
Abstract
Background:
Recovering normal hindfoot alignment and correcting deformity of the ankle joint following total ankle arthroplasty (TAA) in osteoarthritis (OA) is essential for improving clinical outcomes and increasing long-term survival. We aim to evaluate hindfoot alignment following standard TAA compared to TAA with a total talar prosthesis (“combined TAA”) in varus-type OA patients.
Methods:
This retrospective study was conducted between 2010 and 2022. We included 27 patients (30 feet) who underwent standard TAA and 19 patients (22 feet) who underwent combined TAA. Hindfoot alignment at the subtalar joint was measured by weightbearing subtalar radiographic view before and after surgery.
Results:
In the standard TAA, the angle between the tibial shaft axis and the articular surface of the talar dome joint (TTS) changed from 75 to 87 degrees (P < .01), the angle between the tibial axis and the surface on the middle facet (TMC) from 89 to 94 degrees (P < .01), and the angle between the tibial axis and the surface on the posterior facet (TPC) from 80 to 84 degrees (P < .01). The angle between the articular surface of the talar dome and the posterior facet of the calcaneus (SIA) decreased from 4.7 to −2.5 degrees (P < .01). In the combined TAA, TTS angle changed from 77 to 88 degrees (P < .01), TMC angle from 93 to 101 degrees (P < .01), TPC angle from 84 to 90 degrees (P < .05), and SIA from 6.6 to 2.1 degrees (P < .01). Varus deviation to the subtalar joint (TMC, TPC) significantly improved postoperatively in both groups. However, TPC was smaller than TTS and SIA was negative in standard TAA, and TPC was larger than TTS and SIA was positive in combined TAA.
Conclusion:
The amount of correction of the subtalar joint differed depending on the ligament dissection of the subtalar joint and shape of the talar component
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
In the early stages of varus-type osteoarthritis (OA), the subtalar joint adopts a valgus configuration to compensate.8,18,30 However, as OA progresses, the subtalar joint is unable to compensate, and it is impossible for both the talus and calcaneus to incline to the valgus position from stage 3b to stage 4. Recovering normal hindfoot alignment and correcting the deformity of the ankle joint following total ankle arthroplasty (TAA) are essential for improving clinical outcomes and increasing long-term survival.9,10 Good postoperative outcomes depend on prosthesis design, patient selection, and severity of preoperative deformity.7,17 Correct hindfoot alignment evaluation is essential, as uncorrected coronal alignment after TAA may give rise to instability and edge loading that wears the polyethylene insert, leading to premature implant failure.3,6,29,34,35 There is correlation between postoperative changes in varus tibiotalar surface angle and hindfoot alignment changes because of TAA and the predicted angle of hindfoot alignment that would be corrected by TAA. 29 However, this formula is only applicable to the normal subtalar joint, and there are limitations in the correction of hindfoot alignment with TAA. Hobson et al 9 reported the need for additional procedures, such as subtalar joint fusion and calcaneal osteotomy, in cases in which hindfoot alignment and internal rotation remained after correction of the ankle deformity with TAA.
Combined TAA is performed in cases of varus OA in which the talus is flattened and collapsed or in cases of large bone cysts that are at risk for implant sinking and subtalar joint OA. In recent years, favorable results have been reported following the use of a custom-made artificial talus, without subsidence or mismatch. 16 To produce an artificial talus, computed tomography (CT) data from the contralateral talus was obtained, and a 3-dimensional wire model was constructed using the data. 33 In the past, the evaluation of hindfoot alignment in TAA has recommended caution in cases of severe preoperative varus; however, this has not been reported in combined TAA.
The Cobey, long axial view, and hindfoot alignment view were used to evaluate the varus and valgus hindfoot by tilting the tibial and calcaneal axes.4,11,13,15,26,27 Weightbearing subtalar joint radiography is also used to evaluate hindfoot alignment.8,31 Because this radiographic procedure depicts the subtalar joint, it is possible to evaluate not only the relationship between the tibia and calcaneus but also the relationship between the talus and calcaneus.
By evaluating the changes in the subtalar joint in combined TAA, in which the ligaments are dissected and the talus is replaced, and comparing them to standard TAA, the potential for alignment correction with combined TAA may be anticipated to be potentially greater. This study aimed to evaluate and compare the changes in hindfoot alignment before and after standard TAA and combined TAA for varus-type OA using a weightbearing subtalar joint view.
Materials and Methods
We conducted a retrospective study of 144 patients with varus-type OA treated with TAA between 2010 and 2022. We included patients whose weightbearing subtalar joint view were obtained before surgery and at least 3 months after surgery. Standard TAA was performed in 27 patients (30 ankles), whereas combined TAA was performed in 19 patients (22 ankles). The cases were stage 3b (18 ankles) and stage 4 (34 ankles).30,32 Combined TAA was indicated in patients with severe flat talus, talar collapse, a large cyst in the talus, or subtalar joint OA. The combined TAA group included patients with medial OA complicated by flatfoot but not at stage 3a. Patients with rheumatoid arthritis, a history of periarticular ankle fractures, or any other concomitant foot deformities or the additional surgery (subtalar joint fusion and calcaneal osteotomy) at the same time were excluded. The TNK ankle (Kyocera, Kyoto, Japan) was used as the prosthesis in all cases. In standard TAA, a resurfacing component was used on the distal end of the tibia and dome of the talus, wheras in combined TAA, a resurfacing component was used on the tibia side and an artificial talus was inserted on the talus. The total talar prosthesis was custom-made based on the patients’ individual CT data (Kyocera). 16 To produce the artificial talus, CT data from the contralateral talus was obtained, and a 3-dimensional wire model was constructed using the data. Subsequently, a stereolithographic model was cast, and a total talar prosthesis was produced. 33
Surgical Technique
Patients were placed in the supine position, and the surgery was performed from the anterior ankle joint view. For standard TAA, cutting of the distal end of the tibia and body of the talus was performed to enable the insertion of the implant. A tibial component coated with calcium phosphate paste (Hoya, Tokyo, Japan) and bone marrow fluid was placed in the tibia, and the talus component was fixed with cement. In combined TAA, the distal end of the tibia is cut, and the talus was completely removed while splitting the bone with a bone saw. When the talus was cut, the connecting ligaments (the attachements of the deltoid ligament, the anterior and posterior talofibular ligaments, the cervical ligament, the interosseous talocalcaneal ligament, and the talonavicular) were dissected, and an artificial talus was inserted. On the tibial side, a component was placed, as in Standard TAA. After surgery, both groups were immobilized in a short-leg cast for 3 weeks. Partial weightbearing was allowed 2 weeks after surgery.
Subtalar Radiographic View
In the weightbearing subtalar radiographic view,10,27 an X-ray film cassette was placed in front of the foot perpendicular to the ground, and radiographs were obtained in the standing position with a 30-degree tilt from 100 cm behind the foot (Figure 1A). Radiographs depicting the articular surface of the talus and subtalar joints were obtained. Radiographic assessment included the angle between the tibial axis and the surface of the talar dome joint (TTS), the angle between the tibial axis and the surface of the middle facet (TMC), and the angle between the tibial axis and the surface of the posterior facet (TPC) from the weightbearing subtalar view. In addition, as an index of the inclination of the subtalar joint relative to the ankle (SIA), the angle between the articular surface of the talar dome and the posterior facet of the calcaneus was calculated using a numeric formula (Figure 1B). TTS, TMC, and TPC angles less than 90 degrees to the tibial axis indicate varus, and angles greater than 90 degrees to the tibial axis indicate valgus. A positive SIA value indicates valgus of the posterior facet relative to the talar dome joint, whereas a negative value indicates varus.
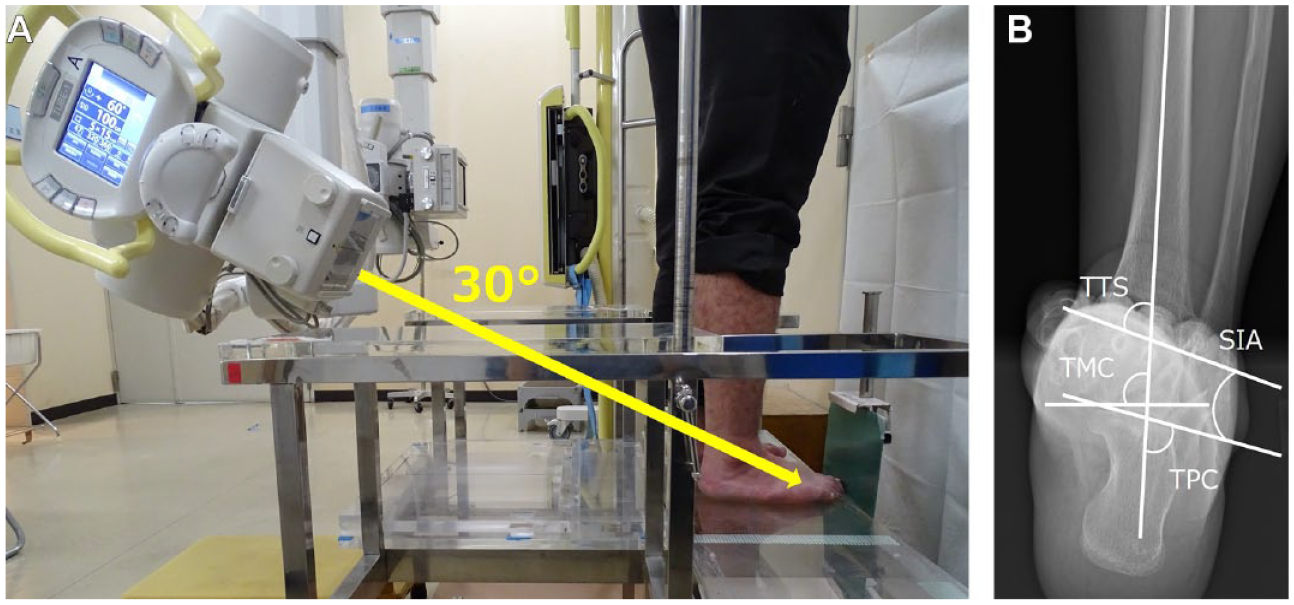
Weightbearing subtalar radiographic view. (A) The cassette is placed vertically on the floor in front of the patient and angled at 30 degrees from 1 m behind the patient. (B) Radiographic parameters. TTS angle, angle between the tibial axis and surface of the talar dome joint; TMC angle, the angle between the tibial axis and the surface on the middle facet; TPC angle, the angle between the tibial axis and the surface on the posterior facet; SIA (TPC-TTS), inclination of the calcaneus to the talus.
The angles between the tibial shaft and the articular surface of the distal tibia (TAS), the articular surface of the talar dome (TTA), and the angle of inclination of the talus to the tibial articular surface (TT) from the weightbearing ankle anteroposterior (AP) view were measured.
In addition to radiographic assessment, a clinical assessment was also performed. The Japanese Society for Surgery of the Foot (JSSF) ankle-hindfoot scale was used for subjective evaluation.21,22 This scale comprises 3 categories: pain, function, and alignment. The Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was used for objective assessment.23,24 This includes 5 subscales: “pain and pain related, physical functioning and daily living,” “social functioning,” and “shoe-related, general health, and well-being.” These clinical assessments were calculated based on those recorded at the last follow-up among the imaging-assessed cases.
Statistical Analysis
To evaluate the intraobserver agreement of the measurement technique, measurements of 10 randomly selected radiographs were repeated using the same reader (T.F.). For interobserver agreement, a third reader (Y.U.) repeated the measurements for the same 10 participants. Interobserver and intraobserver reliabilities for the parameters were assessed by estimating the intraclass correlation coefficients (ICCs) and 95% CIs using an ICC (2,1) modeling scheme.
Preoperative and postoperative radiographic and clinical assessments (JSSF and SAFE-Q) were compared between the groups using corresponding t tests. The Student t test was used to compare data between the groups. Statistical significance was set at P <.05. All statistical analyses was performed using EZR software (version 1.60; Japan). 12
Results
The interobserver and intraobserver reliabilities of the parameters of the 10 randomly selected participants for the weightbearing subtalar radiographic views were 0.771 (95% CI 0.239-0.944) and 0.985 (95% CI 0.939-0.996) for TTS, 0.851 (95% CI 0.494-0.964) and 0.966 (95% CI 0.867-0.992) for TMC, and 0.933 (95% CI 0.751-0.984) and 0.987 (95% CI 0.946-0.997) for TPC, respectively. The interobserver and intraobserver reliabilities of the parameters of the 10 randomly selected participants for the weightbearing ankle AP were 0.968 (95% CI 0.867-0.993) and 0.973 (95% CI 0.892-0.994) for TAS and 0.970 (95% CI 0.874-0.993) and 0.993 (95% CI 0.972-0.998) for TTS, respectively. These values indicated substantial agreement (ICC > 0.7).
The demographic details of patients in the 2 groups are listed in Table 1. In both groups, the TAS and TTA angles in the weightbearing ankle AP view changed significantly before and after surgery, and the varus improved (Tables 2 and 3). In the subtalar radiographic view, the TTS, TMC, and TPC angles changed significantly before and after surgery, and varus improved. The SIA from 4.7 to −2.5 degrees (P < .01) in the standard TAA group, whereas the SIA changed from 6.6 to 2.1 degrees (P < .01) in the combined TAA group, with significant differences found in both the ankle and subtalar joints in both groups (Tables 2 and 3).
Patient Demographics.
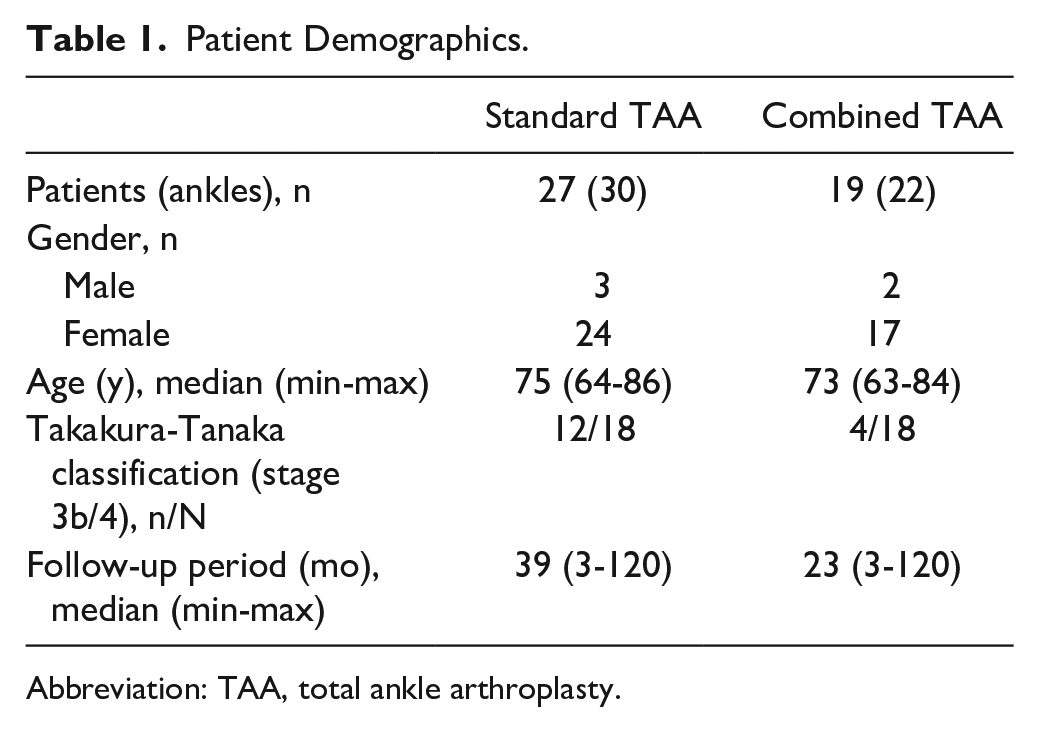
Abbreviation: TAA, total ankle arthroplasty.
Comparison of Preoperative Radiographic Parameters Between Standard TAA and Combined TAA.

Abbreviations: AP, anteroposterior; SIA (TPC-TTS), inclination of the calcaneus to the talus; TAA, total ankle arthroplasty; TMC angle, the angle between the tibial axis and the surface on the middle facet; TPC angle, the angle between the tibial axis and the surface on the posterior facet; TT angle, the angle of inclination of the talus to the tibial articular surface; TTA angle, the angle between the tibial axis and the articular surface of the talar dome; TTS angle, angle between the tibial axis and surface of the talar dome joint; TAS, the angle between the tibial shaft and the articular surface of the distal tibia.
Comparison of Postoperative Radiographic Parameters Between Standard TAA and Combined TAA.

Abbreviations: AP, anteroposterior; SIA (TPC-TTS), inclination of the calcaneus to the talus; TAA, total ankle arthroplasty; TMC angle, the angle between the tibial axis and the surface on the middle facet; TPC angle, the angle between the tibial axis and the surface on the posterior facet; TT angle, the angle of inclination of the talus to the tibial articular surface; TTA angle, the angle between the tibial axis and the articular surface of the talar dome; TTS angle, angle between the tibial axis and surface of the talar dome joint; TAS, the angle between the tibial shaft and the articular surface of the distal tibia.
Comparison of the standard TAA and combined TAA groups revealed no significant differences in ankle joint weightbearing from the ankle AP and subtalar views preoperatively; however, the TMC angle, TPC angle, and SIA were significantly larger in the combined group in the postoperative subtalar view (Table 3). The postoperative JSSF results were not significantly different overall, but the subcategory “function” was significantly higher in the Combined TAA group (P = .0478). Further, there were no significant differences in the postoperative SAFE-Q scores between the 2 groups. However, all the mean subscale scores were higher in the combined TAA group (Table 4). No complications requiring reoperation occurred in either group.
Comparison of Clinical Parameters Between Standard TAA and Combined TAA.
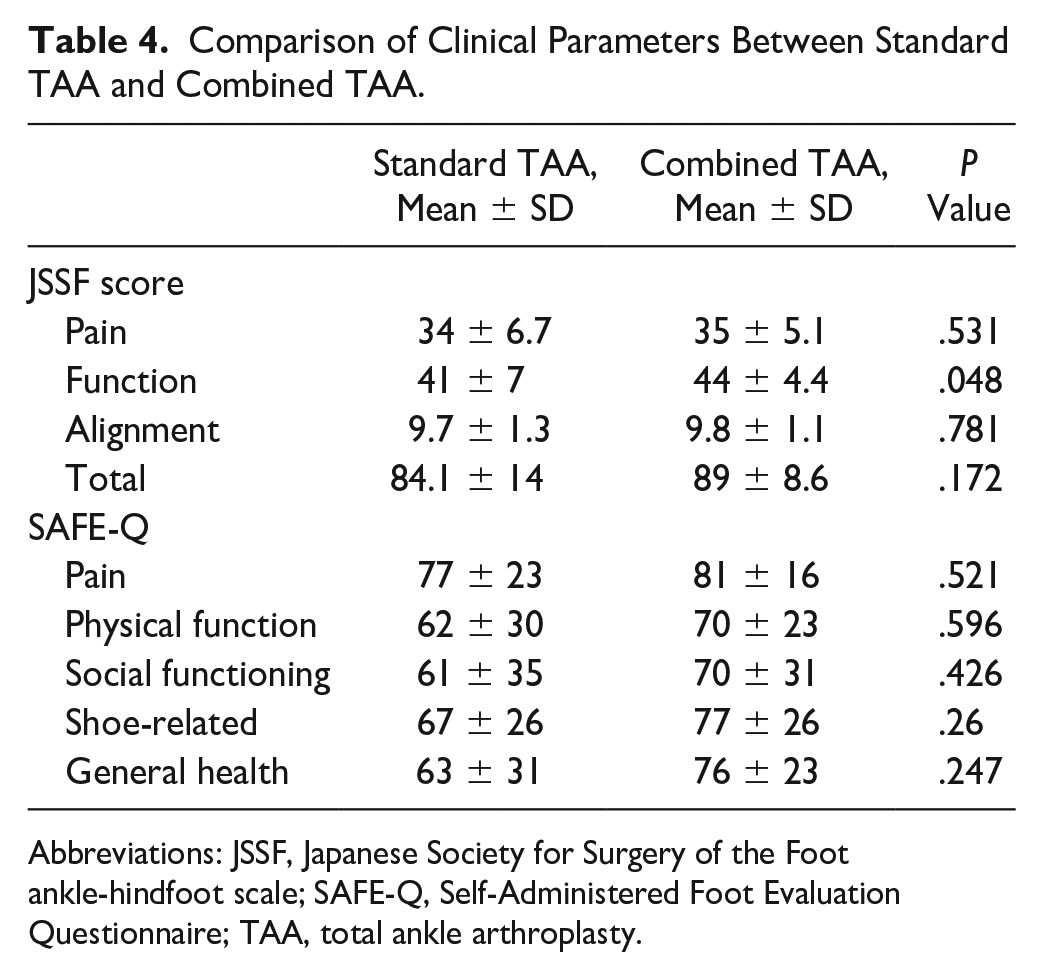
Abbreviations: JSSF, Japanese Society for Surgery of the Foot ankle-hindfoot scale; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAA, total ankle arthroplasty.
Discussion
Varus deviation of the ankle joint (TAS, TTA, and TTS) and the subtalar joint (TMC and TPC) in both groups significantly improved after surgery. However, the TPC was smaller than the TTS and the SIA was negative in the standard TAA group; in contrast, the TPC was larger than the TTS and the SIA was positive in the combined TAA group.
Previous methods for evaluating hindfoot alignment of TAA have reported the relationship between the tibial and calcaneal axes using the weightbearing ankle AP view or hindfoot alignment view.11,17,26,27 The weightbearing subtalar view is an imaging technique that can evaluate the inclination of the posterior facet of the calcaneus in relation to the articular surface of the talar dome; however, there have been no reports of its use in the subtalar views for TAA. The normal values for the subtalar view were 87 degrees for the TTS angle, 88 degrees for the TPC angle, and 1.5 degrees for the SIA, but the TTS angle (stage 3b: 70 degrees; stage 4: 82 degrees) and the TPC angle (stage 3b: 75 degrees; stage 4: 85 degrees) were smaller because of varus in stages 3b and 4. 8
The standard TAA corrected the TTS angle to normal; however, the TPC angle remained lower than normal, resulting in a negative SIA, which indicates the amount of correction at the subtalar joint. The amount of correction at the subtalar joint was small, whereas an adequate varus correction was achieved at the ankle joint. Standard TAA replaces only the articular surface of the talus; therefore, the subtalar joint is not treated. Consequently, although the hindfoot alignment to the tibia is improved, the degree of varus correction at the subtalar joint may be smaller than that at the ankle joint (Figure 2A).

Mechanism of correction of hindfoot alignment in Standard TAA and Combined TAA. (A) The degree of correction of the subtalar joint is smaller than that of the ankle joint because of the correction of the hindfoot alignment associated with the correction of the ankle joint. (B) Both the ankle and subtalar joints can be corrected by removing the interosseous talocalcaneal ligaments and the ligaments around the talus and inserting an artificial talus. TAA, total ankle arthroplasty.
Conversely, combined TAA also significantly improved the TTS and TPC angles, whereas the SIA was positive; collectively, the postoperative hindfoot alignment was close to normal. In combined TAA, an artificial talus is inserted after the interosseous talocalcaneal ligaments, and the ligaments surrounding the talus are transected. The interosseous talocalcaneal ligament contributes more to subtalar joint stability than the calcaneofibular ligament.1,20,29 We suggest that dissection of this interosseous complex, especially the interosseous talocalcaneal ligament, which is involved in eversion and pronation, will improve the varus calcaneal alignment of the calcaneus relative to the talus. Furthermore, the subtalar joint has an anterior compartment (coxa pedis) consisting of the anterior and articular surfaces of the talonavicular joint and the anterior and middle calcaneal facets, and a posterior compartment comprising the concave posterior-inferior talar facet and the large convex posterior calcaneal facet. The geometry and joint congruency of the subtalar joint determine the mobility and guidance of this motion.10,28 Because the artificial talus was custom-made to fit the shape of the joint surface of the affected ankle and subtalar joint, 33 it was thought that the artificial talus was not only a spacer but also conformed to the joint surface, resulting in alignment correction in both the ankle and subtalar joints (Figure 2B). The most common indication for TAA is end-stage ankle osteoarthritis (stage 3b or 4). It is important to understand the amount of subtalar joint change in TAA without subtalar joint procedures for end-stage ankle osteoarthritis without subtalar joint compensations to determine the need for subtalar joint procedures.
Normal hindfoot alignment was defined as a calcaneus of 0 to 5 degrees valgus, or 5 to 10 mm lateral to the tibial axis.2,19 Although our measurement method did not use the calcaneal axis, a small TPC angle and a negative SIA value also indicates that the hindfoot alignment is varus. In both groups, the preoperative TTS and TPC were small, but the SIA was positive. This indicates a strong internal rotation of the ankle joint resulting in a relative external rotation of the subtalar joint. Postoperatively, SIA increased as the ankle joint was corrected, and the degree of change in the subtalar joint determined the SIA value. Our results suggest that the hindfoot alignment was closer to normal in the compound TAA group than in the standard TAA group.
Frigg et al 5 previously reported that hindfoot alignment after TAA correlated with the physical function and role of the SF-36 using the hindfoot alignment view, and that hindfoot alignment correlated with the dynamic loading pattern during heel strike using plantar pressure measured by pedobarography. They further reported that normalization of the hindfoot alignment may improve the clinical outcomes and long-term survival of patients with TAA. Kurokawa et al 16 previously compared postoperative JSSF, Ankle Osteoarthritis Scale, and SAFE-Q scores between standard TAA and combined TAA, and reporting that postoperative JSSF was significantly higher and that all subscales of the postoperative SAFE-Q were higher, although not significantly, in Combined TAA, whereas clinical outcomes were also better. In the present study, we only found a significant difference in postoperative JSSF in the subscale; however, the improvement in function and SAFE-Q scores were similar to those previously reported.5,16 Nevertheless, it will be necessary to increase the number of cases to investigate this difference more thoroughly, as we have not yet demonstrated a significant difference. Normalization of the hindfoot alignment is important, and consideration should be given to whether soft tissue treatment (deltoid ligament release, lateral ligament reconstruction and posterior soft tissue releases) or subtalar joint fusion and calcaneal osteotomy should be added to standard TAA, or whether Combined TAA should be indicated for patients with end-stage OA with talar deformity or subtalar joint OA who require correction of internal rotation of the subtalar and ankle joints .
This study has several limitations. This study included a small number of cases, and the inclusion of cases at 3 months postoperatively may not have been sufficient to observe the loading capacity and final subtalar joint changes. Some patients had medial OA complicated by flatfoot. Some cases of varus ankle arthritis demonstrate valgus hindfoot alignment that is too significant to be explained as compensation for proximal deformities, implying the possibility of preexisting hindfoot valgus alignment before the development of varus ankle arthritis.18,25 This could explain why the preoperative and postoperative TPC angles and SIA were larger in the combined TAA group. Only 2-dimensional evaluation using radiographs was performed; TTS may not depict the complete articular surface of the talus because of the imaging technique of subtalar radiography; we did not consider whole-limb alignment or the influence of other joints that may affect alignment, such as the knee joint; and the results of this study do not prove that hindfoot alignment improved because it was not evaluated with traditional hindfoot alignment. Additionally, simultaneous rotation in the axial plane and translation in the sagittal plane may be present; therefore, we need to evaluate parameter changes in 3 dimensions. 14 It is estimated that ligament dissection of the subtalar joint affects the alignment correction, but only bony anatomical considerations were made. The clinical scores were only postoperative comparisons, and differences in parameter improvement were not evaluated.
In conclusion, the amount of correction of the subtalar joint differed depending on the ligament dissection of the subtalar joint and shape of the talar component.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231205299 – Supplemental material for Assessment of Changes in Hindfoot Alignment of Total Ankle Arthroplasty for Ankle Osteoarthritis on Weightbearing Subtalar X-ray View
Supplemental material, sj-pdf-1-fao-10.1177_24730114231205299 for Assessment of Changes in Hindfoot Alignment of Total Ankle Arthroplasty for Ankle Osteoarthritis on Weightbearing Subtalar X-ray View by Taro Fujimaki, Hiroaki Kurokawa, Yuki Ueno, Takahide Sasaki, Ananto Satya Pradana, Tunku Naziha Binti Tunku Zainudin, Anne Marie Milo, Takuma Miyamoto, Akira Taniguchi, Hirotaka Haro and Yasuhito Tanaka in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study was approved by the institutional review boards of our affiliated institutions. An opt-out statement regarding the application of medical data was published on our institute’s website. This study was performed in accordance with the principles of the World Medical Association Declarations of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.