
Abstract
Background:
There continues to be controversy regarding treatment options for Achilles tendon ruptures (ATR). The aim of our study is to compare outcomes between operatively and nonoperatively managed Achilles ruptures in young adults (age 18-30 years), which has not been previously evaluated.
Methods:
At a single institution, all patients aged 18-30 years at time of injury who underwent treatment for an acute ATR from 2014 to 2021 were evaluated. Medical records were reviewed to collect demographics, dates of injury and treatment, smoking status, body mass index (BMI), Charlson Comorbidity Index (CCI), rate of deep venous thrombosis (DVT) after treatment, and rate of rerupture. Patients then completed Patient-Reported Outcomes Measurement Information System (PROMIS) physical function (PF) and pain interference (PI) questionnaires. Mann-Whitney nonparametric testing was used to evaluate for any statistical differences in PROMIS scores.
Results:
Sixty-six operative patients qualified and 28 (42%) participated. Thirty-seven nonoperative patients qualified and 14 (38%) participated. All patients had a CCI of 0. One patient in the operative cohort and 2 in the nonoperative reported active smoking. In the operative and nonoperative cohorts, respectively, the average age was 24.4 and 27.8 years; average BMI 26.5 (SD = 4.8) and 27.3 (SD = 4.3, P = .52); DVT rates 4 (6.1%) and 2 (5.4%); and rerupture rates 2 (3.0%) and 1 (2.7%), respectively. PROMIS scores did not differ in the operative and nonoperative groups: PROMIS PF mean of 60.4 (SD = 9.8) and 62.9 (SD = 9.1), respectively (P = .33); as well as PROMIS PI mean of 44.6 (SD = 5.9) and 43.9 (SD = 6.5), respectively (P = .59).
Conclusion:
This study should be interpreted with the understanding that we had a considerable loss to follow-up rate. In the study cohort, we found that young adults with ATR may be considered for either operative or nonoperative management. Rates of DVT, rates of rerupture, and PROMIS scores were not dissimilar between the 2 cohorts.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
There continues to be debate regarding the optimal treatment of acute Achilles tendon rupture (ATR). Over the past 15 years, a growing number of studies have compared nonoperative vs operative treatment of ATR, providing clinicians with estimates of treatment success and complication rates for these approaches. Multiple randomized controlled trials comparing nonoperative treatment with open repair of ATR have reported similar patient-reported outcomes and physical performance with both approaches.8,11 In 2019, Ochen et al 9 published a large systematic review of 10 randomized controlled trials and 19 observational studies involving more than 15,000 patients that showed a higher risk of Achilles rerupture after nonoperative treatment, although operative treatment was associated with risks of various perioperative complications including infections and sural nerve injury. More recent studies using accelerated functional rehabilitation protocols that stress early weightbearing have been shown to lessen the risk of rerupture after nonoperative treatment.13,16
Rupture of the Achilles tendon is most typically encountered in the young to middle-aged active population, with mean age ranging from 37 to 44 years. 17 In younger adult patients <30 years old, surgical intervention has historically been recommended for management of ATR based on anecdotal evidence or surgeon preference. Although the general population as well as athletes have been studied, the younger adult population aged 18-30 years has not been specifically evaluated in this context. Although younger adults may have different functional requirements and expectations compared to the general population, it remains unclear if these factors will affect treatment success and complication rates in the era of modern rehabilitation protocols. The aim of our study is to compare outcomes between operatively and nonoperatively managed Achilles tendon ruptures in young adults aged 18-30 years, with both cohorts using an accelerated functional rehabilitation protocol. Our hypothesis is that both cohorts have equivalent patient-reported outcomes as well as similar rates of deep venous thrombosis (DVT) and rerupture.
Materials and Methods
This is an Institutional Review Board–approved retrospective cohort study. At our single academic institution, all patients aged 18-30 years at the time of injury who underwent treatment for an acute Achilles tendon rupture between 2014 and 2021 were evaluated. International Classification of Diseases, Tenth Revision (ICD-10), codes were used to gather the initial list of patients. To be eligible for participation in this study, individuals were required to meet all the eligibility criteria provided in Table 1. Delayed presentations were excluded. The inclusion criteria for nonoperative management varied among the surgeons and may have changed over the course of the study. Currently, our group considers nonoperative management for patients who are placed in a plantarflexed splint within 48 hours of injury. In cases where the initial splinting was done after this window, some surgeons used magnetic resonance imaging (MRI) or ultrasonography to assess the size of the Achilles defect gap. There was no strict gap size cutoff used to determine qualification for nonoperative treatment as many other variables were considered when considering the optimal treatment. Ultimately, all surgeons discussed the benefits and risks of operative vs nonoperative management with each patient, with the goal of informed and shared decision making. Operative repair technique varied based on surgeon preference and included open as well as percutaneous. Both operative and nonoperatively managed patients used an accelerated functional rehabilitation protocol adapted from Willits et al (Table 2). 19
Eligibility Criteria.

Accelerated Functional Rehabilitation Protocol Used by Both Operative and Nonoperative Cohorts.

Patients were required to wear the Aircast boot while sleeping. Patients were permitted to remove the boot for bathing and while getting dressed but were still required to adhere to the weightbearing restrictions according to the rehabilitation protocol during those activities. All patients received a removable below-the-knee orthosis with a 2-cm heel lift to provide approximately 20 degrees of plantar flexion. Adapted from Willits et al. 19
Medical records were then reviewed to collect demographics, date of injury, time from injury to presentation, smoking status, body mass index (BMI), Charlson Comorbidity Index, rate of DVT after treatment, and rate of Achilles rerupture after treatment. Patients were then called and asked to complete Patient-Reported Outcomes Measurement Information System (PROMIS) physical function (PF) and pain interference (PI) computer adaptive testing (CAT) questionnaires. The PROMIS PF CAT utilizes a 121-item bank of questions, whereas the PROMIS PI CAT draws from a 40-item question bank to evaluate the limitations of daily activities, pain, and physical activity. Higher scores on the PROMIS PF indicate greater patient function whereas higher PROMIS PI scores indicate a greater degree of pain interference. PROMIS instruments use standardized T scores designed to return a mean score of 50 and a SD of 10 in the general population of the United States. 12 The comprehensive set of questionnaires provided by PROMIS have been studied and shown to be an excellent method for measuring outcomes for patients with foot and ankle injuries. 10 Recently, a retrospective cohort study by Ochen et al 10 validated the use of PROMIS PF as a reliable and perhaps the most useful instrument for comparing functional outcomes between operative and nonoperative treatment groups in the setting of acute Achilles tendon Rupture.
Basic descriptive statistics were used for all data sets derived from demographics and outcome scores. Mann-Whitney nonparametric testing was used to evaluate for statistical differences in PROMIS scores. Significance was set at a P value less than .05.
Results
In total, 66 patients qualified for the operative cohort, with 28 (42.4%) responding to our survey request. In the nonoperative cohort, 37 patients qualified and 14 (37.8%) responded. Mean follow-up was 4.7 years for the operative cohort and 3.7 years for the nonoperative. The average age was 24.4 years in the operative cohort and 27.8 in the nonoperative group. The average BMI in the operative cohort was 26.5 (SD = 4.8) and 27.3 (SD = 4.3) in the nonoperative cohort, which was not statistically different (P = .52). All patients across both groups had a Charlson Comorbidity Index of 0. One patient in the operative cohort and 2 patients in the nonoperative cohort reported active smoking. Demographics and clinical characteristics are listed in Table 3.
Demographics and Clinical Characteristics of Study Population. a
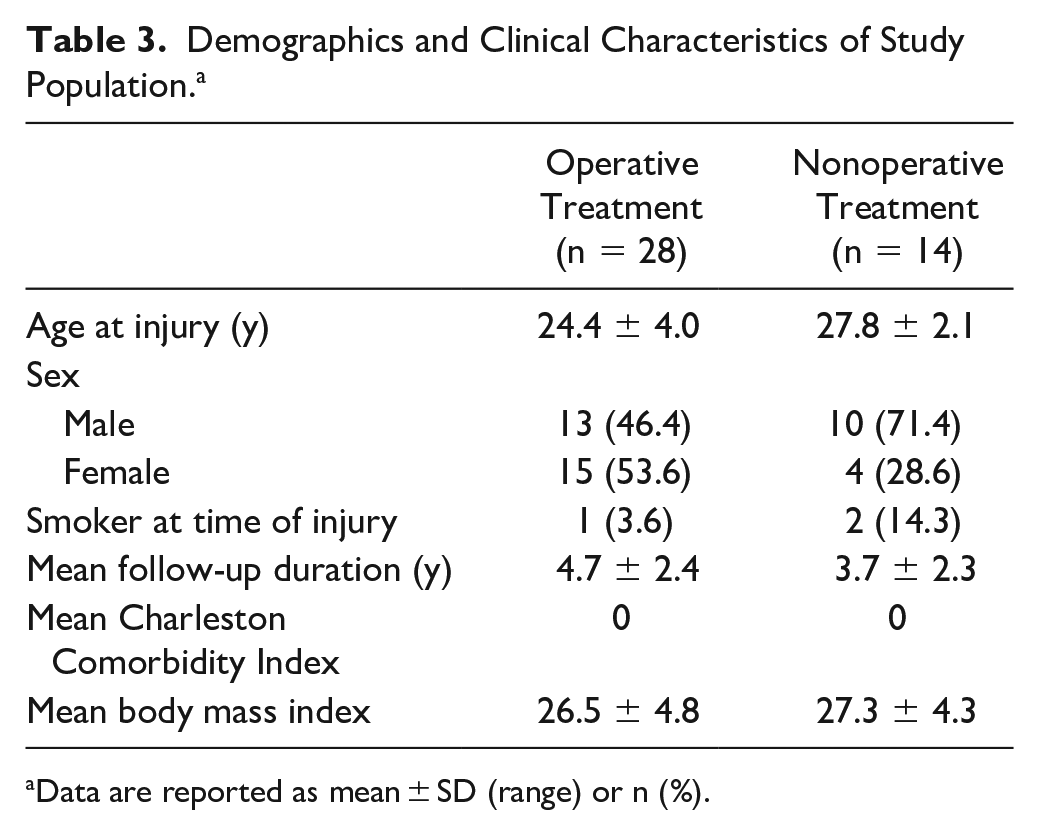
Data are reported as mean ± SD (range) or n (%).
PROMIS PF and PI scores did not significantly differ between the operative and nonoperative cohorts (Figure 1). The PROMIS PF mean was 60.4 (SD = 9.8) in the operative cohort and 62.9 (SD = 9.1) in the nonoperative cohort (P = .33). The PROMIS PI mean was 44.6 (SD = 5.9) in the operative cohort and 43.9 (SD = 6.5) in the nonoperative cohort, also not significantly different (P = .59). The rates of DVT were similar with 4 (6.1%) in the operative cohort and 2 (5.4%) in the nonoperative cohort. Rerupture rates were also similar, with 2 (3.0%) in the operative cohort and 1 (2.7%) in the nonoperative cohort.

Comparison of PROMIS (A) PF and (B) PI scores. There was no statistically significant difference between the operative and nonoperative cohorts. (ns, not significant; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System.)
Discussion
With the sample size numbers available, we found no significant differences in patient-reported outcomes, rates of DVT, and rerupture rates when comparing operative vs nonoperative treatment of acute Achilles tendon rupture in patients aged 18-30 years. Our findings corroborate the results of several high-level randomized controlled trials that found comparable patient-reported outcomes after operative vs nonoperative management of acute ATR in the general population, and our rates of rerupture and DVT are within the range of existing literature as well.1,3,5,6,11,19 To our knowledge, the current study is the first to compare nonoperative treatment with surgery in the younger adult population, a group typically considered for operative repair rather than rehabilitation alone with the goal of restoring maximum functionality and physical performance.
A growing number of studies have been published on the optimal treatment of acute ATR. A meta-analysis published in 1997 by Lo et al 4 showed the rate of Achilles rerupture to be 2.8% for operatively treated and 11.7% for nonoperatively treated patients. However, a randomized controlled trial published in 2010 by Willits et al 19 reported an overall rerupture rate of 2.8% for operatively treated and 4.2% for nonoperatively treated patients, likely reflecting the implementation of a novel accelerated functional rehabilitation protocol. Furthermore, Ochen et al 9 conducted a systematic review and meta-analysis of 10 randomized controlled trials and 19 observational studies comparing operative vs nonoperative treatment, which found no significant difference in rerupture rate if accelerated functional rehabilitation was used. In Norway, a recent multicenter, randomized, controlled trial compared nonoperative treatment, open repair, and minimally invasive repair in 554 adults aged 18-60 years with acute ATR. 7 This study found that open repair or minimally invasive surgery was not associated with better patient-reported outcomes than nonoperative management at 12 months from injury. However, they also reported a lower risk of Achilles tendon rerupture in the operative groups at 0.6% regardless of approach, compared to 6.2% rerupture rate in the nonoperative group, in contrast to other recent trials that showed no difference in the incidence of rerupture.5,16,19 Operative Achilles tendon repair is associated with an increased risk of infection, risk of sural nerve injury with resultant deficits in skin sensation, and higher direct health care costs as well as indirect costs (eg, sick leave days) when compared to nonsurgical treatment, although this may vary between countries.2,14,15,18
There are some limitations to this study. This is a single-institution retrospective study with limited sample size and relatively sparse follow-up, which limits the generalizability of our results. In addition, our survey-based methodology may introduce bias as those with complications or dissatisfaction may be more inclined to respond. The lower response rate is unsurprising given the age of our participants and proximity to a college town, with many patients having moved out of town or changed contacts since the initial injury and treatment. This study is also underpowered to determine any differences between open vs percutaneous Achilles repairs though we hope to do this in the future. Finally, it is important to note that this patient population primarily comprised individuals who were not focused on athletic pursuits and exhibited a wide range of baseline physical function. As such, return to prior activities or sports was not formally evaluated because of concerns about the influence of multiple confounding factors. However, we believe that the utilization of validated PROMIS scores in this study adequately and meaningfully captures outcomes within this diverse population.
Conclusion
This retrospective analysis comparing surgical and nonoperative management of ATR (with both groups participating in a uniform accelerated functional rehabilitation protocol) in young adults aged 18-30 years found no statistically significant differences in patient-reported outcomes, rerupture rates, or incidence of DVT. The findings should be interpreted in light of the dropout rate, which was considerable. Our study suggests that patients aged 18-30 years of age may be considered for either operative or nonoperative treatment. Our findings are consistent with those reported in the growing number of randomized controlled trials and meta-analyses that showed no significant differences between operative and nonoperative treatment in the general adult population. However, further higher-level studies are required to guide decision making in this younger patient population.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231198849 – Supplemental material for Midterm Outcomes of Operatively and Nonoperatively Managed Achilles Tendon Ruptures in Young Adults
Supplemental material, sj-pdf-1-fao-10.1177_24730114231198849 for Midterm Outcomes of Operatively and Nonoperatively Managed Achilles Tendon Ruptures in Young Adults by Laurence Ge, Noah Saunders, Dakota Betts, James R. Holmes, David M. Walton and Paul G. Talusan in Foot & Ankle Orthopaedics
Footnotes
Author Note
All work was performed at the University of Michigan, Ann Arbor, Michigan.
Ethical Approval
Ethical approval for this study was obtained from University of Michigan Institutional Review Board (HUM00213665).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.