
Abstract
Background:
The posterior malleolus component of the trimalleolar ankle fracture has posed a controversial topic for diagnostic imaging and surgical management. Preoperative computed tomography (CT) scans are used to better appreciate fracture morphology and may affect management techniques. No prior study has investigated the trend in preoperative CT scan use and the rates of posterior and syndesmotic fixation for trimalleolar injuries.
Methods:
This retrospective cohort study evaluated the use of preoperative CT scans and the rates of posterior and syndesmotic fixation for trimalleolar ankle fractures over a 10-year period at an adult level 1 trauma center. Patients surgically managed for ankle fractures with OTA/AO classifications of 44B3, 44C3.3, 44C1.3, 44C2.3, and 44A3 were identified and included using Current Procedural Terminology codes and a prospectively collected fracture registry. Demographic information, comorbidities, fixation methods, and use of preoperative CT scan were recorded. Comparative analyses were performed to assess for yearly differences in demographic characteristics along with changes in trends of preoperative CT scans and posterior and syndesmotic fixation.
Results:
A total of 1191 patients were included in the analyses. OTA/AO 44B3.2 fractures were the most common injuries (yearly range of 59.4%-80.1%). The rate of posterior fixation did not significantly increase during the study interval (1.4% growth per year [95% CI −0.27, 3.07]). However, the rate of preoperative CT scan use significantly increased by 2.76% (95% CI 1.99, 3.52) per year and the rate of syndesmotic fixation increased by 2.58% (95% CI 1.17, 3.99) per year. Fixation methods for both the syndesmosis and posterior malleolus changed during the study timeline.
Conclusion:
Despite a relatively stable rate of posterior fixation, the frequency of preoperative CT scans and use of syndesmotic fixation increased significantly over a 10-year study period.
Level of Evidence:
Level IV, descriptive pilot study.
Introduction
Trimalleolar ankle fractures are frequently encountered by orthopaedic surgeons involved with routine fracture care.24,32 The posterior malleolus component of the trimalleolar ankle fracture has posed a controversial topic for diagnostic imaging and surgical management. Since at least 1990, studies have shown that the posterior malleolus component of these fracture patterns cannot be fully characterized from radiographs, and are frequently underestimated.3,7,16,20,30 Further studies support the recommendation to obtain computed tomography (CT) scans for trimalleolar ankle fractures.1,15,22 CT scans can be used to assess both size and morphology of posterior malleolus fractures and to visualize other fracture features, such as joint impaction, incarcerated bone fragments, and incisura anatomy.25,30 The size of an articular fragment, joint impaction, and syndesmosis stabilization are some of the indications to fix a posterior malleolus fracture.8,9,28 Furthermore, recent literature suggests greater syndesmotic stability with posterior fixation rather than a more traditional primary syndesmotic approach.1,6,8,9
There is evidence from survey studies suggesting that some surgeons retrospectively change their initial preoperative plan for trimalleolar fractures after obtaining an additional CT scan.2,5,16,26,31 In addition, nearly 25% of Orthopaedic Trauma Association (OTA) members polled reported that they changed their operative plan to include posterior fixation according to the results of a CT scan. 10 However, there is no direct evidence on the rate at which operative changes are implemented as a result of CT scan review, or analysis of how management trends have changed over time. We evaluated the trend of preoperative CT scans, posterior fixation, and syndesmotic fixation for trimalleolar ankle fracture over a 10-year period at a university-affiliated level 1 trauma center. This investigation serves as a pilot study for an ongoing retrospective multicenter cohort study evaluating changing management philosophies and postoperative implications in trimalleolar fractures. We hypothesized that CT scan use would increase over time in response to recommendations in prior publications, but posterior and syndesmotic fixation treatments would not change significantly given a tendency for surgeons to maintain practice patterns despite constantly evolving evidence.
Methods
Study Design and Patient Population
The study was approved by the institutional review board. Medical records at a single university-affiliated adult level 1 trauma center were searched for Current Procedural Terminology codes 27822 and 27823 between January 1, 2011, and January 1, 2021. A prospective fracture data registry was used to identify patients surgically managed with trimalleolar fractures. Preoperative ankle radiographs were reviewed to confirm patients had the fracture patterns of interest (OTA/AO classifications 44B3, 44C3.3, 44C1.3, 44C2.3, and 44A3). Exclusion criteria were pathologic fractures, incomplete medical records, incomplete radiographs, nonunion/malunion reconstructions, periimplant fractures, and fixation revisions.
Data Collection
Medical records were reviewed for demographic information, comorbidities, surgical details, and whether a preoperative CT scan was obtained. Postoperative radiographs and operative notes were reviewed to determine if posterior and/or syndesmotic fixation were used. The type of fixation for both the syndesmosis and posterior malleolus—either independent screw(s), suture device, plate-and-screw construct, or combined—was recorded.
Statistical Analysis
Patients were grouped according to the year of their surgical procedure, and demographic and clinical characteristics were compared. A Kruskal-Wallis test was used to analyze continuous data, and a χ2 test was used to analyze categorical data. Because there were 10 groups (1 for each year, corresponding to 46 pairs of comparisons), Bonferroni corrections were used, and a P value of <.001 was considered statistically significant for year-by-year comparisons. The incidence rates of CT scans, posterior fixations, and syndesmotic fixations were calculated for each year by dividing the number of CT scans, posterior fixations, and syndesmotic fixations by the total number of surgeries that year and converting that to a percentage. A linear regression was used to assess associations between year of surgical procedure and rates of CT scans, posterior fixations, and syndesmotic fixations. For this analysis, the y-axis intercept was determined, and no Bonferroni correction was performed. Lastly, the hazard ratio (with 95% CIs) for having a posterior and syndesmotic fixation if a CT scan was performed was calculated for each year. All analyses were performed using SPSS, version 28. 29
Results
A total of 1223 patients were identified with a Current Procedural Terminology code of 27822 or 27823 between the years of 2011 and 2020 from our institution’s fracture registry. After exclusion criteria were applied, data from 1191 eligible patients were included in the analysis (Figure 1). The only difference in demographics and comorbidities after correcting for multiple comparisons was a higher rate of alcohol consumption among patients in 2016 to 2020 than in those in 2011 to 2015 (Table 1).

Tree digaram of selected patient cohort.
Patient Demographics and Comorbidities by Year.

Boldface indicates significance (P < .001).
The proportions of fractures in different classifications each year are shown in Table 2. The rate of dislocations was highest in 2013, but this was not statistically significant after correcting for multiple comparisons.
Clinical Characteristics of Patients by Year.

The rates of posterior fixations, syndesmotic fixations, and CT scans ordered every year are shown in Figure 2. Linear regression analyses were performed to estimate the rates of posterior fixations, syndesmotic fixations, and CT scans using the year as a covariate (Table 3). The rates of CT scans and syndesmotic fixations, but not posterior fixations, were positively associated with later years of the study period.

Yearly rates of CT scan use and syndesmotic and posterior fixation.
Summary of Results From Linear Regression.

Abbreviation: CT, computed tomography.
Boldface indicates significance (P < .001).
We also calculated the hazard ratios at each year of the study period for receiving posterior fixation or syndesmotic fixation if a CT scan was performed. Patients who had a CT scan were significantly more likely to have a posterior fixation than those without CT scans in each year of the study period (HRs ranged from 2.19 to 13.80) (Table 4). However, the likelihood of syndesmotic fixation among patients who had a CT scan was only significantly higher than that among those who did not have a CT in the earlier years of the study period, with hazard ratios declining each year so that there was no significant association in 2019 and 2020 (or 2015 and 2018 when correcting for multiple comparisons).
Hazard Ratios by Year for Fixation if CT Scan Was Performed

Boldface indicates significance (P < .001).
The yearly fixation techniques for both posterior and syndesmotic methods proportionally changed throughout our study timeline in a progressive and more rapid manner, respectively (Figures 3 and 4). Despite large fluctuations in posterior fixation technique between the years of 2015 and 2017, our data demonstrate an increasing use of plate-and-screw constructs (Figure 3). In contrast, the data show a rapid growth of suture device use over the last year of the study timeline, despite a preceding period of proportional consistency (Figure 4).

Method of posterior fixation per year.
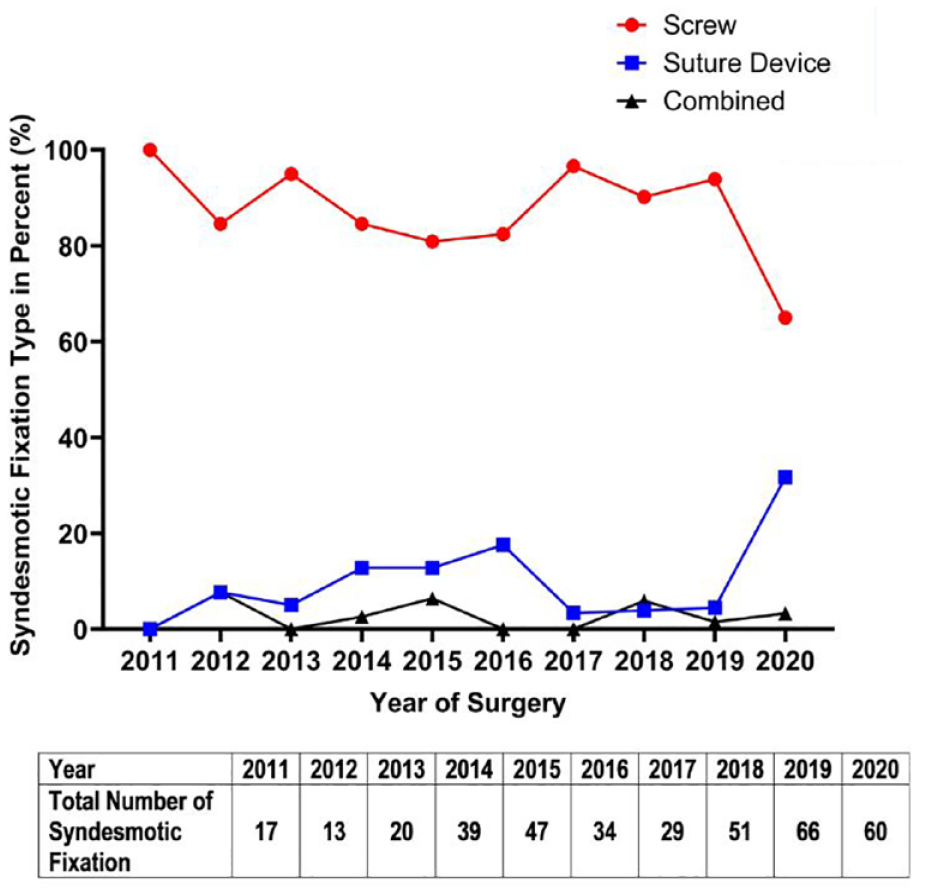
Method of syndesmotic fixation per year.
Discussion
We investigated the change in trends of preoperative CT scans and use of posterior and syndesmotic fixation in operatively managed trimalleolar ankle fractures at a level 1 trauma center over a 10-year period. This pilot study presents descriptive fracture and population characteristics along with managements trends for an ongoing multicenter retrospective study evaluating evolving management philosophies for trimalleolar injuries and their postoperative implications. Our data partially support our hypothesis, demonstrating a consistent growth in preoperative CT scans with a relatively stable rate of posterior fixation during this period. We believe that the increase in preoperative CT scans is influenced by the increasing amount of literature concerning the importance of the posterior malleolus and syndesmotic stability.3,7-9,15,28,30 Additionally, advancements in technology have substantially broadened the application of CT imaging, increasing its use in all orthopaedic subspecialties. 11 Although the relationship between advanced imaging and management trends have been explored in other orthopaedic disciplines, ours is the first study of this design to evaluate this relationship with respect to trimalleolar fractures.
Our study design closely parallels that by Lumsdaine et al, 19 who documented a relationship between CT scans and upper extremity periarticular fractures in a retrospective study at a level 1 trauma center. In contrast to our findings, they found a relatively stable rate of CT scans over a 5-year period but with a statistically significant increase in operative interventions. 19 Several other studies have more directly investigated the role of CT scans in operative management, typically with comparative analyses of proposed treatment strategies with and without the added benefit of advanced imaging.2,13,14,16,18,33,34 Despite most of these studies demonstrating changes in operative plans on reviewing imaging, none have provided a prospective analysis or evaluated practice adaptations in real time.
The yearly demographic and fracture characteristics of our study population were relatively consistent and align with those in prior literature.12,21,27 The only significant difference during the 10-year period was in reported alcohol use, but we do not believe that patient alcohol consumption influenced preoperative CT scan use or posterior fixation rates. In our study cohort, open injuries and dislocations represented 3% to 13% and 46% to 73%, respectively, of the yearly operative trimalleolar fractures. These are consistent with previous findings from the few studies detailing the rates of these injury types.12,21,27 A large epidemiologic study of foot and ankle fractures in the United States by Shibuya et al 27 found that 11.5% of trimalleolar fractures were open injuries. Dislocation rates for trimalleolar injuries were 48.4% (15 of 31) in a retrospective review by Hong et al 12 and 53.5% (15 of 28) in a prospective analysis performed by Martin et al. 21
Our data demonstrate that despite a consistent rate of posterior fixation (1.4% growth per year [95% CI −0.27, 3.07]), the rate of preoperative CT scan use significantly increasing by 2.76% (95% CI 1.99, 3.52) per year. The rate of posterior fixation is similar to rates from other smaller retrospective reviews of ankle fractures involving the posterior malleolus: De Vries et al 4 demonstrated a posterior fixation rate of 24.4% (11 of 45) and Langenhuijsen et al 17 reported a similar rate of 26.4% (14 of 53). However, the rate of syndesmotic fixation was also increasing by 2.58% (95% CI 1.17, 3.99) per year during the study interval. We believe that the substantial impact syndesmotic stability has on postoperative outcomes and the increasing popularity of suture devices lowered the threshold to opt for syndesmotic fixation.6,23 This trend toward suture devices is demonstrated in our data, with a rapid increase in use during the final year of the study period (Figure 4). In addition, the growing emphasis on the contribution of posterior malleolus fractures to syndesmotic stability may have influenced surgeons to use syndesmotic fixation rather than conservative management in cases with smaller posterior fragments.3,7-9,15,28,30 We also believe this emphasis influenced surgeons to more readily utilize plate-and-screw constructs for posterior fixation rather than independent screw(s) given the inherent superior stability and rotational control (Figure 3).
This investigation has several limitations, primarily stemming from surgeon-specific bias. The use of posterior fixation was much more frequent in 2017, possibly reflecting the addition of a new orthopaedic traumatologist to the faculty who may have influenced management algorithms used by existing surgeons. However, despite this addition, there were no further fluctuations in the faculty during the study period. All trauma faculty contributing to these data completed residency and/or fellowship training at our institution, producing relatively consistent management philosophies and algorithms. Furthermore, our institution does not require a preoperative CT scan for the management of trimalleolar fractures. We cannot provide the true indication for each CT scan obtained or the indications for surgical decision making. Although this analysis would be useful, the retrospective nature of this study prohibits such data collection. The decision to order advanced imaging can come from emergency medicine providers, orthopaedic surgery residents, midlevel providers, and faculty. We recognize the differences in management preferences and algorithms among the trauma faculty, which impacts how these injuries are treated at our institution. We feel this is a typical scenario in many centers, and the relatively large sample size over the span of 10 years provides an accurate assessment of practice changes.
Conclusion
Despite the increase in preoperative CT scans, the frequency of posterior fixation for trimalleolar fractures remained relatively constant at our level 1 trauma center over the 10-year study period. By contrast, syndesmotic fixation became more frequent, possibly because of the growing knowledge of its importance in postoperative outcomes and the popularity of flexible suture devices. This descriptive pilot study provides new baseline information regarding these trends and will serve as a foundation for further investigations regarding indications for syndesmotic and posterior fixation over time and the effect on surgical outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231216984 – Supplemental material for Computed Tomography Scans and Fixation Rates for Trimalleolar Ankle Fractures Over 10 Years at a Level 1 Trauma Center
Supplemental material, sj-pdf-1-fao-10.1177_24730114231216984 for Computed Tomography Scans and Fixation Rates for Trimalleolar Ankle Fractures Over 10 Years at a Level 1 Trauma Center by Joseph Kocan, Elias Joseph, Paul Mercado, Mohammad N. Haider, Sonja Pavlesen and Bernard Rohrbacher in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study has been approved by the University at Buffalo Institutional Review Board; Study ID STUDY00006258
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.