
Abstract
Background:
Joint replacement procedures have traditionally been performed in an inpatient setting to minimize complication rates. There is growing evidence that total ankle arthroplasty (TAA) can safely be performed as an outpatient procedure, with the potential benefits of decreased health care expenses and improved patient satisfaction. Prior studies have not reliably made a distinction between outpatient TAA defined as length of stay <1 day and same-day discharge. The purpose of our study was to compare a large volume of same-day discharge and inpatient TAA for safety and efficacy.
Methods:
Patients undergoing TAA at our US-based institution are part of an institutional review board–approved registry. We queried the registry for TAA performed by the single highest-volume surgeon at our institution between May 2020 and March 2022. Same-day discharge TAA was defined as discharge on the day of the procedure. Patient demographics, baseline clinical variables, concomitant procedures, postoperative complications, and patient-reported outcomes were collected. Postoperative outcomes were compared after 1:1 nearest-neighbor matching by age, sex, Charlson Comorbidity Index (CCI), and American Society of Anesthesiologists (ASA) score. Multivariable models were created for comparison with the matched cohort outcome comparison analysis.
Results:
Our same-day discharge group was younger (median 58 vs 67 years; P < .001), with proportionally fewer females (36.4% vs 51.4%; P = .044) and lower Charlson Comorbidity Indices (median 1 vs 3; P < .001) than the inpatient group. At a median follow-up of 1 year, after matching by age, sex, CCI, and ASA score, there was no difference in complications (P = .788), reoperations (P = .999), revisions (P = .118), or Patient-Reported Outcomes Measurement Information System (PROMIS) scores between the 2 groups. Multivariable analyses performed demonstrated no evidence of association between undergoing same-day discharge TAA vs inpatient TAA and reoperation, revision, complication, or 1-year PROMIS scores (P > .05).
Conclusion:
In our system of health care, with appropriate patient selection, same-day discharge following TAA can be a safe alternative to inpatient TAA.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Total ankle arthroplasty (TAA), a mainstay of treatment for end-stage arthritis, has traditionally been performed in an inpatient setting to minimize complication risks and adequately treat postoperative pain. 8 In various joint replacement procedures, there has been an effort to decrease health care expenses and improve patient satisfaction by transitioning to outpatient and short-stay procedures.1,13,24,26 In part likely due to Medicare policies, TAA has lagged behind other joint replacements in the transition to the outpatient setting. 1
There is growing evidence that TAA can safely be performed as a short-stay or outpatient procedure, with similar rates of complications, adequate postoperative pain control, and adequate patient satisfaction.1,8,15,21,22,28 Functional outcomes have also been shown to be similar for outpatient TAA. 1 However, many studies have defined outpatient TAA as length of stay <1 day or similar.1,22 Failing to distinguish between same-day discharge from the recovery room and overnight stay neglects a set of clinical and financial ramifications posed by same-day discharge. Prior studies of same-day discharge have been limited by small sample sizes and/or lack of comparative inpatient groups.5,8,18,21
Given the lack of data on outcomes following outpatient TAA with same-day discharge, there is a need for larger comparative studies. If these studies were to demonstrate equivalent outcomes and reduced costs, this would indicate that more TAA can safely be performed in ambulatory surgery centers. The primary aim of our study was to compare outcomes between same-day discharge and inpatient stays among a large cohort of patients who underwent a TAA at our institution. We also aimed to compare baseline characteristics and operative variables between the 2 groups. We hypothesized that, with appropriate patient selection, same-day discharge TAA would have equivalent outcomes as compared to inpatient TAA.
Methods
Patient Selection
This study was a retrospective review of data collected prospectively as part of the IRB-approved Total Ankle Replacement Registry at our US-based institution. All patients who underwent a primary TAA by the single highest volume surgeon (C.D.) between May 1, 2020, and February 28, 2022, were included. All TAAs were performed in a hospital setting. Same-day discharge was defined as discharge on the same day as the procedure. Demographic variables, preoperative clinical characteristics, operative variables, and complications were extracted from the registry and compared between outpatients and inpatients.
At our institution, decision for same-day discharge is made on a case-by-case basis by the treating surgeon and patient. Patient characteristics such as age, body mass index (BMI), underlying medical conditions, and pain management plans are assessed. Logistical factors such as geographic distance from home to hospital and timing of surgery are evaluated. The benefits of same-day discharge and inpatient admission are discussed with the patient as well as the need for good social support at home. Ultimately, these various considerations are explored in a shared decision-making process, and a final choice for same-day discharge is made.
Demographic variables included age, sex, and insurance type. Preoperative clinical characteristics included primary indication for surgery, past surgical history, BMI, smoking history, alcohol abuse history, baseline Patient-Reported Outcomes Measurement Information System (PROMIS) scores, Charlson Comorbidity Index (CCI), American Society of Anesthesiologists (ASA) score, and individual comorbidities including congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, diabetes, and bleeding disorders. Operative variables included procedure start and end time, tourniquet time, implant used, and concomitant procedures. Included implants were Vantage Total Ankle (Exactech, Gainesville, FL) and INBONE II Total Ankle System (Wright Medical Technology, Arlington, TN). Postoperative outcomes included discharge time, rates of overall and individual complications, reoperations, and revision surgeries, and PROMIS scores at 1 year.
Statistical Analysis
Descriptive statistics were performed for baseline patient characteristics, operative variables, and postoperative outcomes. Differences between cohorts were assessed using Mann Whitney U test for continuous variables and Pearson chi-square or Fisher exact test for categorical variables.
To assess if there was evidence for differences in postoperative outcomes between same-day discharge TAA and inpatient TAA after controlling for baseline characteristics, 1:1 nearest neighbor matching without replacement using the Mahalanobis distance was used to approximate a blocked clinical design. 12 Specifically, a caliper with ±5 age years, ±3 CCI, and ±1 ASA score was used in the matching criteria to account for confounding. The target estimand was average treatment effect on the treated, which was defined as the same-day discharge TAA cohort. After matching, differences in categorical outcomes such as reoperation, revision, and complication were tested using Fisher exact test, whereas continuous outcomes such as PROMIS scores were evaluated using the Mann Whitney U test. Complications were recorded from time of discharge to a median follow-up of 1 year.
Furthermore, we conducted a series of logistic and linear regression models using the entire cohort of all patients to investigate if there was evidence of association between having same-day discharge surgery and reoperation, revision, complication, and PROMIS domains at 1 year, respectively, after adjusting for demographic characteristics and baseline PROMIS scores. We then assessed if the entire cohort multivariable models reached similar conclusions to the matched cohort outcome comparison analysis.
Statistical significance was established at α = 0.05. Analysis was conducted on R: A Language and Environment for Statistical Computing using the rms and MatchIt packages.
Results
Preoperative Variables
Our unmatched cohort included 70 same-day discharge patients and 118 inpatients who underwent TAA between May 2020 and March 2022. The same-day discharge TAA group was younger (median 58 vs 67 years; P < .001) with proportionally fewer females (36.4% vs 51.4%; P = .044) than the inpatient group.
Patients who underwent same-day discharge TAA had fewer comorbidities as measured by Charlson Comorbidity Index (CCI) (median 1 vs 3; P < .001) (Table 1), and the distribution of the 2 groups by ASA Score was different (P = .012). This was reflected in a lower proportion of same-day discharge patients with obstructive sleep apnea (7.1% vs 28.0%; P = .001). There was no evidence of differences in other individual medical comorbidities, including congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, diabetes, and bleeding disorders (Table 1). There was no evidence of differences in BMI, smoking history, or alcohol abuse between the 2 groups.
Preoperative Patient Characteristics a

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson Comorbidity Index; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; EtOH, ethanol; ORIF, open reduction internal fixation; OSA, obstructive sleep apnea; TAA, total ankle arthroplasty.
Unless otherwise indicated values are n (%). Bold text indicates statistical significance, P < .05.
Continuous variables reported as median [IQR].
Same-day discharge patients and inpatients had a different distribution of arthritis etiology (P = .006), with more same-day discharge patients undergoing TAA for instability (25.7% vs 11.9%) and fewer same-day discharge patients undergoing TAA for other indications including inflammatory arthritis, flatfoot deformity, or takedown of ankle fusion (10.0% vs 22.9%) (Table 1). There was no evidence of differences in surgical history between the 2 groups.
Operative Variables
The median procedure start (11:05 vs 13:02, P = .002) and end times (13:02 vs 15:32, P < .001) were approximately 2 hours earlier in the same-day discharge vs the inpatient group, but there was no evidence of difference in tourniquet times between groups (120.4 vs 121.3 minutes, P = .849), or in procedure length (150.0 vs 151.0 minutes, P = .865). There was a difference in the distribution of implants used for same-day discharge TAA vs inpatient TAA (P = .030): there were more low-profile implants in the same-day discharge group (68.6% vs 50.8%) and more stemmed modular implants in the inpatient group (31.4% vs 46.6%).
Concomitant procedures are outlined in Table 2. The most common procedures were Achilles lengthening (n = 112, 59.6%) and medial malleolus fixation (n = 83, 44.1%). Fewer same-day discharge patients underwent procedures to address progressive collapsing foot deformity like medializing calcaneal osteotomy (4.29% vs 17.8%; P = .007) and Cotton osteotomy (1.43% vs 10.2%; P = .033). There was no evidence of differences in other concomitant procedures between the 2 groups (Table 2). The median length of stay was 3.0 hours for same-day discharge TAA vs 24.4 hours for inpatient TAA. The median discharge time for same-day discharge TAA was 16:29 vs 14:04 for inpatient TAA.
Operative Variables. a

Abbreviations: MCO, medializing calcaneal osteotomy; MMF, medial malleolus fixation; ROH, removal of hardware; TMT, tarsometatarsal.
Unless otherwise noted, values are n (%). Bold text indicates statistical significance, P < .05.
Continuous variables reported as median [IQR].
Other includes INBONE/Invision talus, Infinity, and Invision/INBONE talus.
Complications
After matching by age, sex, ASA score, and CCI, there were 57 patients in each group (Table 3). There was no evidence of differences in rates of revision (7.0% same-day discharge vs 0% inpatient, P = .118), reoperation (5.3% same-day discharge vs 5.3% inpatient, P = .999), or complication (15.8% same-day discharge vs 12.3% inpatient, P = .788) between groups.
Outcomes After Matching by Age, Sex, ASA Score, and CCI. a
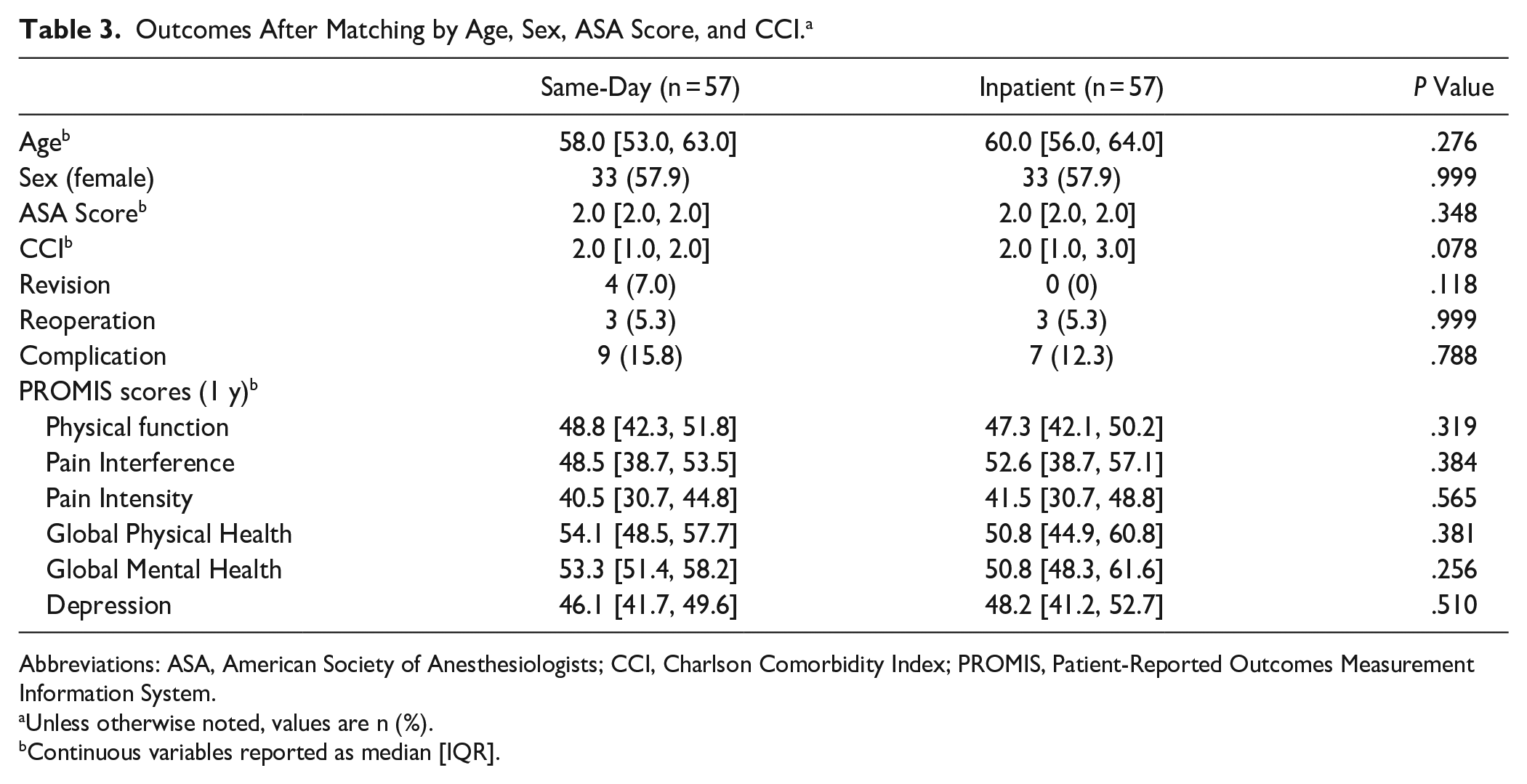
Abbreviations: ASA, American Society of Anesthesiologists; CCI, Charlson Comorbidity Index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Unless otherwise noted, values are n (%).
Continuous variables reported as median [IQR].
Table 4 shows the breakdown of postoperative complications, reported before matching to demonstrate the full spectrum of observed complications. The most common complications were wound complications (3.0% overall) and stress fractures (3.0% overall). There was no evidence of differences in the rates of individual complications for same-day discharge TAA and inpatient TAA.
Types of Complications Following Same-day vs Inpatient TAA (Unmatched).

Abbreviations: CRPS, complex regional pain syndrome; TAA, total ankle arthroplasty.
Neurologic: 1 patient in the outpatient group developed CRPS; 1 patient in the inpatient group had persistent leg weakness requiring prolonged admission.
PROMIS Scores
Median PROMIS scores at baseline were available for 54 of 70 unmatched patients (77.1%) who underwent same-day discharge TAA and for 94 of 118 patients (80.0%) who underwent inpatient TAA. There was no evidence of differences between groups in these scores for any subscales at baseline (Table 1). After matching by age, sex, ASA score, and CCI, PROMIS scores at 1 year after surgery were available for 27 of 57 patients (47.4%) in each matched group. There was no evidence of differences between groups in these scores for any subscales (Table 3).
Multivariable Analysis
Multivariable analyses performed demonstrated no evidence of association between undergoing same-day discharge TAA vs inpatient TAA and reoperation, revision, complication, or 1-year PROMIS scores (P > .05) when controlling for age, sex, CCI (all models), and baseline PROMIS scores (for 1-year PROMIS score models) (Figures 1-3, Appendix).

There was no evidence of association between same-day discharge and reoperation when controlling for age, sex, and Charlson Comorbidity Index.

There was no evidence of association between same-day discharge and revision when controlling for age, sex, and Charlson Comorbidity Index.

There was no evidence of association between same-day discharge and complications when controlling for age, sex, and Charlson Comorbidity Index.
Discussion
There are many stakeholders in decision making for procedure setting. Costs, complications, and patient-reported outcomes are all important metrics. To various degrees, these metrics affect surgeons, patients, hospitals, and insurance payers. If equally safe, the transition to same-day surgery has the potential to ensure patient satisfaction and decrease costs.2,14,17,19,20
In this study, we observed baseline differences in patients undergoing same-day discharge TAA and inpatients, as well as differences in operative variables. Some of these differences were likely a result of intentional selection criteria (comorbidities, insurance type, distance traveled to hospital, social support), whereas others were unintentional but related to patient health and functional status (age, sex, arthritis etiology). After controlling for demographics and clinical risk factors with matched comparisons and multivariable analyses, there was no evidence of association between same-day discharge and complications, revisions, and reoperations at median 1-year follow-up, as well as PROMIS scores at 1 year. Taken together, these findings suggest that same-day discharge TAA is a safe and effective alternative to inpatient TAA.
Given the retrospective nature of our analysis, we would expect that younger, less comorbid patients would be more likely to be indicated for same-day discharge. Prior studies have similarly found baseline differences in patients undergoing outpatient and inpatient TAA.1,6,22,28 Previous studies have shown increased complication and revision rates in TAA in patients with obesity and diabetes.10,25 We did not observe a difference in BMI or in diabetes prevalence at baseline between the same-day discharge TAA group and the inpatient TAA group, suggesting that these factors are not of high importance in determining patient selection for same-day discharge at our institution. The only comorbidity that was different between the 2 groups was the proportion of patients with obstructive sleep apnea, which was higher in the inpatient group. At our institution, even patients with unconfirmed sleep apnea who appear to obstruct during surgery may be required to stay overnight for monitoring. As many ambulatory surgery centers have strict criteria regarding obstructive sleep apnea, this may remain an important determinant of same-day discharge eligibility.
The etiology of patients’ arthritis was different between groups, with patients undergoing same-day discharge TAA more likely to have a diagnosis of instability or posttraumatic arthritis and patients undergoing inpatient TAA more likely to have a diagnosis of primary arthritis or other indications. This observation may be at least partially explained by the difference in age between the 2 groups, with younger, more active patients undergoing same-day discharge TAA more likely to have a diagnosis of instability or posttraumatic arthritis resulting from multiple sprains or trauma, and less likely to have a diagnosis of an age-related degenerative condition like primary arthritis. 28
The implant used was different for same-day discharge vs inpatient TAA, with more INBONE II implants in the inpatient group and more Vantage implants in the same-day discharge group. Stemmed modular implants may be indicated for patients with more severe deformity or other risk factors for mechanical failure. 11 Patients with more challenging cases might be undergoing surgery with the INBONE II implant, and the surgeon’s decision to use this or other stemmed modular implants might reflect more complex surgical cases or additional concomitant procedures. Our results showed that inpatients underwent more concomitant procedures such as medializing calcaneal osteotomy and Cotton osteotomy, which add to the complexity of the case. Patients requiring a medializing calcaneal osteotomy or Cotton osteotomy likely have more significant deformities and may require a stemmed modular implant, as well as be more likely to be admitted following surgery.
There was no evidence of differences in tourniquet times or procedure times between groups, despite the observed differences in concomitant procedures and hypothesized differences in case complexity. It may be that experienced surgeons adjust technique and/or speed to accommodate concomitant procedures and avoid increases in tourniquet time. There were also some procedures (eg, Achilles lengthening and Brostrom repair) that were more common proportionally in the same-day discharge TAA group, although these differences did not reach statistical significance. These factors may at least partially explain the similar tourniquet times and case lengths for same-day discharge TAA and inpatient TAA. For same-day discharge TAA, surgeries started and ended earlier in the day. Surgeons likely schedule outpatient TAA earlier in the day to allow for increased recovery time prior to discharge home and/or to facilitate travel home postoperatively.
We found no evidence of differences in rates of overall complication, revision, or reoperation for same-day discharge vs inpatient TAA. A previous study of same-day discharge vs inpatient TAA found low complication rates in a cohort of TAA performed at an ambulatory surgery center (ASC), with no 30-day readmissions. 8 Another study found that 31% of 16 patients who were admitted for 2 or more nights following surgery had a complication, as opposed to 5% of patients who were discharged same day or admitted overnight. 20 A large propensity score–matched analysis found no differences in rates of operative complications, unplanned readmission, reoperation, or mortality between outpatients and inpatients but was limited to 30 days of follow-up and did not distinguish between same-day discharge and overnight stay. 21
Functional outcomes as measured by PROMIS scores were not different at baseline or at 1 year between groups in our study for any subscales. A previous study of inpatient vs short-stay TAA chose to evaluate clinical outcomes using the visual analog scale, 36-Item Short Form Health Survey total, Short Musculoskeletal Function Assessment (SMFA) function index, SMFA bother index, and American Orthopaedic Foot & Ankle Society (AOFAS) total scores. 1 The inpatient designation group had a worse SMFA function score than the short-stay designation group at baseline, but the inpatient group was able to achieve similar final SMFA function scores postoperatively. There were no differences in improvement between groups from baseline to final follow-up in any of the other scores besides SMFA function.
Many of the findings in our study have been reported previously in the total hip and total knee arthroplasty populations. Age and ASA score have been identified as important predictors of adverse events following same-day arthroplasty, and social support has been consistently cited as essential to optimal recovery.3,4,23,25 A large, multicenter, prospective randomized trial of patients undergoing outpatient vs inpatient THA found no difference in reoperations, readmissions, emergency department visits, or acute office visits. 9 Other matched cohort studies have shown no difference in complications following total hip or total knee arthroplasty in the outpatient vs inpatient setting.7,23 Furthermore, functional outcomes have been shown to be comparable in these populations, with high rates of patient satisfaction.4,7,9,16
Our study was subject to several limitations. Although larger than those prior to compare same-day discharge TAA and inpatient TAA, our final matched cohorts contained only 57 patients in each group, limiting the power of our analysis. We were unable to assess other factors such as social support and physical distance from home to the hospital that are thought to influence selection for same-day discharge and postoperative outcomes. 27 Our same-day discharge surgeries also took place at our hospital rather than an ASC, limiting our ability to draw conclusions about the safety of same-day discharge TAA performed at an ASC.
Despite these limitations, to our knowledge this is the largest study to date to compare same-day discharge TAA and inpatient TAA. We found that, in our US-based health care system with appropriate patient selection including consideration of ankle deformity and anticipated arthroplasty complexity, same-day discharge following TAA can provide an alternative to inpatient TAA with comparable complication rates and functional outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241241300 – Supplemental material for Safety of Same-Day Discharge Following Total Ankle Arthroplasty: A Retrospective Cohort Analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114241241300 for Safety of Same-Day Discharge Following Total Ankle Arthroplasty: A Retrospective Cohort Analysis by Isabel Wolfe, Matthew Conti, Jensen Henry, Isabel Shaffrey, Agnes Cororaton, Grace DiGiovanni, Constantine Demetracopoulos and Scott Ellis in Foot & Ankle Orthopaedics
Footnotes
Appendix
Ethical Approval
This study was a retrospective review of data collected prospectively as part of the IRB-approved Total Ankle Replacement Registry at our US-based institution
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.