
Abstract
Background:
Bone fragments are often found in ankles with anterior bony impingement. However, whether they are detached osteophytes or accessory bones remains unknown.
Methods:
Among the 66 continuously enrolled cases of ankles with anterior bony impingement, 32 had a fragment located at the anterior margin of the tibia. The cases of posterior impingement, lateral instability, osteochondral lesions, or free bodies simultaneously treated were excluded. The enrolled subjects were classified into 2 groups: ankles without (group A) and with remarkable spurs (group B). The patients’ backgrounds, location of the fragments, clinical scores, and other parameters required to resume sports were compared. The Japanese Society for Surgery of the Foot (JSSF) ankle rating scale was used to evaluate preoperative and postoperative ankle conditions, and the Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was used to evaluate postoperative sports abilities.
Results:
Eight (seven subjects) and 11 ankles were classified into groups A and B, respectively, and the mean age of the 18 patients was 25.4 (range, 16-37) years. No statistical differences in patient backgrounds or fragment sizes between the groups existed. In group A, the fragments were located on the lateral plateau in 7 of the 8 ankles, whereas in group B, their locations varied. The patients were followed up for a median of 48 months (range, 24-168). No complications were observed. The postoperative JSSF and SAFE-Q sports activity scores were significantly higher in group A than in group B (P <.01 and <.001, respectively). The postoperative term to return to their original sports activities was significantly shorter in group A (P < .05).
Conclusion:
Anterior bony fragments of the ankle without a remarkable spur were located at a specific site, and the results of arthroscopic treatment were better than in those with remarkable spurs. Such a fragment may be called an os talotibiale.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Anterior bony impingement (ABI) of the ankle was first reported in 1947 in an athlete’s ankle by Morris. 14 It was also called the footballer’s ankle or impingement exostosis in the 1950s and has been well established as a cause of chronic ankle pain.12,18 Typical ABI of the ankle is characterized by a restricted range of sagittal motion of the ankle because of a large bone spur of the tibia and/or talus visible on routine lateral radiography.2,3,7,20 Three-dimensional computed tomography (3DCT) is an excellent tool to realize the precise morphology of these spurs with accompanied spur fragmentation or free bodies.3,19,21 Small bone fragments are usually ignored as they do not cause symptoms unless they are free bodies in the joint. However, in our experience, some fragments other than a free body causes symptoms, even if the spur is not distinctive or remarkable.
The os talotibiale is a rare accessory bone located in the front of the tibiotalar joint. Tsuruta et al reported that the os talotibiale was radiographically incident in 16 (0.5%) of 3460 feet, which could include detached osteophytes of the tibia. 23 Furthermore, Candan et al found no cases of os talotibiale in 1651 feet. 5 Spur formation of the ankle with fragmentation is common in athletes. The fragmentation is usually observed in ankles with remarkable spurs; however, some ankles have a symptomatic ossicle in front of the joint without spurs. Keles-Celic suggested the possibility of ABI of the ankle caused by the os talotibiale, although there is insufficient knowledge in present literature on the differentiation of the os talotibiale and spur fragmentation. 9
We report a cohort of patients who complained of anterior ankle impingement because of a small ossicle without a remarkable spur compared with those accompanying typical distinctive spurs.
Materials and Methods
This retrospective cohort study was approved by the medical research committee of our hospital. Comprehensive agreement for the academic use of information on treatment progress or any other data acquired during treatment was obtained from the patients by the hospital at the time of hospitalization.
From June 2006 to December 2021, a total of 66 ankles of 64 consecutive patients who underwent arthroscopic treatment at our hospital based on symptoms of anterior ankle impingement were enrolled for this study. Exclusion criteria were soft tissue impingement or a free body revealed by arthroscopy, osteoarthritic changes with narrowing of the joint space, ankle without a spur fragmentation or an ossicle in front of the joint, and incomplete records. Patients who were treated simultaneously of osteochondral lesions or ligament injuries treated simultaneously were also excluded (Figure 1).

Flow diagram of patients meeting study inclusion criteria.
Preoperatively, the demographic data of the patients, including age, sex, passive range of dorsiflexion of the ankle with the knee flexed, and ankle imaging findings were recorded. The ankle and hindfoot clinical rating scale of the Japanese Society for Surgery of the Foot (JSSF) was used to compare the pre- and postoperative clinical status of the patients. A Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was used to evaluate postoperative ankle conditions during sports activities.15 -17 The patients were divided in to 2 groups according to the classification of Scranton and McDermott: patients without remarkable spurs in the ankle (no spurs or type I spurs; group A) and those with remarkable spurs (types II-IV; group B). 20 Collected data of the ankles were compared between the groups.
Evaluation of Imaging
The stage of the anterior bony spur was evaluated on the lateral ankle view of computed radiography (CR) using the classification of Scranton and McDermott. An ankle without a spur other than a fragment or ossicle was classified as type 0 (Figure 2). Spur fragmentation or the presence of an ossicle in front of the ankle was evaluated using computed tomography (CT) consisting of sagittal, coronal, axial, and 3-dimensional (3D) view. The widths, lengths, and heights of the fragments or ossicles were measured on CT views. The location of the fragment or ossicle was classified into 5 zones: medial shoulder, medial plateau, central plateau, lateral plateau, and lateral shoulder (Figure 3). Magnetic resonance imaging (MRI) was performed when the ankle was suspected to have an osteochondral lesion.

Classification of the anterior bony spur by Scranton and McDermott (type I–type IV). The ankle without spurs was rated as type 0 in this study.
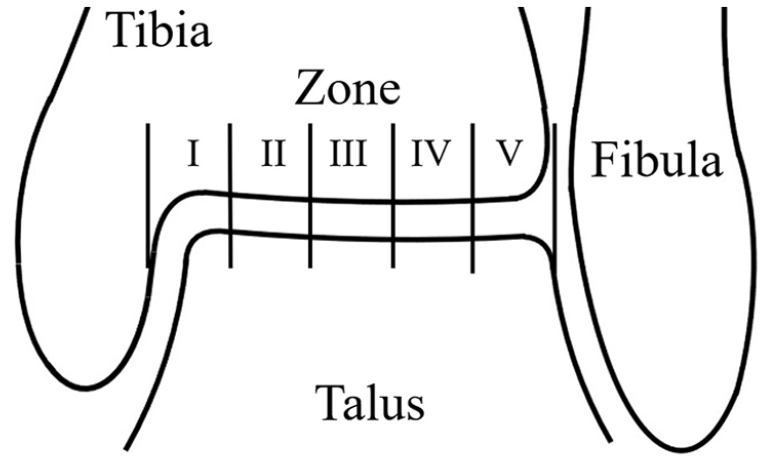
Five zones of anterior margin of the tibia. Zone 1, medial shoulder; zone 2, medial plateau; zone 3, central plateau; zone 4, lateral plateau; and zone 5, lateral shoulder.
Arthroscopic Treatment
The ankle arthroscopy was performed under general anesthesia with the patient in a supine position, and a traction device was used. A 2.7-mm-diameter 30-degree oblique scope was inserted through the medial portal, and another instrument was inserted through the lateral portal. The portals were changed as needed. An irrigation pump was used with an initial setting of 60 mm Hg pressure and 0.5 mL/s flow volume, and adjusted according to the bleeding. If control of bleeding was difficult by the pump, 0.5 mg of adrenaline was added to 3000 mL of perfusate or 250 mm Hg air pressure was applied to the tourniquet attached to the proximal thigh. The inflamed synovium and fibrous scars were removed, and the intraarticular structures were examined. The cartilage surface and marginal spurs were carefully probed to examine any chondral or osteochondral lesions and spur fragmentations. Spurs were removed using forceps or a motorized burr, and fragments were also removed.
Postoperative Course
Bulky dressings and compression bandages were applied to the ankles overnight. The next day, the bulky dressing was removed, hydrogel dressing and bandage were applied, and the patients were allowed to walk without crutches. Patients were allowed to jog 3 weeks after the operation and were followed at least for 24 months.
Statistical Analysis
Statistical analyses were performed using EZR software (ver. 1.61; Saitama Medical Center, Jichi Medical University, Saitama, Japan) using R version 4.2.2. 8 Patients’ age, BMI, fragment size, and the JSSF and SAFE-Q scores were assessed by the Mann-Whitney U test. The required terms to return to exercise and games were assessed by Welch’s t test. The patients’ sex, affected side, and fragment location were compared using Fisher exact test. P <.05 was considered statistically significant.
Results
The patient demographics are summarized in Table 1. Nineteen ankles from 18 patients with an ABI accompanying spur fragmentation were included in the analysis (Figure 1). All the patients were athletes, 12 were male and 6 female; the average age was 25.4 (range, 16-37) years. Seven patients with 8 ankles (4 ankles of type 0, 4 of type I) were classified into group A (Figure 4) and 11 patients (1 ankle of type II, 1 of type III, and 9 type IV) into group B (Figure 5). There were no statistically significant differences in age, sex, affected side, and BMI between groups.
Basic Demographic Data of the Patients

Abbreviation: IQR, interquartile range.
Mann-Whitney U test.
Fisher exact test.

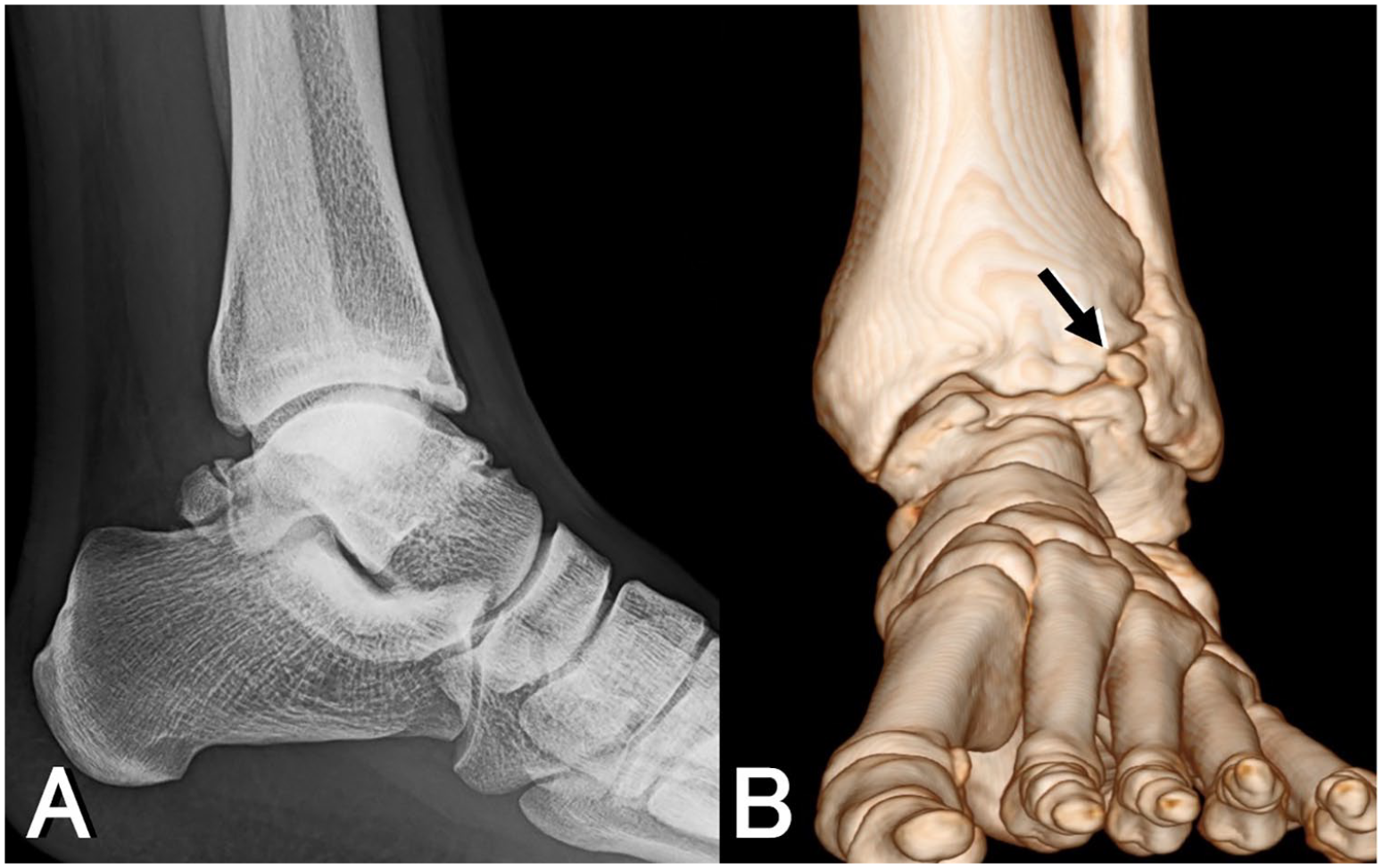
A 17-year-old high school girl who played kendo. (A) A fragment located lateral to the midline of the tibia without a socket (arrow) on 3D CT. (B) Arthroscopy showed that the fragment was covered with fibrous tissue, and loose union to the fibrous socket was observed by probing. (C) The fragment was removed.
A 26-year-old professional rugby player. (A) Type 4 spurs are shown on lateral ankle view. (B) A spur fragmentation at zone 5 (arrow) is shown on 3D CT.
The average size of the fragments was 7.3 (width) × 5.3 (length) × 4.8 (height) mm and the volume ranged from 51.6 to 655.8 mm 3 . There were no statistical differences in the volume of the fragments between the groups (Table 2). The fragments were located on the medial shoulder in 2 ankles, medial plateau in 3, central in 2, lateral plateau in 10, and lateral shoulder in 5. The fragments in group A were located on the lateral plateau in 7 of the 8 ankles (Figure 3), whereas those in group B were located across various areas. The differences in the locations of the fragments between the groups were statistically significant. Tram track lesions were observed by arthroscopy in 4 ankles in group A and 7 in group B. There were no statistically significant differences in the existing rates of tram track lesions between the groups.
Size and Location of the Fragments and Existence of Tram Track Lesion.

Abbreviation: IQR, interquartile range.
Mann-Whitney U test.
Fisher exact test.
The patients were followed up for a median of 48 months (range, 24-168). There were no complications such as delayed healing of the portals or sensory nerve disturbances. The postoperative condition of the patients is summarized in Table 3. The median preoperative JSSF scores were not significantly different between the groups; however, the scores improved significantly in both groups postoperatively (P < .001). The postoperative median JSSF and SAFE-Q sports activity subscale scores were significantly higher in group A than in group B (P < .01 and P < .001, respectively). The postoperative average term to return to sports activities was significantly faster in group A (exercises, P < .01; games, P < .05). The median ranges of ankle dorsiflexion change were not significantly different between the groups both pre- and postoperatively.
Comparison of JSSF and SAFE-Q Scores, Required Term to Return to Sports, and Range of Dorsiflexion of the Ankle.

Abbreviations: IQR, interquartile range; JSSF, The Japanese Society for Surgery of the Foot; SAFE-Q, Self-Administered Foot Evaluation Questionnaire.
Difference between pre- and postoperative values.
Mann-Whitney U test.
Welch t test.
Discussion
BAI of the ankle, known as ankle impingement exostosis, is a major ankle disorder that occurs in athletes. 4 Scranton and McDermott categorized impingement exostosis into 4 types according to its size and location on lateral radiographs: type I, osteophyte less than 3 mm; type II, osteophyte >3 mm; type III, anterior tibial osteophyte with secondary talar osteophyte (kissing lesion); and type IV, pan-talocrural osteoarthritic destruction. 20 In this classification, ankles with an osteochondral fragment are categorized as type IV with panarthritic changes.
In our cohort of patients, spur fragmentation was not always accompanied by large osteophytes or typical osteoarthritic changes when examined on the 3D CT. Instead, symptomatic ankles due to an ossicle in front of the joint were found, with no marginal spurs on either the tibia or talus. In our opinion, they seem to have the os talotibiale, an accessory bone, rather than spur fragmentation. These ossicles were situated on the midlateral portion of the anterior margin of the tibia, specifically in 7 of the 8 ankles without spurs, and were caught in a shallow dimple of the tibial margin.
If the origin of the fragments was a synovial osteochondroma (osteochondromatosis), it would be difficult to explain why the fragments landed at the apex of the anterior margin of the tibial plafond. Os talotibiale is a rare accessory bone located in the front of the tibial joint. Few studies have explained the nature of os talotibiale, it seems difficult to distinguish between a true accessory ossicle and an old nonunited fracture. The anterior tibial spur of the ankle generally arises from the lateral to midline portion of the tibiotalar joint. 3 It is likely that a fracture occurred in the young spur and did not heal completely because of the strenuous exercise, resulting in osteochondral fragments attached to the tibia via fibrous union in this area.
When an athlete complains of symptoms compatible with anterior ankle impingement syndrome (AAIS) without a large bone spur detected on radiographs, soft tissue impingement is usually suspected.1,6,10,11 However, a small ossicle in front of the joint, whether an accessory bone or a bone fragment of nonunion after osteophyte fracture, can contribute to AAIS, even in the absence of large spurs. In our series, a tram track rail lesion, one of the typical chondral lesions of ABI, was observed in half of the ankles without large spurs. 13 The occurrence rate of track rail lesions was not significantly different for the ankles with large spurs.
Anterior ankle symptoms affecting sports activities are stressful for competitive athletes. Although the lesions were subtle on radiographs, the symptoms were not as subtle in elite athletes. In our series, postoperative conditions were better in the ankles without spurs than in those with them, although the severity of the preoperative symptoms was not significantly different between the ankles with and without spurs. Patients without spurs also resumed their original activity in the shorter term after arthroscopic excision of the ossicle compared to patients with spurs. We believe that athletes with these lesions should not hesitate to undergo arthroscopic treatment.
The fragment is visible on routine lateral radiographs. However, physicians or radiologists may overlook this subtle lesion. In this cohort, 3D CT enabled us to recognize the location of the lesion and the relationship between the fragment and the tibia, including ball-and-socket–like interfaces. These images were helpful for understanding the pathology underlying the symptoms and explaining them to patients.19,21
Reports on the recurrence rate of osteophytes in AAIS vary, and studies with >5 years of follow-up have reported high recurrence rates.4,22,24 Recurrence of osteophytes does not always lead to relapse of AAIS symptoms, and long-term follow-up is preferred after surgery for AAIS. Among the patients in our cohort, 2 had a recurrence of symptoms: one without a spur 7 years postoperatively, and the other with a spur 2 years postoperatively who underwent reoperation.
The limitations of this study include the small sample size of each group. All patients were treated arthroscopically to minimize surgical invasions and an en bloc excision of the lesions was not performed. Histological analysis of specimens, including the interface between the ossicle and the tibia, may be helpful to distinguish accessory bones from spur fragmentations. However, we found no literature describing the os talotibiale in detail with histology other than the general occurrence rate on radiographs.
Conclusion
The so-called os talotibiale may be a fragmentation of a young tibial spur initiated at the specific area. The anterior bony fragments of the ankle without a remarkable spur were located at a specific site, and the results of arthroscopic resection of the fragments were better than in those with remarkable spurs. Such fragments without spurs may be what is known as an os talotibiale.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231224724 – Supplemental material for Anterior Ankle Impingement Syndrome With Spur Fragmentation: Is It an Os Talotibiale?
Supplemental material, sj-pdf-1-fao-10.1177_24730114231224724 for Anterior Ankle Impingement Syndrome With Spur Fragmentation: Is It an Os Talotibiale? by Kazuya Sugimoto, Shinji Isomoto, Tomohiro Matsui, Kazunori Tanaka, Kou Matsuyama, Akira Taniguchi and Yasuhito Tanaka in Foot & Ankle Orthopaedics
Footnotes
Author Note
This study was performed at the Nara Prefecture General Medical Center and the Imperial Gift Saiseikai Nara Hospital.
Ethical approval
This study was performed in accordance with the ethical standard in the 1964 Declaration of Helsinki. Comprehensive agreement for academic use of information on treatment progress or any other data acquired during their treatments was obtained from all the patients by the hospital at the time of their hospitalization. Details that might disclose the identity of the subjects under study have been omitted. This study was approved by the IRB of Nara Prefecture General Medical Center (IRB ID: 368).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.