
Abstract

Introduction
Charcot neuroarthropathy, a condition often observed in patients with diabetes, is a destructive joint disorder characterized by joint dislocation, fractures, and severe deformities. 3 Typically, it progresses from the inflammatory phase, where joint destruction occurs, to the coalescence phase, and eventually reaches the consolidation phase. 3 Performing surgery during the early stages of neuroarthropathy is challenging because of the swelling, inflammatory process, and osteopenia leading to difficulty in reduction and fixation, and there is a high risk of continued joint destruction postoperatively. Additionally, complications such as metal failure and chronic intractable ulcers can occur at any stage, and in the worst-case scenario, amputation may be needed. 9 Therefore, in some cases, conservative treatment methods, such as a total contact cast, may be more advantageous while attempting to distribute weight as evenly as possible and waiting for consolidation to occur. 5
We report a patient with Charcot neuroarthropathy in the hindfoot treated using a conservative approach who achieved autofusion after 3 years, leading to a successful clinical outcome. This study was approved by the Institutional Review Board of our institution, and verbal consent was obtained from the patient, which was subsequently documented in electronic medical records.
Case Report
A 56-year-old man presented to an outpatient clinic with the chief complaint of a swollen and deformed right ankle. He reported that his ankle area had been swollen for approximately 1½ years, and the swelling had worsened over the past month after he started increasing his physical activity. His underlying medical condition included a 7-year history of diabetes mellitus for which he was taking oral diabetic medications.
On physical examination, the patient weighed 80 kg and his body mass index was 30.5. There was mild to moderate swelling and warmth in the right ankle area. The distal third of the lower leg extending to the ankle joint was generally erythematous, but the dependent rubor disappeared after elevating the leg for a few minutes. Signs of skin atrophy were not observed. Grossly, the forefoot was neither abducted nor adducted, and the hindfoot was assessed to be in neutral alignment. In addition, no areas appeared to receive eccentric pressure due to protruding bony prominences in the plantar side of the foot. His ankle joint range of motion was slightly reduced, and there was triceps tightness present. Sensation was found to be decreased during the 2-point discrimination test. Laboratory tests were conducted to rule out the possibility of acute infection. The results showed a white blood cell count of 8000/μL and C-reactive protein level of 0.47 mg/dL. His HbA1c level was 8.4%.
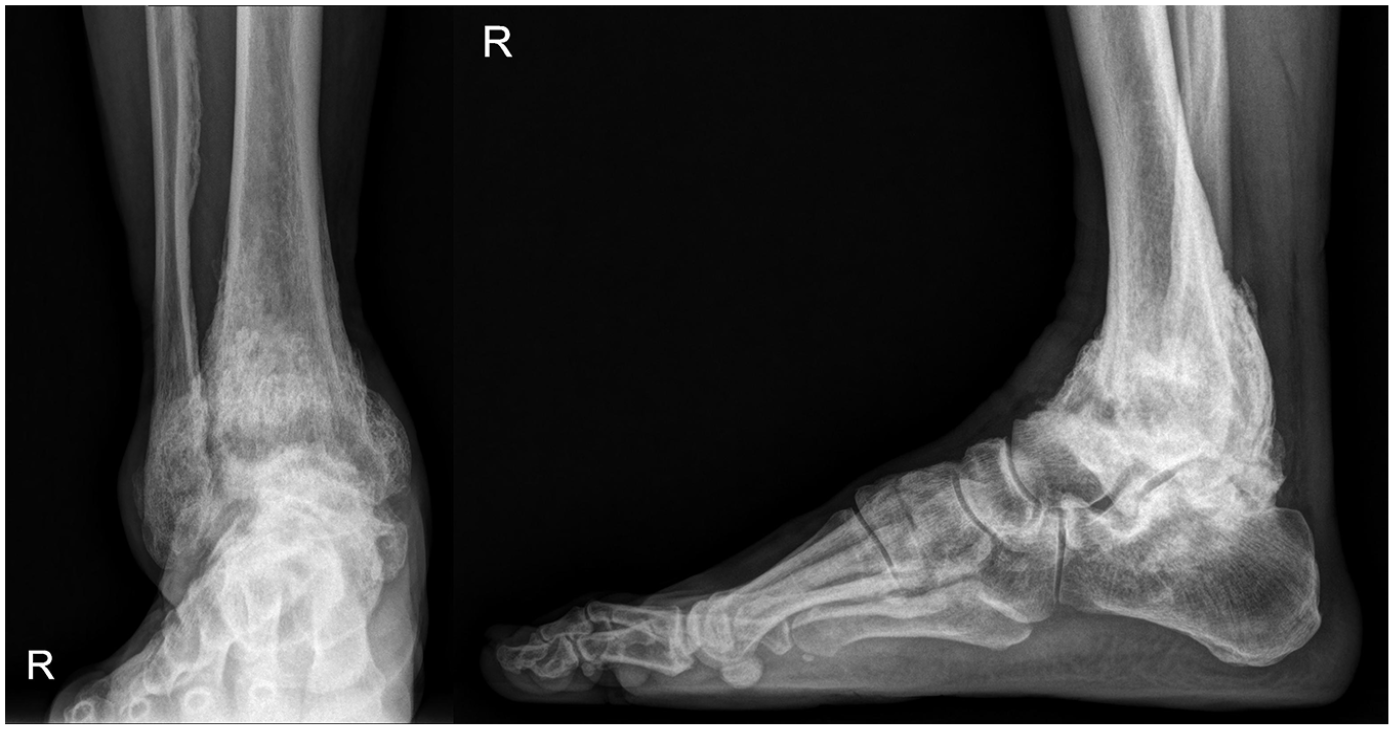
Plain radiographs revealed severe destruction of the ankle joint, sclerotic changes, and a solid periosteal reaction (Figure 1). Computed tomography of the 3-dimensional structure revealed extensive osteolysis on the medial side, mixed with sclerotic changes and severe joint destruction (Figure 2). Magnetic resonance imaging revealed bone edema, which was consistent with those of neuroarthropathy (Figure 3).

Initial plain standing ankle radiographs demonstrating severe destruction of the ankle joint, sclerotic changes, and a solid periosteal reaction.

Initial weightbearing computed tomography images showing extensive osteolysis on the medial side, mixed with sclerotic changes and severe joint destruction.

Initial magnetic resonance images revealing bone edema, which is consistent with neuroarthropathy.
With regard to clinical outcome scores, the patient's Foot and Ankle Outcome Score (FAOS) was 55.2 points (FAOS symptoms: 81; FAOS pain: 25; FAOS activities of daily living: 50; FAOS sports and recreation: 85; and FAOS quality of life: 35). The patient was diagnosed as Charcot neuroarthropathy based on the underlying condition of diabetes mellitus, the physical examination, and the destruction of the ankle joint being present but with disproportionately less pain. To prevent further deterioration, he was advised to wear a short leg thermoplastic splint (New Yogips, Woosam Medical, Seoul, Republic of Korea) with an ankle protector with BOA (DR A-080, A-mi Global, Republic of Korea) indoors and a boot cast (Rebound air walker; Össur Americas, Irvine, CA) outdoors, ensuring that they were always worn (Figure 4). A short leg thermoplastic splint was molded to fit the patient’s ankle, providing rigidity at the posterior side, while an ankle protector with BOA was used in conjunction to serve as an anterior shell. He was also advised to maintain nonweightbearing positions as much as possible, with only toe-touch weightbearing allowed. We decided to consider ankle arthrodesis once consolidation occurred and his condition stabilized.

(A) A boot cast (Rebound air walker; Össur Americas), a short leg thermoplastic splint (New Yogips; Woosam Medical), and an ankle protector with BOA (DR A-080, A-mi Global, Republic of Korea) (left to right), (B) Example photo of wearing a short leg thermoplastic splint and an ankle protector with BOA.
At the 8-month follow-up, the patient reported being able to walk plantigrade without significant difficulty while wearing an orthotic device. His foot was considered shoeable. However, he felt uncomfortable walking without the device and mentioned that the swelling had waxed and waned. Simple radiographic findings showed no significant lesion progression (Figure 5); however, we decided to adopt a wait-and-see approach.

Plain standing ankle radiographs at the 8-month follow-up.
At the 2-year follow-up, the patient reported that swelling had significantly reduced and walking had become more comfortable. He mentioned that he attempted to run as his ability to walk improved; however, he felt discomfort while running but found it manageable to wear an ankle protector with BOA instead of the previously used boot cast. Nevertheless, he was advised to prohibit activities that involve heavy weightbearing, such as running. There was no additional occurrence of deformity, nor were there any newly developed ulcers. Radiographically, the patient’s condition had stabilized (Figure 6); therefore, ankle fusion surgery was considered. However, owing to the patient’s reluctance, regular follow-ups were decided.

Plain standing ankle radiographs at the 2-year follow-up.
At the 3-year follow-up, the patient reported being almost pain-free in the ankle itself, but experienced some tingling sensations in the dorsum of the foot and toes. He demonstrated a stable gait and was satisfied with the outcome. Plain radiographs revealed autofusion of the ankle joint and significant reduction in the swelling of the soft tissue contour (Figure 7). The FAOS was 66.8 points (FAOS symptoms: 97; FAOS pain: 38; FAOS activities of daily living: 64; FAOS sports and recreation: 90; and FAOS quality of life: 45). Therefore, as there has been no significant clinical deterioration during the follow-up period of 3 years and imaging studies showed fusion of the bone, we decided to continue conservative treatment without surgical intervention and planned for regular outpatient follow-up. Additionally, the patient was advised to strictly manage his blood sugar levels.
Plain standing ankle radiographs at the 3-year follow-up revealed autofusion of the ankle joint. There is a noticeable reduction in the swelling of the soft tissue contour from the initial visit to the last follow-up.
Discussion
In neuroarthropathy, although surgical treatment is challenging, it is an important treatment option for the condition. The primary goal is not to create a normal foot but to achieve a foot that can be fitted with an orthotic device and bear weight in a plantigrade position. 3 Surgical treatment options vary; however, in cases where the hindfoot is affected by severe deformity and the ankle is unstable, the only alternative to amputation is fusion surgery to stabilize the joint. Some authors suggested early intervention, such as tibiocalcaneal arthrodesis, in the early stages of the disease when pressure ulcers over bony prominences had not yet developed. 2 However, in most cases, it is essential to delay joint fusion surgery until the end of the consolidation phase (Eichenholtz stage 3). 6 Although fusion surgery is a useful treatment method, complications such as infection, nonunion, malpositioning of hardware, and recurrent ulcers have been reported. 9 Additionally, in cases of unstable fibrous fusion or uncontrollable infection, amputation remains the only treatment option.
Therefore, although surgery remains pivotal for numerous patients, some patients might benefit substantially from conservative management. 8 In cases like ours, where there are no fixed deformities caused by bony prominences, no ulcers, acceptable coronal alignment, and the ability to maintain a plantigrade foot, it may be feasible to continue with conservative treatment without surgical intervention. Sinacore also noted that time to healing is delayed using the total contact cast when a major fixed deformity of the foot is present. 7
The initial treatment involved the use of a boot cast followed by an ankle protector with BOA for stabilization as the condition improved. Although the total contact cast is considered the gold standard, its requirement for multiple visits for replacements not only makes it cumbersome but also introduces additional costs for the patient. Furthermore, the inability to wash the leg and the fact that the cast does not expand if the leg swells can cause discomfort, potentially exacerbating the patient's discomfort. According to previous literature, the removable cast walker has also been effective in reducing plantar foot pressures and treating diabetic foot ulcers. 1 The boot cast used in our case is constructed with thicker foam, starting from the plantar regions and extending to the entire calf area, and a rocker-bottomed outsole. Although the outer part of the boot cast is solid and durable, the characteristics of the rocker bottom help promote the redistribution of the load. Furthermore, an ankle protector with BOA, serving as an anterior shell, may have played a role in stopping the progression moment of the tibia over the foot.
According to a previous study, successful outcomes have been reported without radiographic deterioration even when tolerable weightbearing was maintained during the conservative treatment process. 4 The patient in this case was active and needed to work, making it impossible to maintain 24-hour nonweightbearing positions. Therefore, initially, only toe-touch was allowed, and later, the degree of weightbearing was flexibly adjusted. However, despite being removable, the orthosis must be worn continuously, making patient compliance extremely important.
At the 3-year follow-up, our patient demonstrated successful autofusion, avoiding the potential complications of fusion surgery. To our knowledge, there has been no previous documentation of a similar case with autofusion. Along with the use of orthosis, some previous studies reported the potential for pharmacologic therapies, including bisphosphonates and intranasal calcitonin, for restoring the balance between bone formation and resorption. 10 However, because of the weak quality of evidence, it was not used in this case. Although there was a slight increase in the pain score within the domains of the FAOS, it is not the most significant aspect of Charcot neuroarthropathy. Because he obtained a stable foot and ankle with minimal deformities and no recurrent ulcers, it can be considered that a favorable clinical outcome was achieved.
Conclusion
This case highlights the potential for nonsurgical management of a Charcot ankle without definite coronal plane deformity to an autofused state in 3 years through the use of orthosis and tolerable weightbearing.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241242782 – Supplemental material for Conservative Management Leading to Autofusion in Charcot Ankle: A Case Report
Supplemental material, sj-pdf-1-fao-10.1177_24730114241242782 for Conservative Management Leading to Autofusion in Charcot Ankle: A Case Report by Min Gyu Kyung and Dong Yeon Lee in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study was approved by Seoul National University Hospital Institutional Review Board (IRB No. H-1806-151-953). This study was carried out in accordance with the World Medical Association Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2016R1D1A1B02009379).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.