
Abstract
Background:
Chronic osteomyelitis of the calcaneus (OC) and open infected calcaneal fractures, especially when complicated by infected soft tissue defects, present significant surgical challenges. Accepted recommendations for the surgical treatment of this pathology are yet to be established.
Methods:
Drawing from our experience and the consensus among experts, we have developed a concept for selecting optimal, well-known surgical approaches based on the specific pathologic presentation. This concept distinguishes 4 main forms of hindfoot infection: infected wounds, open infected fractures, OC, and their mixed forms. Patients with conditions that could confound the treatment outcomes, such as diabetes mellitus and neurotrophic diseases, were excluded from this analysis. We present a retrospective analysis of the treatment outcomes for 44 patients (4 women and 40 men) treated between 2009 and 2022 using some refined surgical techniques. Treatment success was evaluated based on the absence of disease recurrence within a 2-year follow-up, the avoidance of below-knee amputations, and the restoration of weightbearing function.
Results:
The treatment results were considered through the prism of our proposed concept and according to the Cierny-Mader classification. There were 4 instances of disease recurrence, necessitating 6 additional surgeries, 2 of which (4.5% of the patient cohort) resulted in amputations. In the remaining cases, we were able to restore weightbearing function and eliminate the infection through reconstructive surgeries, employing skin grafts when necessary.
Conclusion:
Surgical infections of the hindfoot area remain a significant challenge. The strategic concept we propose for surgical decision making, tailored to the specific pathology, represents a potential advancement in addressing this challenge. This framework could provide valuable guidance for orthopaedic surgeons in their clinical decision-making process.
Level of Evidence:
Level IV, case series.
This is a visual representation of the abstract.
Keywords
Introduction
The management of nonspecific surgical infectious pathology of the hindfoot is a complex and relatively uncommon task. When an infected wound is accompanied by calcaneal osteomyelitis (CO), the issue requires comprehensive treatment involving not only orthopaedic surgeons but also plastic surgeons. 47
In the spectrum of bone infections, OC is encountered in approximately 3% to 10% of cases, as reported by various authors.1,21,38,39 Schildhauer et al 40 even suggest that the frequency of OC may reach up to 11%, particularly affecting 3% to 10% of children. Jenzri M et al 18 noted similar indicators in children. In cases of open calcaneal fractures, the complication rate increases by 5 to 7 times.15,16,33 Many authors have noted that in open calcaneal fractures, infection can affect up to 60% of cases, sometimes necessitating amputations, with postoperative infections affecting up to 25% of patients.6,14,42 As Morgenstern et al 32 have noted, there are currently no specific diagnostic criteria for fracture-related infections. Similarly, Metsemakers et al 30 highlight the lack of consensus among experts regarding the definition of fracture-related infection.
The frequency of wound complications following surgical interventions for closed calcaneal fractures varies from 0% to 27%. 12
Assessing the extent of pathologic focus within the calcaneus can be challenging, as plain radiographs or fistulography often provide an incomplete picture.20,31
On identifying a pathologic focus in the calcaneus, surgical intervention is planned, including the possibility of filling the cavity formed after intralesional resection. The current surgical treatment of CO offers only a limited range of options, including trepanation, partial resection of the calcaneus or total calcanectomy, and amputation below the knee.5,38 Schade 39 asserts that partial resection of the calcaneus or total calcanectomy can be a viable approach to salvage limbs affected by OC. In their work, Bollinger and Thordarson 7 recommend partial resection of the calcaneus if less than 50% is involved in the inflammatory process.
Such radical operations can lead to disability and a reduced quality of life for patients. 17 In case of safe operations after intralesional resection, there is a need to fill the cavity.
Kurien et al 25 demonstrated that there is a wide array of bone graft substitutes available for filling cavities after debridement in patients with osteomyelitis.
Kim et al 24 used antibiotic-containing calcium phosphate cements for filling the cavity in the calcaneus after its intralesional resection with good results. Other authors share this view.19,35,40
An even more complex problem arises when osteomyelitis is coupled with soft tissue defects in the hindfoot region. 50
This leads to the adoption of various approaches for wound closure in the hindfoot, including local and free flaps, skin-fascial flaps, arterial flaps with reverse flow, skin-78 fascial flaps from the opposite limb, and others.2,8,9,13,33,44 Medium skin defects (5-10 cm²) in combination with OC may be addressed with locoregional pedicled flaps, as discussed in the literature.33,41 However, the efficacy of these methods remains unproven. 37 For open, infected calcaneal fractures, external fixation devices and various types of skin grafting are used.27,42,43
In treating patients with this pathology, the goal is to minimize the number of amputations, eliminate the infectious process, and restore limb function. Currently, there is no consensus among specialists regarding optimal surgical interventions for surgical infections of the hindfoot. Therefore, drawing on our experience and the opinions of other experts, we have attempted to formulate a concept for selecting optimal, well-known surgical solutions depending on the condition of the pathologic focus.
A retrospective analysis of the treatment results of our patients with some refined operations is presented from the perspective of this concept.
Patients and Methods
It is crucial to state that our observational study was conducted in strict adherence to the Declaration of Helsinki. This retrospective analysis encompasses 44 patients (4 females and 40 males) treated from 2009 to 2022. Based on our collected data and comprehensive literature review, we devised a strategic scheme for selecting surgical interventions tailored to various pathologies of the hindfoot (refer to Figure 1). This scheme accounts for the intricate nature of the pathologic state and the full spectrum of available surgical techniques.
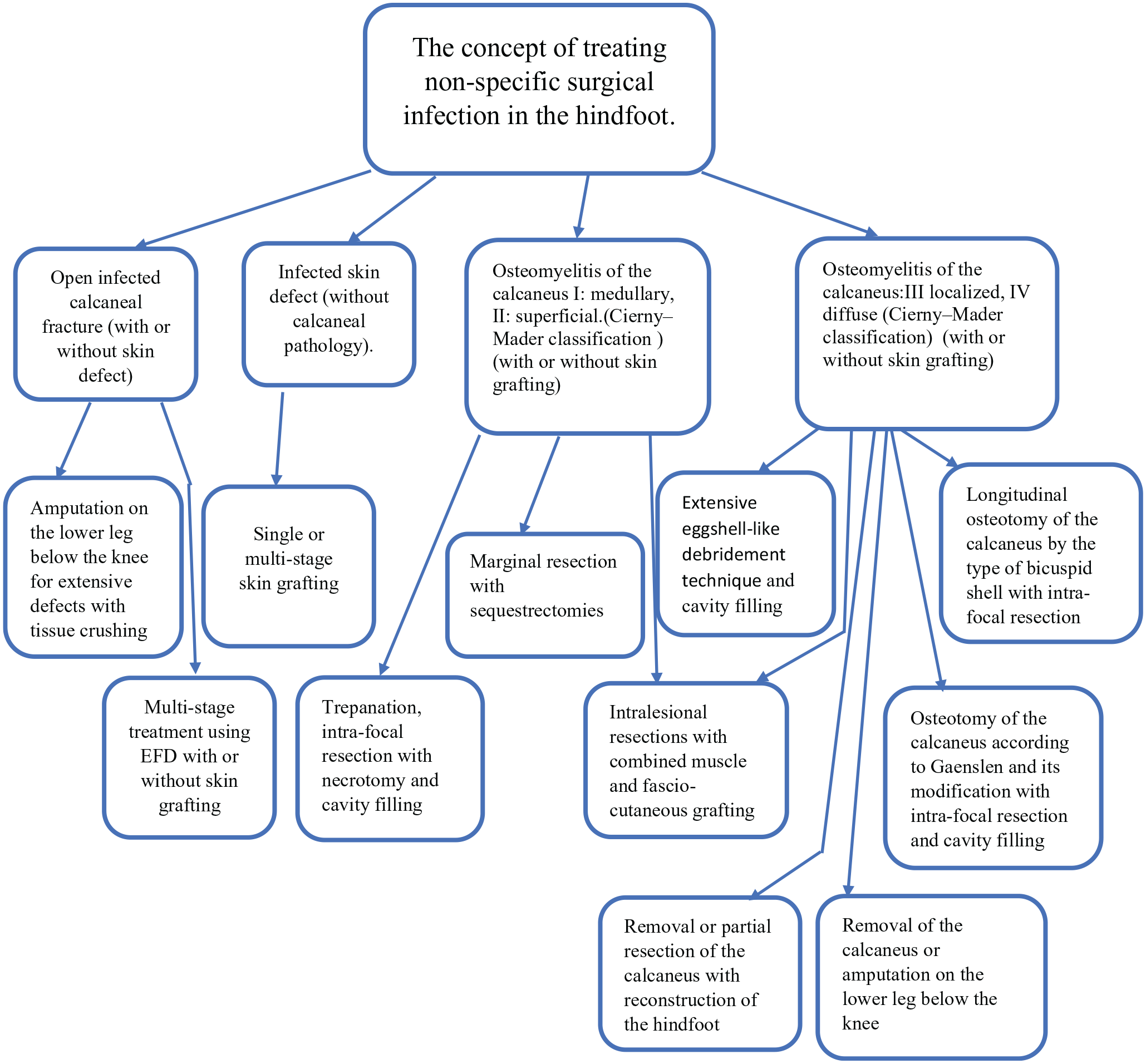
Concept of choosing surgical solutions for infectious pathology in the calcaneus area. EFD- external fixation device.
In our study, we have classified patients with open fractures of the calcaneus older than 3 weeks as cases of fracture-related infection. These 4 patients had open infected fractures of the calcaneus, accompanied by skin defects, and were treated using the Ilizarov apparatus. Within the group suffering from chronic posttraumatic and postoperative osteomyelitis, there were 17 patients with an average age of 43.8 years (ranging from 22 to 71 years) and 10 patients with hematogenous osteomyelitis, averaging 12.6 years of age (ranging from 5 to 34 years) (Figure 2). In 19 cases, we used trepanation followed by necrotomy and subsequently filled the resultant cavities with Bioactive glass (BAG-C53P4), which has garnered positive outcomes in chronic osteomyelitis management. 26

Types of non-specific surgical infection in the calcaneal area.
Additionally, we managed 13 patients with a mean age of 35.9 years (ranging from 15 to 78 years) who presented solely with grade 4 surgical infected wounds per the classification by Gorvetzian and colleagues. 11
For the sizable skin defects, we adopted the Italian method, using a pedunculated fasciocutaneous flap from the contralateral limb in 12 patients. In 2 cases, sural gastrocnemius flaps were used to mend infected wounds. The rest with skin defects benefited from free dermatomal flaps or reconstructive techniques using local tissues. Post healing, any trophic ulcers that appeared on the plantar aspect as a result of ambulation were addressed in a secondary procedure using the Italian method in 2 patients.
Single-stage operations were performed on 25 patients, 2-stage on 15, and 3-stage on 4 patients. Patients with conditions that could confound the treatment outcomes, such as diabetes mellitus and neurotrophic diseases, were excluded from this analysis. Treatment outcome criteria were recurrence of OC, incidence of below-the-knee amputations, and restoration of weightbearing limbs. 22
The overarching aim is to showcase the cutting-edge surgical options available for treating infectious conditions of the hindfoot. The selection of the plastic surgery technique and external fixation devices is at the discretion of the attending surgeon. As depicted in Figure 1, for stages 3 and 4 of osteomyelitis according to the Cierny-Mader classification, surgeons can choose from 3 distinct surgical methods, including our advocated longitudinal osteotomy. Although differing in approach, these methods share the crucial objective of thorough debridement of the pathologic site. We propose that our longitudinal osteotomy is the most efficacious, providing comprehensive debridement across the calcaneus without leaving significant scarring that could later pose complications.
Preserving the limb is our priority, but amputation remains a surgical option when necessary. If the calcaneus cannot be salvaged, reconstructive surgery using the Ilizarov method is a viable alternative.
Recognizing the importance of visual aids in surgery, we present several case examples that correlate with the proposed scheme, assisting surgeons in visualizing the procedures and their potential outcomes.
Examples of Surgical Treatment
Trepanation, intrafocal resection with necrotomy, and cavity plasty
Patient N, a 32-year-old, presented at the clinic with left calcaneal pain and was diagnosed with chronic osteomyelitis of the left calcaneus. The surgical intervention included trepanation and intralesional resection of the calcaneus. The resultant bone cavity was filled with third-generation Bioactive glass (BAG-S53P4) (see Figure 3). This led to the complete restoration of weightbearing capacity, with no relapses observed during the 2-year follow-up period.

Patient N. (A) Radiograph. (B) Magnetic resonance imaging scan. (C) View of the foot before surgery. (D) Intraoperative image showing the insertion of Bon Alive into the calcaneal cavity. (E) Radiograph taken 7 months postsurgery.
Longitudinal osteotomy of the calcaneus
Patient M, a 60-year-old, arrived at the clinic with pain and a fistula on the right foot. The diagnosis was chronic posttraumatic osteomyelitis of the right calcaneus. An L-shaped external approach was used. A longitudinal osteotomy of the calcaneus was executed, and the obtained halves of the calcaneus bone were opened like the valves of a bivalve shell (refer to Figure 4, B). This was followed by internal focal resection and sequestrum necrotomy. After reapproximation of the calcaneal halves, the skin was sutured. Postoperative management included immobilization in a plaster cast. Primary wound healing was noted, and graduated weightbearing was initiated after 2 months (see Figures 4 and 5).

Patient M. (A) Preoperative radiograph. (B) Schematic representation of the longitudinal osteotomy. (C) Intraoperative view of the wound postosteotomy, with necrotic tissues visible. (D) Post-sequestrectomy view. (E) Extracted sequesters and necrotic tissues. (F) Postoperative radiograph.

Patient M. (A) Radiograph at 4 months postprocedure. (B) Radiograph at 7 months indicating complete union at the osteotomy site.
Italian plastic surgery with fasciocutaneous-muscular flap
Patient F, a 27-year-old, presented at the clinic with an infected wound on the right foot. Diagnoses included infected fractures of the cuboid and scaphoid bones, OC, and an extensive necrotic wound on the foot. Initial treatment involved necrotomy of the wound with osteosynthesis, employing the Ilizarov apparatus. For more than 4 weeks, the wound underwent treatment until granulation tissue formed, achieving a depth of 6 cm (Figure 6). The subsequent step included marginal resection of the calcaneus and reconstruction using a fasciocutaneous-muscular flap (Italian plastic surgery). The muscle flaps were harvested from the medial gastrocnemius muscle of the contralateral leg. The donor site was closed using a split-thickness skin graft. Both legs were stabilized using components of the Ilizarov apparatus. After 3 weeks, the pedicle of the flap was divided and sutured to the recipient site (Figure 7). The patient experienced no recurrence of osteomyelitis over the 2-year follow-up and achieved complete weightbearing capabilities without discomfort, eliminating the need for specialized orthopaedic footwear.
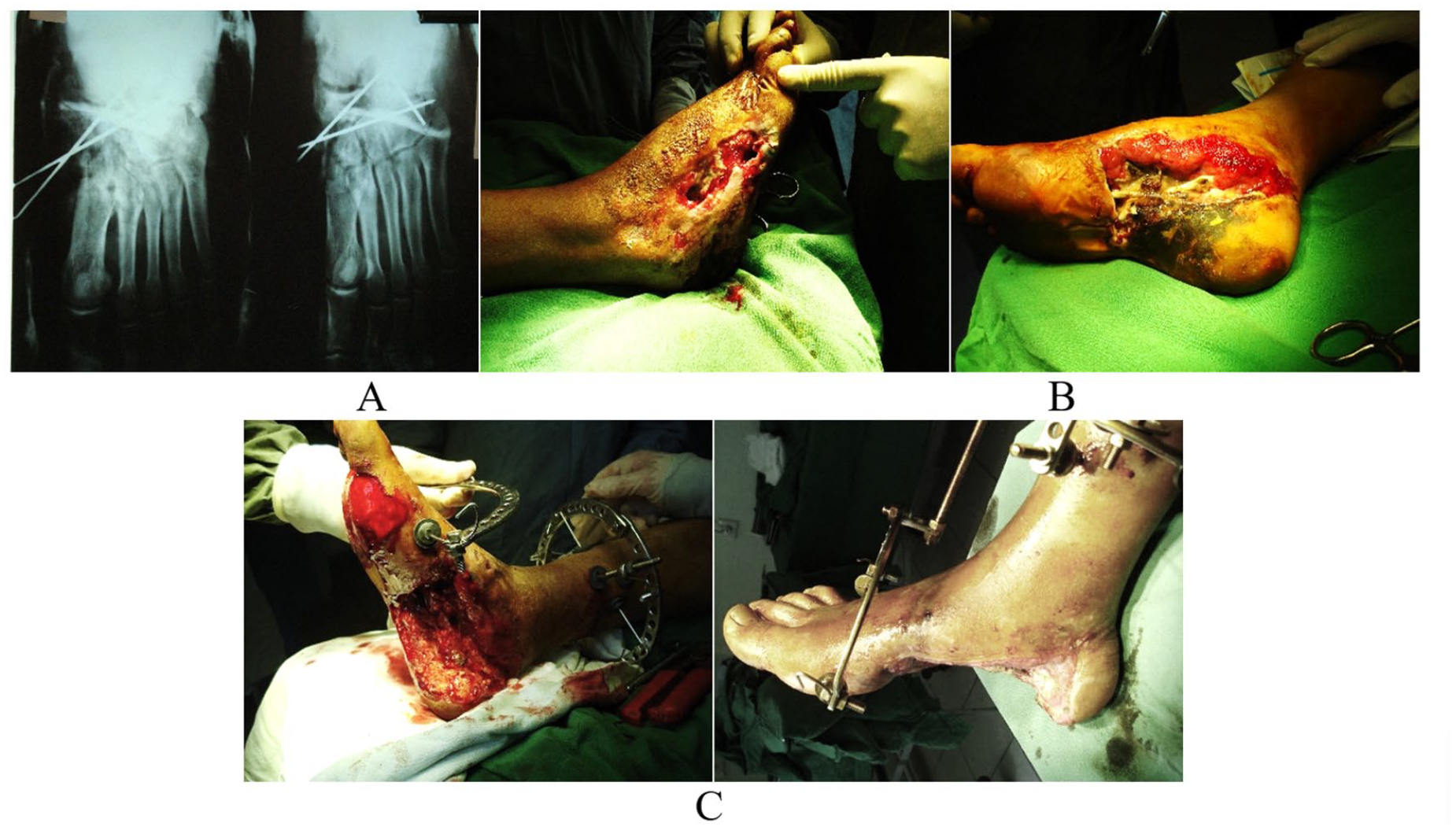
Patient F. (A) Radiograph. (B) View of the foot wound. (C) Foot’s soft tissue defect after the first operation.

Patient M: intraoperative view and postoperative outcomes. (A) Donor site and musculofascial skin flap during surgery. (B) Treatment process with fixation of both legs using an apparatus. (C) Appearance of the donor site. (D) Patient’s foot following flap excision. (E) Two years postsurgery.
Closure of an infected wound of the hindfoot with a sural rotational skin flap
Patient K, a 20-year-old with an infected wound in the hindfoot, was referred to our clinic for further management. The diagnosis was recorded as an infected wound in the left hindfoot. Surgical intervention involved reconstructive plastic surgery using a sural rotational skin flap. A flap, measuring approximately 3 cm in width, was tailored to the wound's dimensions and based on a skin pedicle. The flap was rotated into place from a position 7 cm proximal to the lateral malleolus, followed by a longitudinal incision extending from the flap's base to the wound. The incision margins were meticulously prepared. The skin pedicle was inset into the created space, and the flap was then positioned over the wound and secured with sutures. This surgical technique is designed to prevent flap edema (Figure 8). The patient puts full weight on the leg and wears regular shoes.

Patient K. (A) Preoperative view of the wound. (B) Intraoperative Doppler examination confirming the patency of the superficial sural artery. (C) Surgical stage: excision of the flap. (D) Flap rotation and placement of the fasciocutaneous pedicle in the recipient site are being carried out. (E) Postoperative result of the reconstruction.
Results
In line with our concept, we have mapped out treatment recommendations for 10 patients with hematogenous OC in Figure 1 found in the "Osteomyelitis of the calcaneus" section, according to the Cierny-Mader classification (I: medullary, II: superficial). Under the subsection "Trepanation, intra-focal resection with necrotomy and cavity filling," 8 patients were treated, with 1 experiencing a recurrence of osteomyelitis. The treatment for 2 patients corresponded to the recommendations in the "marginal resection with sequestrectomy" subsection, with one of these patients also experiencing a recurrence. Primary wound healing achieved in 8 patients. All instances of osteomyelitis recurrence were effectively managed with antibiotic therapy.
Evaluating the treatment outcomes for 17 patients with posttraumatic chronic osteomyelitis according to our approach, we provided recommendations for 11 patients presented in Figure 1 under the "Osteomyelitis of the calcaneus" section (III: localized, IV: diffuse—Cierny-Mader classification), divided into 3 subsections. These included the subsection "Longitudinal osteotomy of the calcaneus with intrafocal resection based on the premolar shell type," which resulted in good outcomes for 3 patients. "Extensive debridement using the eggshell technique and cavity filling" was applied to 6 patients, 2 of whom experienced recurrences. "Resection of the calcaneus (with or without skin grafting) or below-knee amputation" was necessary for 2 patients with frequent recurrences.
From the perspective of our concept, the treatment recommendations for the remaining 6 patients aligned with the subsection "Trepanation, intra-focal resection with necrotomy and cavity filling" in the "Osteomyelitis of the calcaneus" section (I: medullary, II: superficial—Cierny-Mader classification) (Figure 1). Of the 17 observed patients, 4 underwent repeat operations during the observation period, including 2 amputations. Primary wound healing was achieved in 7 of these patients. Recurrences were noted in 4 patients during the observation period.
Of the 12 patients who underwent Italian plastic surgery, only 1 developed marginal skin necrosis, which eventually healed by secondary intention. For the 2 patients who received sural flap plasty, their wounds healed primarily. The treatment recommendations for these patients are described in Figure 1 under the "Infected skin defect (without calcaneal pathology)" section and in the "Single or multi-stage skin grafting" subsection.
Overall, the majority of patients successfully regained weightbearing capabilities after the infectious process was eliminated, with the exception of 2 patients who required amputations.
Discussion
Surgical infectious pathologies of the heel area can be categorized into 4 types: (1) infection of a wound without calcaneal involvement, (2) chronic OC, (3) concurrent infected wound and OC, and (4) open infected fractures of the calcaneus. The literature features studies focusing on each pathology type individually. We concur with Sabater-Martos et al 37 who, through systematic analysis, highlighted the complexity of managing these conditions. Their review of 20 studies from 2000 to 2018 found that merely 5 (25%) addressed both soft tissue and bone treatment, reflecting a heterogeneity that hinders the formulation of standardized treatment protocols, which could significantly benefit clinical practice.
Addressing each type of pathology presents significant challenges, particularly when conditions coexist. Our proposed systematization of surgical interventions targets the specific pathologic conditions, offering a concept for treating nonspecific surgical infections in the hindfoot (refer to Figure 1).
For extensive and deep skin defects, Italian plastic surgery employing a fasciocutaneous flap from the contralateral limb demonstrated high success rates with minimal long-term complications. 49
The reverse sural calf flap has become increasingly popular for reconstructing skin defects of the ankle and foot. Tripathee et al 46 support its efficacy in their systematic review of 89 articles, indicating its broad applicability in the hindfoot. However, venous congestion, potentially leading to partial or complete necrosis, is a notable complication of the reversed sural flap. 33
Dhamangaonkar and Patankar 8 have effectively employed a sural fasciocutaneous flap with a dermal pedicle, creating an open channel for the flap by severing a skin bridge between donor and recipient sites. We have successfully adapted this technique for 2 patients with hindfoot wounds.
The choice of the method hinges on the clinic's capabilities and the surgeon's expertise, with the overarching principle being optimal wound closure. In cases of OC, the primary surgical goal is the complete removal of necrotic tissues; however, more radical interventions are sometimes necessary.5,7,26,29,41,42
Researchers are increasingly exploring safer surgical techniques for calcaneus infections.3,23,31,35 Qin et al 35 applied "extensive eggshell-like debridement" to treat localized OC with significant success rates. Similarly, Jiang et al 19 reported limb function preservation and absence of relapses using a comparable approach. In our practice, we typically perform limited trepanation, intralesional resection to healthy tissue margins, and use osteoconductive agents like bioactive glass (BAG-S53P4) for bone cavity filling.
For save operations, Mata-Ribeiro et al 29 and Barbour et al 4 have used a free fibula-flexor hallucis longus osteomuscular flap for partial calcaneus resections. In cases of localized (III) or diffuse (IV) OC classified by Cierny-Mader, our focus is on extensive intralesional resection to excise all altered tissues (see Figure 1).
Babiak et al 3 introduced a method involving reaming of the calcaneus and the insertion of collagen-gentamicin sponges into the boreholes, though this was associated with a higher incidence of subsequent below-the-knee amputations.
In situations of diffuse recurrent osteomyelitis of the calcaneus or extensive skin defects with an infected fracture, amputation of the limb or removal of the calcaneus may be necessary.
In their publication, Kendal et al 22 revisited the Gaenslen 10 technique from 1931, introducing enhancements to the procedure. Despite these improvements, they reported 5 instances of OC recurrence and 2 instances where patients necessitated below-the-knee amputations. Although the technique provides excellent access for addressing the pathologic site, it also results in scarring in the heel and calcaneal prominence, which can be problematic for patients when wearing shoes.
Our team has innovated a longitudinal osteotomy of the calcaneus via an internal approach, aptly named the "bivalve shell technique." This method facilitates extensive intralesional resection, conserving the anatomy of the calcaneus. Our findings indicate a reduced recurrence rate, with patients comfortably wearing standard shoes with supinators posttreatment. We advocate for broader clinical trials to thoroughly evaluate the efficacy of this technique.
Although the literature on OC treatment is extensive, discussions of concurrent OC and skin defect reconstruction are limited.15,34,36,45,47
We contend that such surgical techniques, which strive for limb preservation, should be more commonly employed. Complex cases, especially those necessitating calcaneal reconstruction, may require multiple surgeries and proficiency in Ilizarov techniques.43,48
Consequently, advancements in surgical technology have the potential to decrease the incidence of amputations associated with infectious pathologies of the hindfoot.
Conversely, while amputation may offer faster relief and a quicker return to social activities, it is not without significant long-term costs. MacKenzie et al 28 highlighted that an amputee's lifetime medical care in the United States could reach $509 275 compared to $163 282 for limb reconstruction.
To conclude, the diverse surgical approaches to nonspecific infections in the hindfoot range from amputations to complex reconstructive procedures. The success of these surgeries, which often include plastic surgery for wound closure, depends greatly on the surgeon's choice of intervention. Our concept aims to guide the decision-making process, potentially reducing the need for radical surgeries. We believe that this approach could prove to be a valuable addition to the field, particularly for orthopaedic surgeons early in their careers.
Limitations of the work include retrospective analysis of treatment outcomes, limited sample size for each pathology, and absence of comparative analysis between different surgical procedures. The proposed treatment concept, therefore, is advisory and necessitates validation and potential modification through a large multicenter study.
Conclusion
Infections affecting the bones and soft tissues of the hindfoot represent complex medical challenges that require highly experienced surgeons and specialized treatment facilities. The fundamental goal of treatment is limb preservation, with a focus on maintaining functionality. Our presented surgical concept, which includes procedures such as the longitudinal osteotomy of the calcaneus and fasciocutaneous-muscular nonfree plasty, broadens the spectrum of limb-sparing options available to clinicians. This concept is designed to guide surgeons toward more effective decision making, thereby improving patient outcomes in the management of this severe condition.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241241058 – Supplemental material for The Concept of Treatment for Surgical Infection in the Hindfoot
Supplemental material, sj-pdf-1-fao-10.1177_24730114241241058 for The Concept of Treatment for Surgical Infection in the Hindfoot by Chingiz Alizade, Huseyn Aliyev and Farhad Alizada in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because the work is retrospective. It does not contain any data that would allow identification of any patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.