
Abstract
Background:
Ankle sprains are a common musculoskeletal injury among the general population and often involve the lateral ligament complex. Although the majority of ankle sprains are treated successfully with nonsurgical conservative measures, an estimated 5% to 20% of ankle injuries ultimately develop chronic lateral ankle instability (CAI). Multiple surgical treatment modalities for the lateral ankle complex exist, such as anatomical and nonanatomical reconstruction. The current gold standard for primary surgical repair is the Broström-Gould procedure. This is the first article to provide PROMIS scores following BG and the largest study with 5-year outcomes for an open BG.
Methods:
This was a descriptive study of a retrospective cohort of patients undergoing a BG with a minimum follow-up of 5 years. Patient-reported outcome instruments collected postoperatively were PROMIS Pain, Physical Function, Depression, and FAAM. Further preoperative clinic characteristics were analyzed to correlate with the final outcome. The electronic medical record was queried for Current Procedural Terminology (CPT) code 27698 (Broström-Gould) from January 2010 to June 2017. Surveys were conducted in the clinic and through phone interviews. Patient charts were reviewed to obtain basic patient demographic information including sex, age, race, and body mass index (BMI). The following preoperative variables were recorded: history of prior CAI procedures, history of major trauma, duration of symptoms, number of diagnosed ankle sprains, other collagen pathologies, generalized ligament laxity, participation in sports/activity level, peroneal subluxation, clinically diagnosed peroneus longus or brevis tendinopathy, deltoid ligament injury, anterior ankle impingement, and posterior ankle impingement. The PROMIS and Foot and Ankle Ability Measure (FAAM) scores were obtained with a combination of clinic and phone interviews. Data were aggregated in Microsoft Excel and entered in R (version 4.2.0) for statistical analysis.
Results:
Our results show that the minimum 5-year patient-reported PROMIS scores for patients following a Broström-Gould procedure are as follows: PROMIS physical function, 50.5; PROMIS pain interference, 48.2; and PROMIS depression, 38.2. This indicates, at a minimum, that patients 5 years removed from the procedure are within 1 SD of the general population in regard to PROMIS physical function and pain. Our patient-reported FAAM, activities of daily living, and FAAM sports scores were 59.6 and 13.0 respectively. Preoperative magnetic resonance imaging (MRI) findings were recorded. Arthroscopic examination was performed before lateral ligaments reconstruction for patients with intra-articular pathologies confirmed on MRI.
Conclusion:
The findings from our study offer evidence supporting the effectiveness of the Broström-Gould procedure to be associated with normal physical function, even 5 years after surgery. Furthermore, our research identified specific factors such as tobacco use, diabetes, and sports participation that independently correlated with reported outcome measures. These insights enable physicians to better manage patient expectations and tailor treatment strategies accordingly. Our study establishes a foundation for future prospective research endeavors that aim to leverage the PROMIS system for comprehensive outcome assessments.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Ankle sprains are a common musculoskeletal injury among the general population and often involve the lateral ligament complex. 6 Although the majority of ankle sprains are treated successfully with conservative measures, such as anti-inflammatories and early mobilization of the ankle, an estimated 5% to 20% of ankle injuries ultimately develop chronic lateral ankle instability (CAI). 12 Criteria for diagnosing CAI include pain, swelling, unpredictable inversion of the foot during toe-off or heel strike, and/or recurrent ankle sprains within 12 months of the initial ankle sprain. 14 Current clinical guidelines suggest that for patients with CAI ≥3 months’ duration with failed conservative management, surgical repair of the lateral ligaments along with adjuvant procedures can be helpful.
Multiple surgical treatment modalities for the lateral ankle complex exist, such as anatomical and nonanatomical reconstruction. The current gold standard for primary surgical repair is the Broström-Gould (BG) procedure.6,22 The Broström procedure, first implemented in 1966, used a direct repair of the anterior talofibular ligament (ATFL). It is now typically used with the Gould technique, which involves mobilization and incorporation of the inferior extensor retinaculum. 13 The BG procedure, through use of the inferior extensor retinaculum, increases structural integrity, offers operative versatility for reoperation, and a success rate of 85% to 95%. 13
Current systematic reviews of the available literature on long-term patient outcomes of BG procedures show high success rates (≥85%) and low revision rates (≤1.2%). 13 Currently, there is a paucity of mid- to long-term patient-reported outcome studies following the BG procedure. Additionally, there are no long-term studies using the Patient Reported Outcome Measurement Information Systems survey (PROMIS) or Foot and Ankle Ability Measure (FAAM). PROMIS and FAAM are both validated in the literature as superior methods for analyzing patient-reported outcomes following foot and ankle orthopaedic procedures. 8 This is the first article to provide PROMIS scores following BG, and the largest study with 5-year outcomes for BG with additional procedures.
The purpose of this study is to demonstrate 5-year patient-reported outcomes following the BG procedure for the treatment of CAI in the general population. This will provide valuable insight into the long-term efficacy of the BG procedure. Additionally, our regression analysis portrays information on which individual patient factors independently influence patient-reported outcome scores. We looked at the safety, efficacy, and effect that BG procedure had on patient-reported outcomes, such as PROMIS pain interference and depression scores. We also looked to identify specific factors that influence patient-reported outcomes. This adds to the literature by using PROMIS scores, which is a relatively new and comprehensive tool that offers a broader assessment of patient outcomes compared to traditional scoring systems. PROMIS scores have gained popularity in research and clinical contexts because of their standardized nature, precision, patient-centric approach, capacity to minimize burden, and comprehensive evaluation when contrasted with conventional outcome measures.
Methods
Following approval from our institution’s IRB, the electronic medical record was queried for Current Procedural Terminology (CPT) code 27698 (Broström-Gould) from January 2010 to June 2017. Patients were included in this retrospective clinical study if they had a preoperative diagnosis of chronic lateral ankle instability and failed nonoperative management. Patients were excluded if they had undergone any surgeries since their BG repair (except revision BG repair), had a follow-up of less than 5 years, were age <18 years, or declined to answer all PROMIS and FAAM surveys. Surveys were conducted in the clinic and through phone interviews.
Using the electronic medical records, patient charts were reviewed to obtain basic patient demographic information including sex, age, race, and body mass index (BMI). Comorbidities including, but not limited to, tobacco use, diabetes, hypothyroidism, and rheumatoid arthritis were also recorded.
The following preoperative variables were recorded: history of prior CAI procedures, history of major trauma, duration of symptoms, number of diagnosed ankle sprains, other collagen pathologies, generalized ligament laxity, participation in sports/activity level, peroneal subluxation, clinically diagnosed peroneus longus or brevis tendinopathy, deltoid ligament injury, anterior ankle impingement, and posterior ankle impingement.
Preoperative magnetic resonance imaging (MRI) findings were recorded, if present, and included talar osteochondral (OCD) lesion, tibial OCD, peroneus longus/brevis tendinopathy, and osteoarthritis in the foot and ankle. Arthroscopic examination was performed before lateral ligaments reconstruction for patients with intraarticular pathologies confirmed on MRI. Intraoperative anterior drawer and varus talar stress examinations were performed and peroneal tendons were inspected for any tendinosis or tendon tear.
Additional procedures were performed if necessary and included lateral calcaneal slide osteotomy, peroneal groove deepening, excision of posterior impingement, and peroneal debridement with repair.
Complications recorded during follow-up included deep and superficial infections, superficial peroneal nerve palsy, sural nerve palsy, iatrogenic neuromas, reflex sympathetic dystrophy, overtightness, recurrent instability, and reoperations. Deep infections were characterized by the need for a formal irrigation and debridement.
Patient-Reported Outcomes
The PROMIS and Foot and Ankle Ability Measure (FAAM) scores were obtained with a combination of clinic and phone interviews. The PROMIS pain interference (PI) version 1.1, physical function (PF) version 1.2, and depression (PD) version 1.0 computer adaptive test (CATs) were collected and are composed of 40-item, 12-item, and 29-item question banks, respectively. CATs effectively reduce the total number of answered questions through an algorithm that selects the most relevant question based on the patient’s previous answers. Each PROMIS domain has a mean T score of 50, representing the general population, and an SD of 10. A T score is a standardized score used to compare and interpret data in relation to a reference population. It converts raw data into a standard score, allowing for easier comparison and interpretation of results, to assess and compare measurements across different populations or groups. A higher score correlates with more association with the category. For example, a patient with a pain interference score of 60 has a pain score 1 SD above the general population.
Foot and Ankle Ability Measure
The FAAM activities of daily living (ADL) is composed of 21 standard questions in addition to the 8-question sports subscale. The questions are scored on a 4-point scale (1-4). For both components, a higher score correlates with a higher level of physical capacity. Multiple studies have shown the FAAM to be a reliable and valid instrument for evaluating CAI. FAAM scale has been reported as a “good compromise” when compared to American Orthopaedic Foot & Ankle Society (AOFAS) and Chronic Ankle Instability Scale scoring systems. 8
Statistical Analysis
Data were aggregated in Microsoft Excel and entered in R (version 4.2.0) for statistical analysis. All continuous variables were first evaluated for normality via the use of a Shapiro-Wilk test. After checking for normality, Mann-Whitney U tests and Spearman correlations were used to assess the association of categorical and continuous variables, respectively, on FAAM and PROMIS domains. A linear regression model was constructed to evaluate the independent effect of variables on each FAAM and PROMIS outcome instrument. Variables were included in the regression model based on an a priori significance threshold of P <.1 in bivariate analysis.
Results
From our CPT pull, 254 total patients had the procedure with our CPT code of interest (27698) in our time frame of January 2010 through June 2017. Of these patients, 149 patients were female (58%) and 105 patients were male (41%). From this original cohort, 64 patients responded to the questionnaires fully, and 190 patients from the original cohort either did not respond to the questionnaire, had missing data, or did not meet our inclusion and exclusion criteria. Our cohort included patients aged 15 to 73 years, with BMIs ranging from 19.33 to 51.58. Among the 64 patients, 17 had previously undergone surgeries for ankle instability, and all 64 patients had been experiencing symptoms chronically for at least 6 months.
Of the total 64 patients in the study, 9 (14.1%) made up the cohort that had an isolated BG procedure, without any concomitant procedures. We were able to get complete follow-up information for all of these patients. Regarding patients who had concomitant procedures, 16 of 64 had calcaneal osteotomies (25%), 2 patients had peroneal groove deepening (3.1%), 50 patients had peroneal debridement (78.1%), 13 patients had peroneal tenodesis (20.3%), and 7 patients had longus to brevis transfer (10.9%).
Of the total 64 patients, wound dehiscence occurred in 1 patient (1.6%, P = .95). Similarly, sural nerve palsy occurred in 1 patient (1.6%, P > .99), reflex sympathetic dystrophy was seen in 1 patient (1.6%, P > .99); and overtightness was seen in 1 of 64 patients (1.6%, P = .95). Instability recurrence was a complication seen in 4 of the patients (6.3%, P = .698). Of the total cohort, 6 patients (9.4%) required reoperation.
Our results show that the minimum 5-year patient-reported PROMIS scores for patients following a BG procedure are as follows: PROMIS physical function (PF), 50.5; PROMIS pain interference (PI), 48.2; and PROMIS depression (D), 38.2. This indicates, at a minimum, that patients 5 years removed from the procedure are within 1 SD of the general population in regard to PROMIS physical function and pain. Our patient-reported FAAM, ADL, and FAAM sports scores were 59.6 and 13.0, respectively. Detailed results are demonstrated below.
Basic patient demographics, associated comorbidities, and concomitant pathologies are outlined in Table 1.
Patient Demographics and Concomitant Pathologies. a

Abbreviations: BMI, body mass index; MRI, magnetic resonance imaging; OCD, osteochondral.
Unless otherwise noted, values are n (%).
Patient-reported outcomes for FAAM sports, FAAM ADL, PROMIS PF, PROMIS PI, and PROMIS depression at a minimum 5-year clinical follow-up are displayed in Table 2.
Minimum 5-Year Patient Reported Outcomes.

Abbreviations: ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; PF, physical function; PI, pain interference; PROMIS, patient reported outcome measurement information systems survey.
Linear regression to understand the factors significantly impacting patient reported outcomes are seen in Table 3. To show normality of the data, population and sample means and SDs are compared in Table 4. In summary, the following variables were statistically significant: FAAM score peroneal tenodesis, FAAM ADL tobacco use, PROMIS PF age > 50, PROMIS PI tobacco use, diabetes, participate in sports activities, PROMIS depression age > 50, history of major trauma, varus stress test, and tobacco use.
Individual Regression Analysis for Each Outcome Measure.

Abbreviations: ADL, activities of daily living; FAAM, Foot and Ankle Ability Measure; PF, physical function; PI, pain interference; PROMIS, patient reported outcome measurement information systems survey.
Population Mean Compared to Sample Mean.
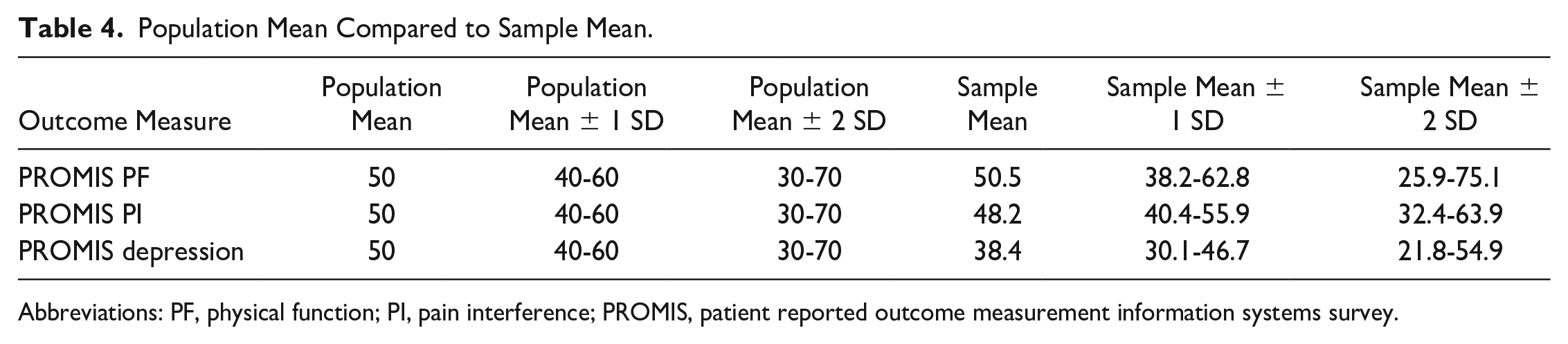
Abbreviations: PF, physical function; PI, pain interference; PROMIS, patient reported outcome measurement information systems survey.
Discussion
BG repair, along with adjuvant procedures, is a viable surgical option for patients with failed conservative management for CAI. 14 To our knowledge, this is the first 5-year outcome study to incorporate PROMIS scores for patients who underwent the BG procedure for CAI. The Broström technique involves repairing the AITFL and CFL and is proposed to restore hindfoot kinematics. 9 The Gould modification additionally repairs the pathologic lateral ligaments while reinforcing the repair with the IER, with the goal of providing additional stability and support against ankle inversion.
A review of the literature yielded few long-term outcome studies following the open BG procedure with adjuvant procedures. Additionally, the majority of the studies reviewed utilized AOFAS scoring. 7 Bajuri et al 2 , in an outcome study following a BG with a PopLok knotless suture anchor, reported 12-month postoperative AOFAS scores of 93.5. Woo et al 20 , in a comparison study between arthroscopic and open BG, found that AOFAS scores were significantly better in the arthroscopic group at the 12-month follow-up (94.2 vs. 70.9 respectively), and these results are supported by Attia et al. 1
Tay et al 17 analyzed outcomes following BG procedure with and without a periosteal flap augmentation and found AOFAS scores to be 90 and 88, respectively, at 2 years. Other mid- to long-term outcome studies have found AOFAS scores to all fall within the minimal clinically important difference (MCID) of each other at follow-ups ranging from 25 months to 10 years. 7
The point of mentioning these studies is to illustrate the absence of literature focusing on long-term patient outcomes, specifically patient-reported outcomes incorporating the superior PROMIS scoring system. 8 To our knowledge, our study is the first to use the superior PROMIS scoring, while simultaneously incorporating a 5-year minimum follow-up, in an attempt to shine a light on the long-term efficacy of the BG procedure, with adjuvant procedures, for patients experiencing CAI. Additionally, this article can serve as a comparison framework for future studies hoping to use the PROMIS system.
It is well known that chronic lateral ankle instability often encompasses numerous different pathologies. These include attenuation of the lateral ligaments, peroneal tendon tenosynovitis, and the occurrence of intra-articular damage from repetitive trauma. 15 The prevalence of many of these concomitant pathologies often necessitate concomitant procedures in addition to the BG procedure. On reviewing the literature, we found that few studies have focused on the relationship between osteochondral defects and peroneal pathology in patient-reported outcomes following a BG. 9 Our study is one of the few to isolate patient factors that influence long-term PROMIS and FAAM outcome scoring following the BG procedure.
In our linear regression analysis, the presence of peroneus longus tendinopathy predicted lower FAAM sports scores. Interestingly, in accordance with current literature, peroneus brevis pathology, tibial, or talar OCD lesions did not independently predict a difference in any of the patient-reported outcomes scores. 9 The fact that peroneal pathology is a common concomitant finding in CAI may provide reasoning as to why its presence does not impact long-term patient-reported outcomes. 4
Additionally, multiple patient demographics that independently influence patient-reported outcomes were isolated. Tobacco use shows a strong negative correlation with FAAM ADL scores and a strong positive correlation with PROMIS pain scores when compared to non–tobacco users. The concept of tobacco usage negatively impacting orthopaedic outcomes has been widely reported in the literature, especially its influence on nonunion, avascular necrosis, wound healing, and functional outcomes. 12 Furthermore, a 2021 systematic review by Heyes et al 7 concluded that tobacco use negatively affects pain control and functional outcomes following foot and ankle procedures, likely because of the peripheral nature of the vasculature and tobacco’s vasoconstrictive effect. Additionally, in 2019, a systematic review by Beahrs et al 3 included 52 articles and concluded that patients undergoing foot and ankle procedures who use tobacco have more pain, lower overall patient satisfaction, and higher rates of wound healing complications.
Diabetes was found to be an independent factor associated with decreased PROMIS pain. These results are likely due to the diminished peripheral sensation associated with diabetes due to effects on peripheral microvasculature. 11 Moreover, literature has identified diabetes mellitus as a risk factor for noninfectious complications in foot and ankle surgery, corroborating our results, as diabetes patients typically have more comorbidities and systematic issues with peripheral vasculature. 21 Nonetheless, it is an important comorbidity that needs to be discussed when counseling patients prior to surgery. Special consideration should be paid to the HbA1c values, as poorly controlled diabetes will typically have more profound systemic repercussions.
A meta-analysis in 2019 by Vuurberg et al 19 demonstrated there is a correlation with increasing weight and BMI with the presence of CAI; however, they did not look into surgical outcomes. Numerous studies have demonstrated the increased incidence of foot and ankle pathologies and decreased response to conservative and surgical management in patients with elevated BMI. 5 This is likely due to a combination of factors including altered biomechanical loading and chronic inflammation due to cytokine release from adipose tissue. 16 Obesity and its negative impact on orthopaedic surgical outcomes is a topic that has been well documented, although our analysis did not predict BMI to independently impact our patient-reported outcomes.
Resiliency is an emerging topic of study in orthopaedics. 10 Participation in sports activities was found to be an independent factor associated with decreased reported PROMIS pain. This finding, supported by the available literature, is likely due to the increased resiliency associated with former athletes and provides a unique avenue for future studies.
Although the study’s retrospective nature precludes a causal relationship from being drawn, our findings substantiate other long-term outcome papers. 18 We believe the available evidence suggests preoperative counseling and expectation management for tobacco users, patients with diabetes, and those with active sports participation.
The reoperation rate among patients for this cohort was 9%, which is higher than the 1.2% reoperation rate reported in the systematic review by So et al. 13 Of the reoperations, 6 had a BMI >30, 3 were smokers, and 1 patient had diabetes. The thought process behind the increased reoperation rate likely involves the elevated BMI of our cohort of community ambulators (50% individuals with >30 BMI). Although BMI has not been proven to directly correlate with adverse outcomes following the BG procedure, the increased stress placed on the repair is intuitive and provides a possible explanation. Furthermore, the average age of the individuals in our cohort was 40.6 years, which is significantly older than the 20.7-30.2-year range reported in So et al. This indicates that our sample might not perfectly mirror the broader population demographics. These findings, coupled with the relatively small sample size, may provide possible explanations for the results. Although this cohort exhibited a high occurrence of concomitant pathologies and procedures, they were similar to the general population in pain and function.
This study’s novelty lies in its use of validated outcome measures, long-term follow-up, comprehensive analysis of patient factors, and its potential to serve as a reference for future studies. These aspects contribute to the unique contribution of the study to the existing literature on patient-reported outcomes following the BG procedure for chronic lateral ankle instability.
One of the major strengths of this study is that all the patients were operated on by a single fellowship-trained foot and ankle surgeon. Additionally, the minimum clinical follow-up was 5 years, which provides novel information on mid- to long-term outcome data. Furthermore, we conducted a comprehensive analysis of patient factors independently influencing the PROMs, which will assist with preoperative counseling and expectation management.
There were limitations to this study. Most notably the fact that preoperative FAAM and PROMIS scores were not obtained, limiting our conclusions on the specific amount of improvement provided to the patients by the procedure. However, because of the intrinsic nature of PROMIS scoring, we were able to see that the PROMIS PF and PI scores were almost exactly equal to the general population. This was also a retrospective study, which introduces unavoidable bias. Additionally, our patient cohort is not representative of a typical patient undergoing a BG procedure. The majority of our patients were aged >40 years, had a BMI >30, and were far cries from a “young athlete.” However, it does shine a light on the outcomes following a BG repair for the generic community ambulator.
Conclusion
Our study provides evidence that the BG is an effective procedure even after 5 years from surgery, as demonstrated through average for population PROMIS physical function and pain scores postoperatively. Additionally, it identifies potential factors (tobacco use, diabetes, sports participation) that independently correlate with reported outcome measures and allows physicians to better manage patient expectations. Through this study we have provided the framework for future prospective studies hoping to use the PROMIS system to assess outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241228272 – Supplemental material for Patient-Reported Outcomes Following Open Broström-Gould Procedure: Minimum 5-Year Follow-Up
Supplemental material, sj-pdf-1-fao-10.1177_24730114241228272 for Patient-Reported Outcomes Following Open Broström-Gould Procedure: Minimum 5-Year Follow-Up by Mila Scheinberg, Thomas Sanchez, Turner Sankey, Meghan Underwood, Matthew Young, Rishi Earla, Swapnil Singh and Ashish Shah in Foot & Ankle Orthopaedics
Footnotes
Ethical approval
Ethical approval for this study was obtained from IRB-300000382 from the University of Alabama at Birmingham Institutional Review Board Federalwide Assurance #FWA00005960.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.