
Abstract
Background:
Metatarsalgia and plantar plate tears are characterized by forefoot pain and toe deformity in severe cases. Conservative management may slow progression of symptoms; however, definitive treatment often requires operative intervention. The purpose of this observational study was to evaluate the combination of plantar condylectomy and surgical imbrication of the plantar plate to the metatarsal neck to repair grade 0 plantar plate injuries.
Methods:
We retrospectively identified 22 patients with metatarsalgia and low-grade plantar plate lesions (grade 0), operated between 2018 and 2021, who underwent operative repair involving plantar metatarsal condylectomy and proximal surgical imbrication of the plantar plate to the metatarsal neck. Fourteen patients underwent concomitant hallux valgus correction. Data collection was performed preoperatively and postoperatively and included Patient-Reported Outcomes Measurement Information System (PROMIS) physical function (PF) and pain interference (PI) scores. Paired Wilcoxon signed-rank tests compared PROMIS PF and PI scores at patients’ preoperative, 6-9-week, 3-4-month, 5-6-month, and ≥9-month follow-up evaluations (P < .05).
Results:
Compared to their preoperative visit, patients demonstrated modest improvement in their PROMIS (pain and physical function) scores over the first ≥9 months postoperatively (median 13.0 months). Median preoperative and most recent PROMIS physical function scores were 40.5 (95% CI: 36-49) and 44.5 (95% CI: 40-52), respectively. Median PROMIS pain interference scores changed from 62.5 (95% CI: 56-67) to 56.0 (95% CI: 51-62). Improvement in pain and function was sustained in patients available for postoperative follow-up.
Conclusion:
In this small, early follow-up series, we found that plantar condylectomy and surgical imbrication of the plantar plate to the metatarsal neck was modestly helpful to treat metatarsalgia and grade 0 plantar plate injuries.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Plantar plate pathophysiology and associated metatarsophalangeal (MTP) joint instability have received increasing attention in orthopaedic literature. Composed of fibrocartilage and type I collagen, the plantar plate forms the plantar border of the MTP joint. 9 The plantar plate originates from the plantar surface of the metatarsal head, inserts into the plantar base of the proximal phalanx, and is further supported by the collateral ligaments, plantar fascia, flexor tendon sheath, transverse intermetatarsal ligament, and interosseous tendons.9,25 Multiple anatomic studies over the past several decades have illustrated the role of the plantar plate in static stabilization of the MTP joint, preventing toe subluxation/dislocation in the sagittal plane.5,13 Furthermore, the plantar plate absorbs compressive forces during weightbearing.9,28,29 This feature is illustrated by complaints of pain and sensation of “walking on marbles” in patients with plantar plate tears that compromise absorptive functioning.
Plantar plate tears are generally characterized by symptoms of forefoot pain and swelling and are associated with toe deformity in more advanced cases. The second toe is most affected, and deformities classically manifest as a dorsally displaced toe at the MTP joint. There may also be splaying between toes if the collateral ligaments are incompetent. 6 Hammertoes can also develop in the setting of chronic plantar plate insufficiency because of imbalance between the toe flexors and extensors. 19 Typically, pain is of gradual onset because of progressive attenuation of the plantar plate. However, tears have been reported with acute injury as well. Diagnoses of capsulitis, synovitis, metatarsal stress fracture, neuroma, inflammatory arthropathy, and degenerative joint disease can imitate this pain and should be considered while evaluating possible injury to the plantar plate. 2
The drawer test, described by Thompson and Hamilton, assesses MTP joint instability by applying dorsally directed force to a stabilized, neutral MTP joint. 30 The “paper pull-out test” has also been described as a reliable means of testing digital purchase, a function of joint position and strength. 3 Plain anteroposterior and lateral radiographs have been demonstrated as a useful tool for evaluating prodromal stages of MTP instability preceding subluxation by characterizing the angle of deformity, joint congruity, and increased lesser metatarsal length, an important contributor to MTP joint instability. 34 More recently, magnetic resonance imaging (MRI) has been demonstrated to have high sensitivity and specificity in identifying plantar plate lesions, particularly useful with high clinical suspicion for a plantar plate tear and an equivocal examination.22,33
Conservative treatment of lesser MTP instability, including the use of cushioned insoles, metatarsal padding, and adjacent toe taping, has been shown to relieve pain and slow progression of deformity in early stages.6,7 However, plantar plate tissue has poor regenerative properties, similar to those of knee menisci, and is unlikely to heal spontaneously.9,29 Nonsteroidal anti-inflammatory drugs (NSAIDs) and intra-articular corticosteroid injections may offer temporary symptomatic relief; however, surgical management may offer definitive improvement.8,23
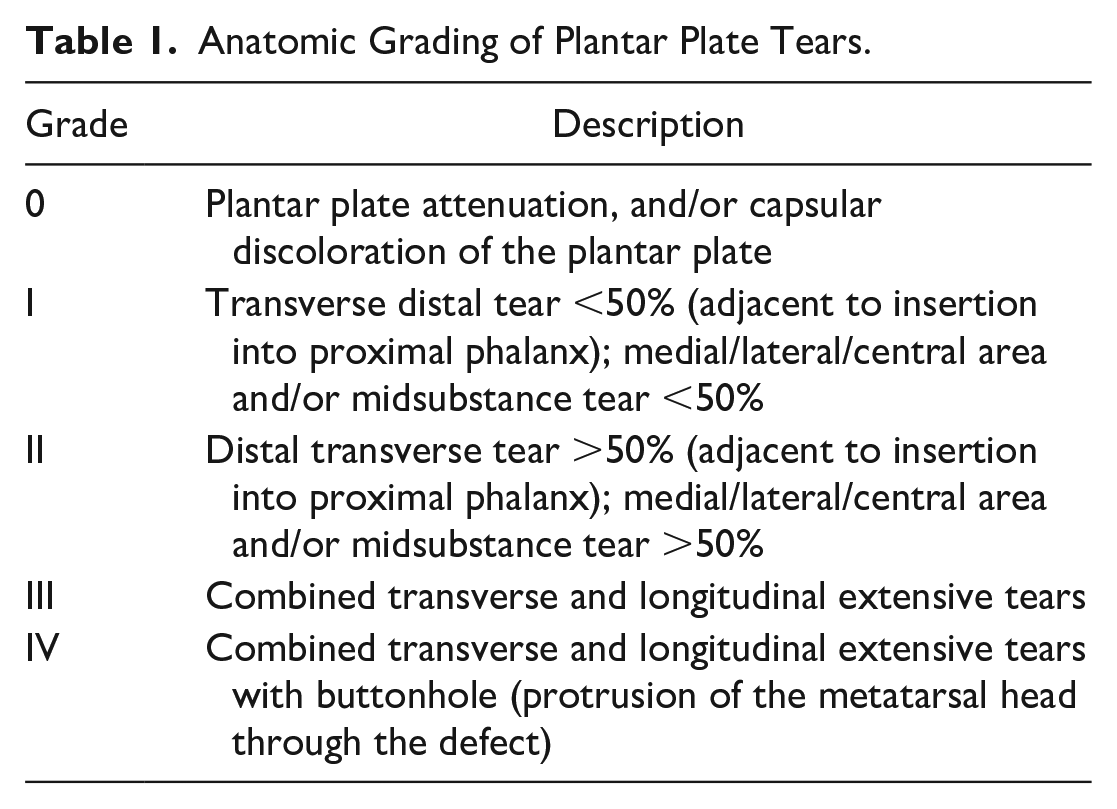
Through a series of plantar plate repairs, Nery and colleagues have proposed guidelines for clinical and surgical grading as well as subsequent management of plantar plate lesions (Table 1).8,20,21,23-25 Radiofrequency shrinkage with Weil osteotomy was described to treat grade 0 (plantar plate attenuation) and grade 1 (transverse distal or midsubstance <50%) lesions. Meanwhile, for grade 2 (transverse distal or midsubstance >50%) and grade 3 (transverse and/or longitudinal extensive) lesions, the authors advocated for direct plantar plate repair with reinsertion of the plantar plate to the proximal phalanx via a dorsal approach with Weil osteotomy. Grade 4 (buttonhole or combined transverse/longitudinal and degeneration) lesions were addressed via flexor-to-extensor tendon transfer due to irreparable plantar plate damage.7,18,20,22
Anatomic Grading of Plantar Plate Tears.
Although management of advanced plantar plate and collateral ligament lesions have been extensively reviewed in orthopaedic literature, the optimal treatment for grade 0 MTP joint instability lesions remains poorly understood. Grade 0 lesions are characterized by pain at the metatarsal head without a discrete tear or MTP deformity, 8 often leading to a delay in diagnosis due to their similarity in presentation to capsulitis or synovitis. Radiofrequency shrinkage, a joint stabilization technique applied in other orthopaedic disciplines with varying degrees of success, has been suggested by Nery and colleagues coupled with Weil osteotomy in the repair of grade 0 and 1 plantar plate lesions. 24 However, 2-year follow-up of patients treated with this approach demonstrated that grade 1 tears actually had a lower percentage of toe purchase, ground touch, and stability when compared to more advanced grade 2 tears, which were managed with direct plantar plate repair rather than radiofrequency shrinkage. Furthermore, complications associated with radiofrequency shrinkage have been cited in the literature including chondrolysis, biomechanical weakness, nerve damage, and recurrent instability.1,14–16,24,35 Surgical plantar plate repair coupled with Weil osteotomy has also demonstrated efficacy for a range of tear grades.4,11,12 Although this is a relatively safe osteotomy procedure, with exceedingly rare incidence of malunion, nonunion, or delayed union, this procedure has been associated with other complications including floating toe and transfer metatarsalgia. 17
The goal of this study was to characterize a novel approach to low-grade plantar plate lesions involving proximal surgical imbrication of the plantar plate to the metatarsal head. To this end, we sought to describe the radiographic changes and patient-reported outcomes in patients undergoing this procedure. Our novel technique serves as an efficacious alternative to radiofrequency shrinkage; however, the long-term consequences of both techniques remain uncertain.
Methods
This was an observational study of patients who underwent a novel technique for surgical repair of low-grade (grade 0) plantar plate lesions. Each subject gave informed consent to participate in this study, and the protocol was approved by the Institutional Review Board at the authors’ institution.
Patient records from a single fellowship-trained orthopaedic surgeon ranging from May 2018 to May 2021 were screened for potential subjects by electronic medical record review. Inclusion criteria were patients aged ≥18 years with grade 0 plantar plate lesions. Indications for the procedure included metatarsalgia with neutral MTP alignment, failure of nonoperative treatment (i.e., Budin splint, metatarsal pads, or avoiding barefoot walking), and pain and instability during a drawer test. MRI findings were considered when available. Plantar plate injuries were classified at the time of surgery based on size and location of the tear or lack of discrete tear for grade 0 lesions. These low-grade tears were treated via imbrication to the metatarsal neck. Patients found to have grade 1-4 tears were excluded from the study. Furthermore, patients without preoperative PROMIS scores were also excluded. PROMIS scores were obtained from 22 enrolled patients preoperatively to serve as a baseline and collected postoperatively at 1-6 months, 6-9 months, and ≥9 months from the date of surgery.
Surgical Technique
A dorsal incision is created over the pathologic MTP joint. A dorsal capsulectomy is performed to access the MTP joint. A McGlamry elevator is used to expose the plantar condyle and a plantar condylotomy is performed by resecting 2 mm from the plantar surface of the metatarsal head to provide a bleeding surface for ligament-to-bone healing. Pins are then placed into the dorsal metatarsal bone and proximal phalanx, and a pin distractor is used to visualize the plantar plate. A mattress suture is then passed through the plantar plate. To achieve this mattress stitch, suture is first placed through the eyelet of a Keith needle and then passed from dorsal to plantar though the plantar plate until the tip of the needle penetrates out of the plantar skin. Then, the eyelet of the needle with suture is redirected immediately after passing through the plantar plate and is pushed dorsally back through the plantar plate to create a mattress suture. Next, 2-mm Kirschner wires are used to make 2 bone tunnels through the metatarsal neck. A suture passer is used to guide the suture limbs from the plantar surface to the dorsal surface of the metatarsal (Figure 1). Finally, the suture is tied with the toe held in 20 degrees of plantar flexion.

Surgical technique. Photographs demonstrate (A) exposure of the metatarsal head, (B) visualization of the plantar plate to confirm lack of a discrete tear, and (C
Postoperatively, the patient is weightbearing as tolerated with the toe bandaged for 3 weeks. The patient is instructed to avoid forceful dorsiflexion for 6 weeks.
Statistical Analysis
Statistical analyses were preformed to compare preoperative and postoperative PROMIS scores and plain radiographs. Paired Wilcoxon signed-rank tests compared (1) preoperative and postoperative PROMIS pain interference and physical function scores at patients’ 6-9-week, 3-4-month, 5-6-month, and most recent (9-44-month) follow-ups; and (2) pre- and postoperative congruence of the second through fourth MTP joints at their 6-week and most recent (3-10-month) radiographs (P < .05). Univariate linear regressions compared changes in PROMIS scores to numerical patient characteristics such as BMI and age at the time of surgery (P < .05). Finally, Mann-Whitney U tests compared changes in PROMIS scores as a function of gender, mood disorders, preoperative opioid use, wound complications, and concomitant dislocation (P < .05). Nonparametric descriptive and comparative statistics were applied throughout due to n <30.
Results
Patient Characteristics
Twenty-two patients met inclusion criteria and were included in the final analysis. The median age of participants at the time of their procedure was 61 years (range: 30-74 years), and 18 subjects were female (Table 2). The median time to the most recent PROMIS score was 13.0 months (95% CI: 12.0-20.0). Fourteen of 22 patients underwent concomitant surgical treatment of hallux valgus deformity at the time of surgery.
Cohort Demographics and Preoperative Measures.

Patient-Reported Outcomes
Compared with their preoperative visit, patients demonstrated improvement in their PROMIS scores over the first 9 months postoperatively (median 13.0 months). Median preoperative and ≥9-month postoperative PROMIS physical function scores were 40.5 (95% CI: 36-49) and 44.5 (95% CI: 40-52), respectively, with a median increase of 4.0 points (95% CI: 0-6) (P = .032) (Figure 2). Median PROMIS pain interference scores changed from 62.5 (95% CI: 56-67) to 56.0 (95% CI: 51-62), with a median decrease of 5 points (95% CI: 0-10) (P = .010) (Figure 2).

Change in PROMIS physical function (black) and pain interference (gray) scores at multiple postoperative time points relative to the preoperative score. Data points and whiskers represent medians and interquartile ranges. The final data points were measured at the most recent follow-up, which occurred at a median 13.0 months postoperatively (range: 9-44). *P < .05 compared to preoperative score.
A subgroup analysis of the 8 patients who did not undergo concomitant hallux valgus repair showed median preoperative and ≥9-month postoperative PROMIS physical function scores of 40.5 (95% CI: 32-52) and 45.0 (95% CI: 36-56), respectively, with a median increase of 3.0 points (95% CI: –8 to 15) (P = .338) (Figure S1, Supplemental Material). Median PROMIS pain interference scores changed from 63 (95% CI: 53-72) to 56.0 (95% CI: 50-72), with a median decrease of 6.0 points (95% CI: –12 to 17) (P = .297) (Figure S1, Supplemental Material). Of the 14 patients undergoing concomitant hallux valgus correction, 1 patient received a Lapidus, and the rest underwent distal procedures (Akin, chevron, etc.).

Change in PROMIS physical function (black) and pain interference (gray) scores multiple postoperative time points relative to the preoperative score in the 8 patients who did not undergo concomitant hallux valgus correction. Data points and whiskers represent medians and interquartile ranges. The final data points were measured at the most recent follow-up, which occurred at a median 13.0 months postoperatively (range: 9-44). *P < .05 compared to preoperative score (denoted by *).
We found no significant variation in PROMIS scores as a function of age at the time of surgery, BMI, preoperative opioid use, wound complications, concomitant dislocation, fibromyalgia, or mood disorder (all P > .11).
Discussion
Our goal was to begin to determine if treatment of low-grade plantar plate lesions with partial plantar condylectomy and proximal surgical imbrication of the plantar plate to the metatarsal head can help improve symptoms. Our results demonstrate this surgical technique to be a potentially viable approach to grade 0 plantar plate lesions with significant, albeit modest, measured improvements in physical function and pain. Our method may serve as a potential alternative to radiofrequency shrinkage, which has been shown to offer short-term stability to the MTP joint, but with unclear long-term consequences.
To our knowledge, a study by Nery and colleagues represents the only studied alternative approach to direct plantar plate repair using radiofrequency shrinkage for subtle MTP joint instability published to date, enrolling 19 patients (35 MTP joints) in the analysis. 24 This group demonstrated significant improvement in joint stability measured with the MTP drawer test, reporting 83% of postoperative MTP joints to be totally stable (grade 0) compared to 97% of preoperative joints showing <50% subluxable (grade 1) instability with an average follow-up time of 20 months. Furthermore, patients in this study showed significant improvement in toe purchase and elevation, as well as pain measured using a visual analog pain scale (VAS). 24
Despite these successful findings, Nery and colleagues acknowledged limitations including small sample size, absence of a control, a minimum follow-up period of 12 months, and controversial outcomes associated with electrothermal collagen shrinkage reported in the literature. Although some histologic studies suggest supraphysiologic temperatures induced with radiofrequency may activate wound healing, others have cited biomechanical weakness and susceptibility to capsular stretching as a consequence of collagen shortening.1,14,15,24,31,35 Radiofrequency shrinkage initially appears attractive in comparison to other commonly used techniques, because of being technically less challenging, and providing satisfactory short-term results with more favorable immediate postoperative pain scores. However, the long-term effects of radiofrequency shrinkage on tissue health have been less promising.15,31
Finney et al 10 described the blood supply to the plantar plate, demonstrating the microvasculature is densest at the proximal and distal attachments. Furthermore, torn plantar plates exhibit neovascularization around the site of the tear, suggesting that the plantar plate is a structure that attempts to heal after an insult. 27 Contemporary surgical techniques involve stripping the plantar plate from the metatarsal neck as well as cutting the plantar plate from the proximal phalanx, with subsequent repair of only the distal attachment. 32 These maneuvers may devascularize the plantar plate, and potentially contribute to the 17.4% to 25% residual floating toe deformity following repair of low-grade plantar plate lesions due to iatrogenic plantar plate insufficiency caused by stripping the proximal attachment of the plantar plate from the metatarsal head. 23 If the distal attachment of the plantar plate to the proximal phalanx is intact in the setting of a grade 0 tear, or largely intact in a grade 1 tear, we have imbricated proximally to the metatarsal neck to theoretically preserve its associated vascular contribution, as Park et al 26 have previously demonstrated that the majority of proximal blood supply originates from the metatarsal neck rather than plantar fascia.
Nery and colleagues have previously detailed repair of the plantar plate distally via reattachment of the plantar plate to the proximal phalanx for more severe grade 2 and grade 3 lesions.7,20 This procedure, although established in foot and ankle literature, continues to prove technically challenging even for experienced surgeons because of limited exposure and delicate anatomy.
Outcomes of many plantar plate repair approaches in conjunction with Weil osteotomy have been reported in recent years.4,11,12,32 Fleischer and colleagues compared an isolated second Weil metatarsal osteotomy to a Weil osteotomy plus plantar plate repair, demonstrating significantly improved FAOS scores and radiographic alignment at 1-year follow-up in the latter group. 11 Their findings suggest that repair and advancement of the plantar plate contributes to lesser MTP stability and subjective clinical improvement, regardless of tear grade. Importantly, surgical imbrication of the plantar plate to the metatarsal neck precludes a Weil osteotomy but still yields modestly improved PROMIS scores at ≥9 months.
Several limitations exist for our study including small sample size, minimum follow-up time of 9 months for final postoperative PROMIS scores, and a majority of the cohort undergoing concomitant surgical correction of hallux valgus deformity with no control group. Moreover, the improvements in PROMIS scores among patients who did not undergo concomitant hallux valgus correction were not statistically significant, suggesting that the improvement demonstrated by the broader cohort may have been driven in part by the hallux valgus correction. However, the effect size was comparable between this subgroup and the broader cohort, implying that this subgroup analysis may have been underpowered (n = 8). The amount of improvement measured on these scales are very close to the statistically determined minimal clinically important difference of 5 points, so the findings of this work should be interpreted with caution. Finally, the mechanism of pain relief in this study was unclear, given that the procedure simultaneously resolves lesser MTP instability and relieves pressure via plantar condylectomy.
Conclusion
Overall, these data present satisfactory, early patient-reported outcome measures following plantar condylectomy and surgical imbrication of plantar plate to metatarsal neck to treat metatarsalgia in the setting of grade 0 lesser toe metatarsophalangeal joint instability.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231213615 – Supplemental material for Early Outcomes Following Plantar Condylectomy and Imbrication of Plantar Plate to Metatarsal Neck for Metatarsalgia and Grade 0 Lesser Toe Metatarsophalangeal Joint Instability
Supplemental material, sj-pdf-1-fao-10.1177_24730114231213615 for Early Outcomes Following Plantar Condylectomy and Imbrication of Plantar Plate to Metatarsal Neck for Metatarsalgia and Grade 0 Lesser Toe Metatarsophalangeal Joint Instability by Robert N. Kent, Kempland C. Walley, Noah Saunders, Eric Colomb, Vandan Patel, James R. Holmes, David M. Walton and Paul G. Talusan in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from our institutional review board (HUM00180017)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.