
Abstract
Background:
Increasing attention is being paid to the costs associated with various orthopaedic surgeries. Here, we studied the factors that influence costs associated with surgically treated acute Achilles tendon tears.
Methods:
We retrospectively identified patients with surgically repaired acute Achilles tendon tears, excluding insertional ruptures or chronic tendon issues. Using the Value Driven Outcome (VDO) tool from our institution, we assessed total direct costs as well as facility costs. Briefly, the VDO tool includes an item-level database that can capture detailed cost data—costs are then reported as relative mean data. Cost variables were adjusted to 2022 US dollars, and total direct cost was compared with patient characteristics using gamma regressions to report cost ratios with 95% CIs.
Results:
Our cohort consisted of 224 patients with Achilles tendon tears surgically repaired by one of 4 fellowship-trained orthopaedic foot and ankle surgeons. There were no differences in demographics, total direct costs, or facility costs based on surgical positioning (prone n = 156, supine n = 68). Open repairs (n = 215), compared with percutaneous techniques (n = 9) that used commercially available instrumentation, had 37% less total direct costs (P < .001, 95% CI 0.55-0.72). Compared with surgery at a main academic hospital (n = 15), procedures at an ambulatory care center (n = 207) had 19% lower total direct costs (P = .040, 95% CI 0.66-0.99) and 41% lower facility costs (P < .001, 95% CI 0.5-0.7).
Conclusion:
Improving cost-effective orthopaedic care remains an increasingly important goal. Patient positioning for Achilles tendon repair does not appear to have meaningful impacts on cost. When clinically appropriate, considering surgery location at an ambulatory center appears to reduce surgical costs.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Costs of surgical care continue to be a topic of great interest in the orthopaedic community. However, little evidence has been published on surgical costs for common orthopaedic foot and ankle procedures like Achilles tendon repair. Acute Achilles tendon injuries can be treated both surgically and nonsurgically.4,5,9,12,16 When treated surgically, variables for surgery can include patient positioning (supine vs prone), with prone being the most common,15,19 as well as approach (open and percutaneous) and surgical location (ambulatory center vs inpatient facility).2,13
Limited evidence has directly compared the variables that influence cost of Achilles tendon surgery. McKissack et al 15 conducted a preliminary study on cost with surgical approach but were limited by a small sample size. Although prior studies have found less operating room time associated with supine surgery, an in-depth cost analysis was not performed.1,19 Bronheim et al 2 did not find any difference in cost between repairs performed in an ambulatory surgery center vs an inpatient facility. Few studies, then, have offered a detailed analysis of costs associated with acute Achilles tendon repair. In this study, we investigated the relative costs in surgery for acute Achilles tendon rupture.
Materials and Methods
Data
Following Institutional Review Board approval, we retrospectively identified 224 patients with surgically repaired acute Achilles tears, excluding insertional ruptures or patients with chronic tendon issues needing surgical intervention. Using the Value Driven Outcome (VDO) tool from our institution, we assessed total direct costs as well as facility costs. 10 Briefly, the VDO tool includes an item-level database that can capture detailed cost data. Costs are reported as relative mean data and not raw numbers because of contractual obligations and institutional policies. Cost variables were adjusted to 2022 US dollars, and inflation-adjusted costs were then converted to relative costs. We considered for inclusion all adults (older than 18 years) and visits from February 2014 to February 2022. Demographic data were collected via electronic chart review.
Surgical Technique
Patients were positioned supine or prone, in standard fashion, largely based on surgeon preference. Open repairs involved a roughly 4 to 5 cm incision along the medial edge of the Achilles tendon and used a size 2 ORTHOCORD (n = 184) or FiberWire (n = 28) in Krackow fashion on both sides of the tear. Suture type was unlisted in 2 surgeries, and 1 patient had suture tape augmentation. Percutaneous repairs (n = 9) involved the use of a suture-passing jig.
Statistical Methods
First, we compared prone vs supine patients based on sociodemographic, clinical, cost, and perioperative characteristics of patients using χ2 or Fisher exact tests for categorical variables, and Wilcoxon rank sum tests for continuous variables. Categorical variables were reported as frequencies and percentages while continuous variables were expressed as means and SDs or medians and interquartile ranges for skewed distributions. Cost variables were adjusted to February 2022 US dollars using the Bureau of Labor Statistics consumer price indices for medical care (CPI-M). The inflation-adjusted cost was then converted to relative cost 21 by dividing by the median adjusted cost for the descriptive summaries.
Univariable and multivariable analyses were then used to assess the relationship between total direct and facility cost with positioning and other patient characteristics. Generalized linear regression models with a logarithmic link were fitted to account for the skewness of the cost distributions. The suitability of inverse Gaussian, Gaussian, and gamma distribution families were evaluated, ultimately selecting the gamma because of results from the modified Park test. 14 In addition, the interaction between positioning and body mass index (BMI) for total cost and facility cost outcomes was examined to assess whether the effect of BMI on cost differs for the different surgical positions.
Variables were excluded that could potentially lead to overadjustment bias 18 (ie, controlling for a variable that is intermediate on a causal pathway from the positioning exposure to the cost outcome) and those with a variance inflation factor of 2.5 or higher from the multivariable analyses. Variance inflation factor was used to detect the presence of multicollinearity. We exponentiated regression coefficients and reported results as ratios with 95% CIs, as well as P values. All P values were 2-sided, and statistical significance was established at the threshold of .05. All analyses were performed with R, version 4.1.3. 17
Results
Table 1 compares demographic and relative surgical costs based on patient positioning. Among the total of 224 patients with Achilles tendon, 156 underwent prone Achilles repair whereas 68 underwent supine repair. No significant differences were found between the 2 groups based on demographic factors.
Demographic and Clinical Characteristics of the Overall Patient Population by Positioning. a

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
Missing values in prone/supine: BMI = 24/18; employment = 20/6; ASA class = 1/0; location = 2/0; room to start, minutes = 5/1; tourniquet time, minutes = 10/6; total OR time, minutes = 5/1.
Wilcoxon rank-sum test.
Chi-squared test.
Fisher exact test.
Costs are summarized as relative costs; supply and implant costs are removed because their median values are zero in both groups.
Median time spent from OR arrival to the start of the repair procedure was longer for patients in prone position (26 minutes) compared to patients undergoing repair in the supine position (22 minutes, P < .001). The median relative total direct (median cost = 1.0) and facility costs (median cost = 1.0) were equivalent between the supine and prone Achilles repair groups. The median relative cost for other services was higher in the supine group (0.9) compared to the prone group (1.0, P = .018). There was no cost association with implant or supply costs (Figure 1).

Graph showing the distribution of cost across Achilles’ tendon repairs.
Table 2 shows the results from the univariable and multivariable analyses for total direct cost. Univariable analyses demonstrated no significant difference between supine and prone position with regards to total direct costs (P = .92, 95% CI 0.94-1.06). For every 10-year increase in patient age at surgery, total direct costs increased by 3% (P = .047, 95% CI 1.01-1.05). Total direct costs increased by 9% (P = .023, 95% CI 1.01-1.17) for males compared to females. Open repair procedures compared to percutaneous procedures reduced total direct costs by 32% (P < .001, 95% CI 0.60-0.78), but this subanalysis may be underpowered for full interpretation given the small sample of percutaneous repairs (n = 9). Surgery at an ambulatory center compared with an inpatient facility reduced total direct costs by 25% (P < .001, 95% CI 0.67-0.83). Every 10-minute increase in either room to surgical start time, tourniquet time, or total operating room time led to an increase in cost of 15% (P < .001, 95% CI 1.09-1.22), 6% (P = .001, 95% CI 1.02-1.09), and 12% (P < .001, 95% CI 1.10-1.15), respectively. BMI was not associated with differences in cost.
Univariable and Multivariable Analysis of Factors Impacting Total Direct Cost.
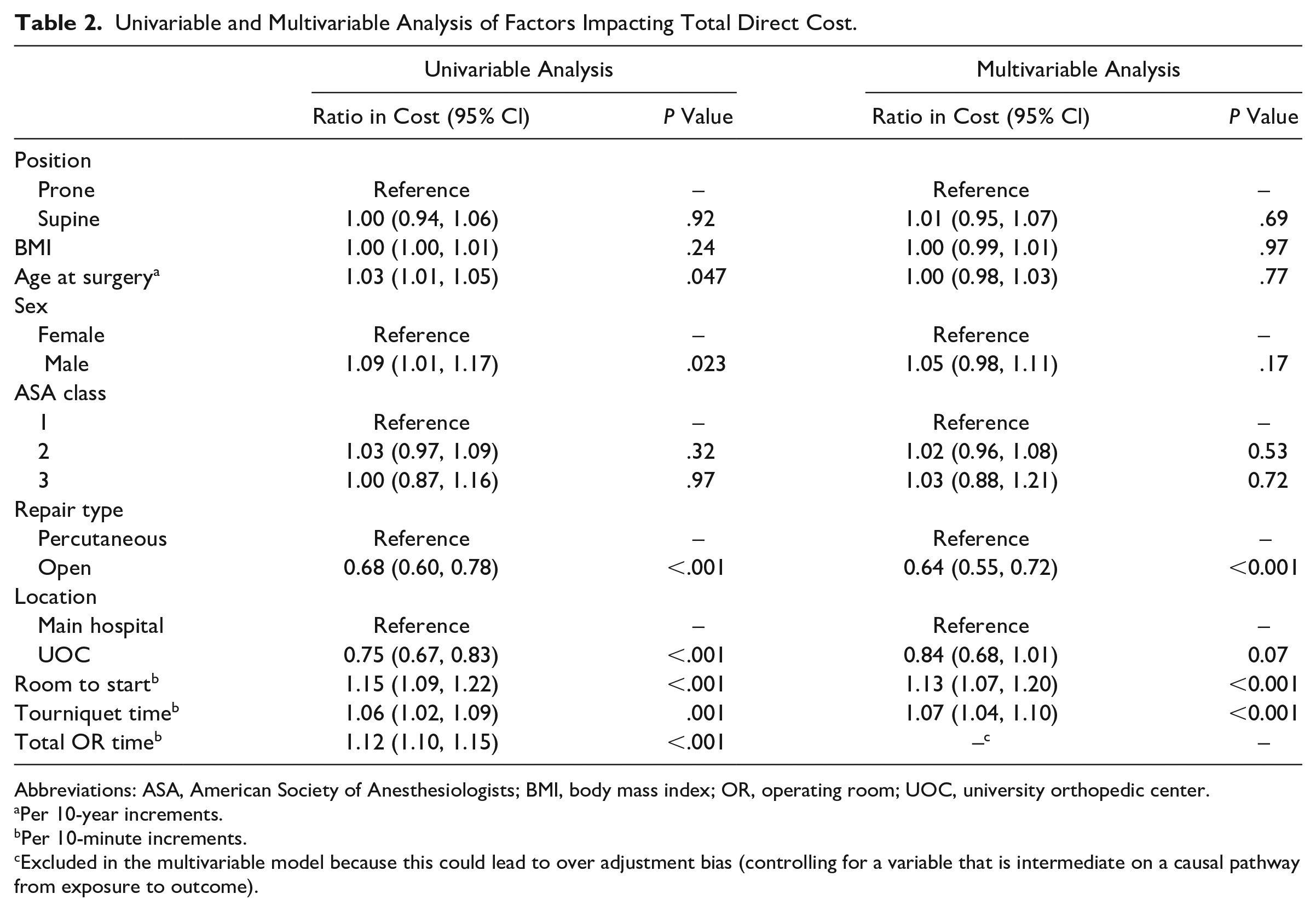
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; OR, operating room; UOC, university orthopedic center.
Per 10-year increments.
Per 10-minute increments.
Excluded in the multivariable model because this could lead to over adjustment bias (controlling for a variable that is intermediate on a causal pathway from exposure to outcome).
Results from multivariable analysis on total direct costs found that open repairs compared to percutaneous procedures were associated with 37% less cost (P < .001, 95% CI 0.55-0.72). Repairs performed at an ambulatory center reduced total direct costs by 19% (P = .040, 95% CI 0.66-0.99). Tourniquet time and room-to-start time were also independent predictors of increased costs, as each additional 10-minute increment increased costs by 7% (P < .001, 95% CI 1.04-1.11) and 12% (P < .001, 95% CI 1.06-1.19), respectively. The interaction between BMI and positioning was not statistically significant (P = .58).
Table 3 shows the results from the univariable and multivariable analyses for facility cost. Univariable analyses demonstrated no significant variation between supine and prone position with regard to facility cost (P = .09, 95% CI 0.90-1.14). With each decade increase in patient age at surgery, facility cost only increased by 2% (P = .17, 95% CI 0.99-1.05). Performing repairs at an ambulatory surgery center reduced facility cost by 44% (P < .001, 95% CI 0.51-0.61). Every 10-minute increase in either room to start time, tourniquet time, or total operating room time increased facility costs by 18% (P < .001, 95% CI 1.10-1.26), 6% (P = .002, 95% CI 1.02-1.11), and 14% (P < .001, 95% CI 1.11-1.12), respectively. Sex and BMI were not associated with facility costs.
Univariable and Multivariable Analysis of Factors Affecting Facility Cost.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; OR, operating room; UOC, university orthopedic center.
Per 10-year increments.
Per 10-minute increments.
Excluded in the multivariable model because this could lead to overadjustment bias (controlling for a variable that is intermediate on a causal pathway from exposure to outcome).
Open repair procedures compared to percutaneous procedures were significantly associated with reduced costs independent of other factors by 12% (P = .043, 95% CI 0.78-0.99). Having the surgical repair done at an ambulatory surgery center also reduced facility costs by 41% (P < .001, 95% CI 0.50-0.70). Tourniquet time and room to start time were also independent predictors of increased facility costs, with each additional 10-minute increment increasing costs by 7% (P < .001, 95% CI 1.05-1.10) and 15% (P < .001, 95% CI 1.09-1.20), respectively. The interaction between BMI and positioning was not statistically significant (P = .42).
Among patients who underwent repair in supine position, total cost (50%) made up the largest proportion, followed by 36.3% for facility cost, 6.4% for other services, 5.7% for pharmacy cost, 1.6% for implant cost, and, lastly, 0.1% for supply cost (Figure 1). Among patients who underwent repair in prone position, total cost (50%) made up the largest proportion, followed by 34.0% for facility cost, 7.3% for other services, 6.1% for pharmacy cost, 2.4% for implant cost and, lastly, 0.2% for supply cost.
Discussion
Increasing attention is being paid to costs of surgical procedures, but limited studies2,15 have evaluated surgical costs for acute Achilles injury repair. This study retrospectively analyzed 224 patients with surgically corrected Achilles tendon injuries including detailed cost analyses. Here, patient positioning for acute Achilles tendon repair does not appear to have meaningful effects on both total direct and facility costs. Surgeries performed at an ambulatory surgery center were associated with significant reductions in cost.
These findings agree with previous research in a number of aspects. McKissack et al 15 demonstrated that the average cost of the prone group (n = 54) exceeded that of the supine mini-approach group (n = 26) by $1823, although this was not statistically significant in their analyses. Although the authors were not able to evaluate overall costs, they attributed this difference to longer operating room (average of 18.7 minutes more for prone approach, P = .001) and postanesthesia care unit times. We found that greater room to start time, tourniquet time, and total operating room time increased total direct costs (by 15%, 6%, and 12%, respectively) and facility cost (by 18%, 6%, and 14%, respectively). In total, we believe that our larger sample size and evaluation of relative cost gives greater insight into an apparent minimal cost difference between the surgical approaches (supine vs prone).
Our results contradict some previous findings about the cost effectiveness of percutaneous approach vs open procedures. In 2013, Carmont and Heaver examined cost differences between the percutaneous and open surgical management of Achilles tendon ruptures. The authors estimated that the percutaneous repair was 361 euros cheaper than the open procedure and suggested that the percutaneous should be the primary method of cost-effective surgical management of Achilles tendon rupture. 3 In contrast, we found that open procedures were relatively cheaper than the percutaneous technique by 32% to 37% for direct cost and 12% for facility cost. The disparities in these findings can possibly be attributed to differences in the UK vs American health care systems as well as differences within the variables used to assess cost. Of note, our sample only had 9 patients who underwent percutaneous repair, which is a notable limitation of our data set.
In previous literature, it has been shown that performing pediatric orthopaedic surgery at an ambulatory center, compared with a university hospital, reduced costs by 17% to 43%. 7 Lower costs in ambulatory surgery centers have also been seen for total ankle arthroplasties, 8 total hip arthroplasty, 20 and unicompartmental knee arthroplasty. 6 Similarly, carpal tunnel release surgery in a procedure room setting minimized direct surgical encounter costs relative to an operating room. 11 In agreement with this, our study showed that direct costs were reduced by 19% to 25% and facility costs by 41% to 44% when performed at an ambulatory surgery center vs a University hospital setting. There have been mixed results in other Achilles tendon cost studies, with some studies showing decreased costs at ambulatory surgery centers 13 and others showing no difference with inpatient settings. 2
Limitations
This study has limitations. Our cohort was, relative to communities across the country, relatively racially/ethnically homogenous. It is unclear, then, how generalizable our data are. Our sample only included 9 patients who underwent percutaneous repair. And although we found that percutaneous repairs were relatively more expensive than open procedures, these findings may be influenced by statistical power. Given our small sample of percutaneous repairs, caution should be made with interpreting these data. Cost differences between open and percutaneous repairs may not be seen at other institutions who perform higher-volume percutaneous procedures and might own the instrumentation needed for such procedures. Or these cost differences may be inverted compared to our findings (cheaper with percutaneous repair). In addition, this cost study only involves the episode of care (ie, surgery) and not subsequent costs that may be incurred. For example, if a patient experienced a postoperative infection, the subsequent costs (ie, antibiotics, possible repeat surgery ± wound care) are not accounted for here.
Conclusion
Improving cost-effective orthopaedic care remains an increasingly important goal. Patient positioning (supine vs prone) for Achilles tendon repair does not appear to have a meaningful impact on both total and facility costs. Surgery at an ambulatory center was significantly less costly than repairs performed at an academic hospital. When clinically appropriate, then, considering surgery location at an ambulatory center may offer an opportunity to meaningfully reduce surgical costs.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241238215 – Supplemental material for Evaluation of Costs Associated With Acute Achilles Tendon Repair
Supplemental material, sj-pdf-1-fao-10.1177_24730114241238215 for Evaluation of Costs Associated With Acute Achilles Tendon Repair by Kade Wagers, Blessing S. Ofori-Atta, William Tucker, Angela P. Presson and Devon Nixon in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the University of Utah (approval number IRB_00071733). The title for the IRB is “EXEMPTION UMBRELLA: Value of the treatment of musculoskeletal disorders at the University of Utah Covered Entity for lower extremity pathologies.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UM1TR004409.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.