
Abstract
Keywords
Introduction
Osteochondral lesions (OCLs) of the tarsal navicular are rare and thought to be due to repetitive trauma caused by excessive shear forces or as a consequence of incompletely healed navicular stress fractures that reach the articular surface. The precarious navicular blood supply further predisposes it to injury and compromises outcomes. Like OCLs of the talus, navicular OCLs can be managed nonoperatively with arch supports, immobilization, limited weightbearing, nonsteroidal antiinflammatory drugs, activity modifications, and physical therapy.1,3 Described operative interventions for navicular OCLs include transplantation of iliac crest bone graft, 3 micronized cartilage matrix, 6 osteochondral autograft transplantation (OATS), 5 and flowable collagen with iliac crest bone marrow aspirate concentrate (BMAC) and fibrin glue. 4 In this report, we present 2 cases of navicular OCLs: one primary lesion treated with autologous bone grafting and cartilage resurfacing with lyophilized collagen II (BioCartilage; Arthrex, Naples, FL) and BMAC, and a second revision lesion after failed microfracture treated with OATS.
Case Report
Case 1: A 15-year-old female high school soccer player and competitive dancer presented with 2 years of chronic dorsal hindfoot pain, initially attributed to a navicular stress fracture. She attempted conservative therapy with activity modification and immobilization. Repeat MRI then revealed hyperintense signal on T2 with cartilage delamination of the right navicular at the middle third of the dorsal aspect of the talonavicular joint, concerning for an OCL, measuring 11.4 mm × 7.6 mm × 8.7 mm (Figure 1). Because of her continued debilitating symptoms despite conservative management, she elected to proceed with surgical intervention, which included augmented microfracture using micronized lyophilized collagen type II cartilage resurfacing with BioCartilage (Arthrex) mixed with BMAC. Given the depth of the lesion of more than 5 mm into subchondral bone, we supplemented with calcaneal autologous bone grafting.

Patient 1. (A) Preoperative radiographs showing navicular cortical irregularity and (B) MRI showing osteochondral lesions with the critical size dimensions of 11.4 mm × 7.6 mm× 8.7 mm.
We began by performing an iliac crest bone marrow aspiration, which was then converted to 3 mL of BMAC using the Angel BMAC System (Arthrex). A dorsal approach to the talonavicular joint was made between the tibialis anterior (TA) and extensor hallucis longus (EHL) tendons, and the joint was distracted using a Hintermann distractor placed dorsomedially and a lamina spreader placed dorsolaterally. The OCL was decompressed and a 0.062 K-wire was used to drill the base of the defect to recruit vascularity. Autograft bone was then harvested from the calcaneus using a 3.5-mm drill sleeve and impacted into the defect until it was flush with the surrounding subchondral bone. We then mixed the BioCartilage with 2 mL of BMAC and laid it onto the surface of the defect (Figure 2). The remaining 1 mL of BMAC was injected into the talonavicular joint.

Patient 1. Intraoperative photograph showing application of the micronized cartilage matrix mixed with bone marrow aspirate concentrate into the base of the defect after autologous calcaneal bone graft was used to level the osteochondral lesion to subchondral bone.
Case 2: A healthy nonsmoking 27-year-old man, on active duty in the Air Force, was referred to our clinic for a right navicular OCL that had failed prior treatment, including physical therapy, immobilization, activity modification, and open microfracture. The patient presented 1 year postoperatively with persistent incapacitating right foot pain, hindering his military duties. He presented with a CT (Figure 3A) and MRI (Figure 3B) showing persistence of his OCL at the same location as the first case: dorsal-central articular margin of the talonavicular joint, measuring 3.9 mm × 6.2 mm × 5.3 mm.
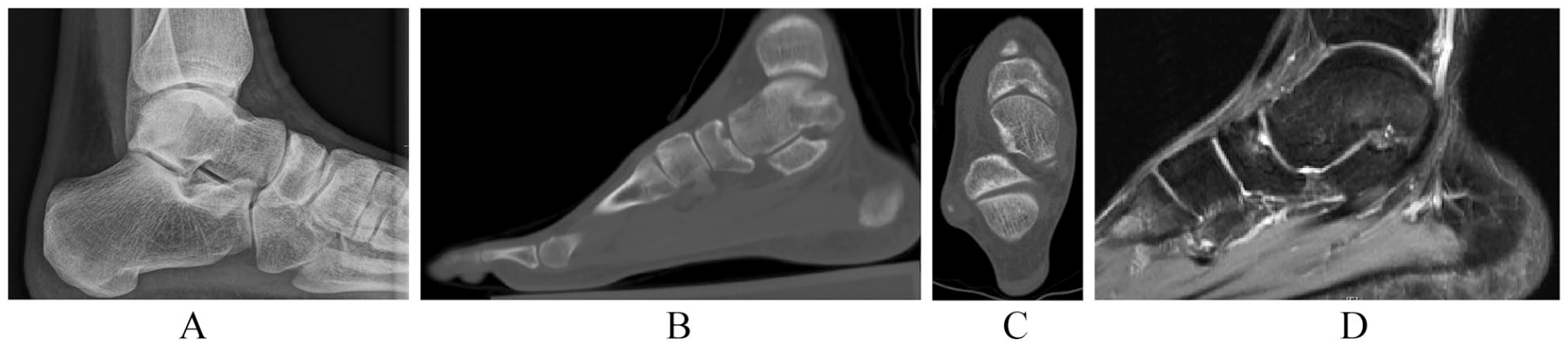
Patient 2 Preoperative radiographs (A), computed tomographic scan (sagittal (B), coronal (C)), and magnetic resonance imaging (D) showing persistence of the osteochondral lesion with cystic changes at the base of the defect after prior microfracture.
A dorsal approach was made at the site of the prior incision in the interval between TA and EHL. The talonavicular joint was distracted in a similar fashion to obtain access to the OCL and the previous site of microfracture was denuded of cartilage. The navicular OCL was curetted down to healthy, stable bone. We then inserted the OATS (Arthrex) guidewire into the center of the defect, reaming 8 × 10 mm.
An 8 × 12-mm OATS plug was then harvested from the superolateral border of the trochlea of the ipsilateral knee and trimmed down to a depth of 10 mm. Returning to the recipient site, we microfractured the defect and used a K-wire to joystick the OATS plug into the center of the lesion, gently tamping down until the OATS plug sat flush with the articular cartilage (Figure 4).

Patient 2. Intraoperative photo.
Postoperatively, both patients remained in a short leg splint until the 2-week follow-up visit, at which time they were transitioned to a boot and allowed range of motion (ROM) exercises, maintaining nonweightbearing status. At 6 weeks, they began touchdown weightbearing for 2 weeks, progressed to flatfoot weightbearing for 2 weeks, and then advanced to full weightbearing at 12 weeks postoperatively.
Results
Twelve weeks postoperatively, both patients had pain-free feet, full ROM, and radiographic evidence of healing of their navicular OCLS. They reported 90% and 80% subjective improvement in their symptoms, respectively. Visual analog scale scores improved from 9 and 8 respectively to 1 in both patients. Both returned to athletics by 6 months postoperatively, which was maintained at 1 year. Patient 1 demonstrative improved Foot and Ankle Ability Measure (FAAM) score from 21 to 77, American Orthopaedic Foot & Ankle Society score 67 to 84, and 12-Item Short Form Health Survey scores 40 (physical component summary [PCS]-12) and 32 (mental component summary [MCS]-12) to 55 (PCS-12) and 35 (MCS-12). Patient 2 demonstrated improved FAMM Score 52 to 84, American Orthopaedic Foot & Ankle Society score 72 to 90, and 12-Item Short Form Health Survey scores 30 (PCS-12) and 60 (MCS-12) to 57 (PCS-12) and 56 (MCS-12). Because of clinical and radiographic improvement, no further advanced imaging was obtained in the follow-up period.
Discussion
Tarsal navicular OCLs are rare; a limited number of case reports have been described in the literature. Therefore, the treatment approach tends to be based on the management algorithm for talar OCLs. One-third of OCLs of the foot and ankle fail conservative management and ultimately require surgical intervention. The gold standard for surgical management of OCLs of the talus is microfracture. For large lesions or those that fail microfracture, other surgical options include osteochondral auto- or allografting, autologous chondrocyte implantation, matrix-based autologous chondrocyte implantation, and biological treatment with BMAC or platelet-rich plasma (Figure 5).1,4,5,7
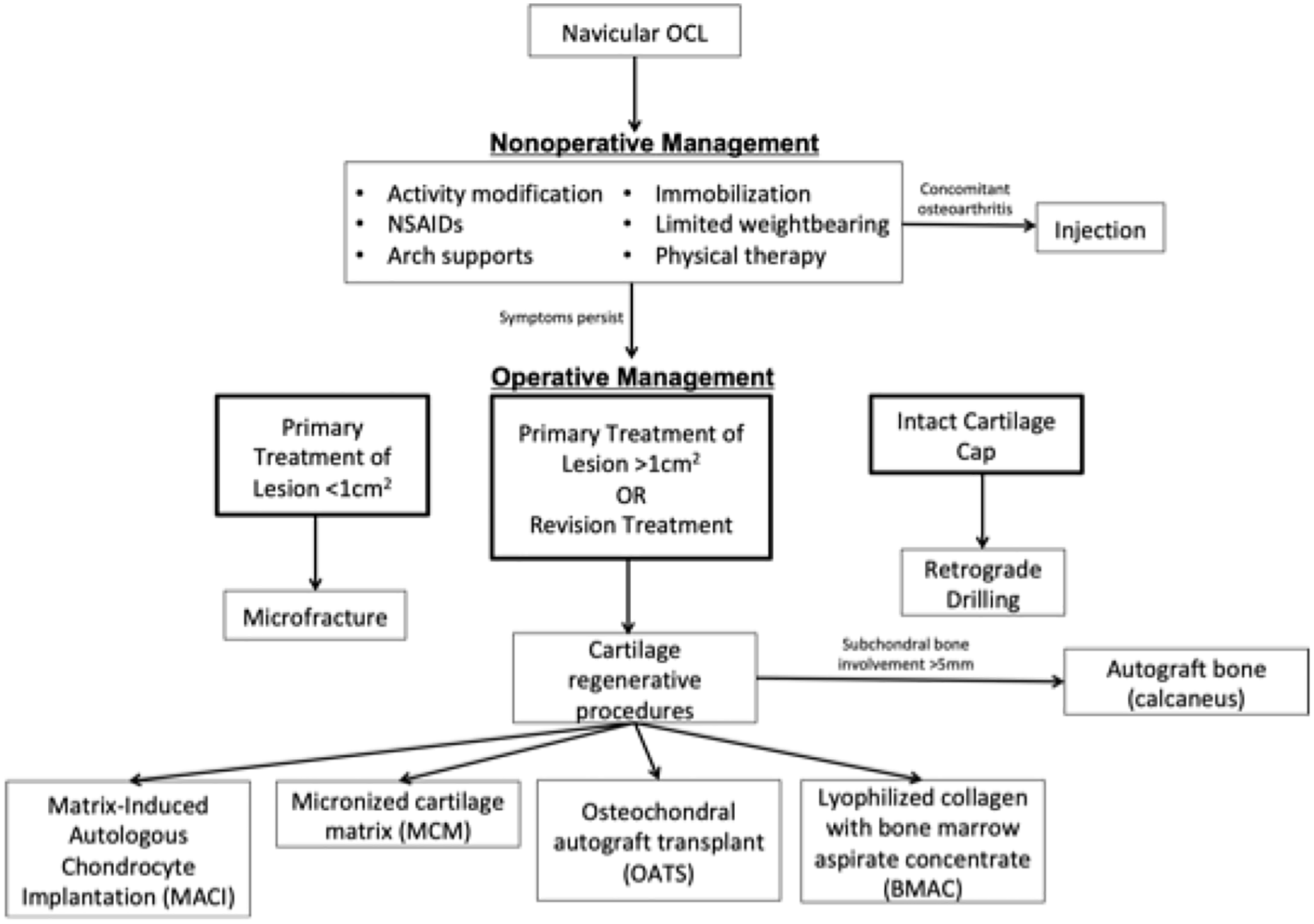
Treatment algorithm for navicular osteochondral lesions.
Our patients both failed nonoperative management, and patient 2 failed prior microfracture. Intraarticular cortisone injections were not offered in our 2 cases because of their young age and risk of cartilage damage and chondrolysis associated with intraarticular steroids. We believe that because of the limited vascularity of the navicular, augmenting microfracture with other cartilage reconstructive procedures is preferred to achieve higher healing potentials, as demonstrated in our limited case series. In the senior author’s opinion, and based on similar recommendations for talar OCLs, extensive involvement of the subchondral bone (>5 mm) is an indication for bone grafting, which was carried out in both of our patients. 2
To our knowledge, this is the first limited case series on reconstructing navicular OCLs with cartilage restorative procedures. The small number of cases in a single-surgeon practice is a limitation of this study. Further, large-scale studies are required to validate the superiority of one treatment modality over the other, which remains challenging because of the limited incidence of this pathology.
Conclusion
OATS and calcaneal autograft transplantation with lyophilized cartilage and BMAC can be used to surgically manage navicular OCLs that have previously failed conservative and/or prior microfracture treatments. More than 12 months out from their respective procedures, both of our patients exhibited clinical and radiographic signs of healing, with return to prior activity levels. No further advanced imaging was ordered given both patients’ clinical improvement. Because of the paucity of data regarding surgical management of navicular OCLs, careful patient selection and further observation is necessary, with the need for evolution of tarsal navicular specific algorithms to effectively manage such a challenging pathology.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241229092 – Supplemental material for Reconstruction of Navicular Osteochondral Lesions: Two Case Reports With Short-term Follow-up
Supplemental material, sj-pdf-1-fao-10.1177_24730114241229092 for Reconstruction of Navicular Osteochondral Lesions: Two Case Reports With Short-term Follow-up by Katherine Wood, Ryan Morrisett, Ty Reasnor and Amgad M. Haleem in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for this study because it is a case report. The cases presented are HIPAA compliant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.