantly from the intact condition after combined IOM+AITFL fixation. Dynamic fixation of the distal tibiofibular syndesmosis resulted in increased axial rotation at the proximal tibiofibular syndesmosis.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241255356 – Supplemental material for Effect of Distal Tibiofibular Destabilization and Syndesmosis Compression on the Flexibility Kinematics of the Ankle Bones: An In Vitro Human Cadaveric Model
Supplemental material, sj-pdf-1-fao-10.1177_24730114241255356 for Effect of Distal Tibiofibular Destabilization and Syndesmosis Compression on the Flexibility Kinematics of the Ankle Bones: An In Vitro Human Cadaveric Model by Walter C. Hembree, Daina M. Brooks, Byron Rosenthal, Carlynn Winters, Jordan B. Pasternack and Bryan W. Cunningham in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
We thank Lyn Camire Jones, MA, ELS, of our department for editorial support.
Ethical Approval
Ethical approval was not sought for the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.