
Abstract
Background:
Total ankle replacement (TAR) surgery has increased in recent decades. The aim of this study was to investigate the evolving burden of revision surgery and risk factors and timing of revision or explant.
Methods:
Using the 2010 to 2020 PearlDiver M151Ortho data set, this retrospective cohort study identified primary TAR, TAR revision, and TAR explant patients via Current Procedural Terminology (CPT) and International Classification of Disease Procedural (ICD-P) codes. This database contains billing claims information across all payers and sites of care in the United States. Patient factors investigated included age, sex, and Elixhauser Comorbidity Index (ECI). Annual incidence for primary TAR was normalized per 100 000 covered lives in the data set for each year of study and recorded. Annual incidence of revision TAR and explant were normalized per 100 TARs performed for each year of study. Multivariate logistic regression analyses were performed to determine independent risk factors for revision TAR or explant. For explants, the eventual intervention by 2 years was analyzed. Ten-year timing and survival to revision or explant surgery following unilateral TAR were characterized.
Results:
A total of 10 531 primary, 1218 revision, and 1735 explant TARs were identified. After normalization, TAR utilization increased by 284% from 2010 to 2020, annual TAR revisions rose 28%, and annual TAR explants decreased 65%. Independent predictors of revision TAR were younger age (odds ratio [OR] 1.29 per decade decrease) and higher ECI (OR 1.23 per 2-point increase). Independent predictors of explant included younger age (OR 1.80 per decade decrease), female sex (OR 1.17), and higher ECI (OR 1.35 per 2-point increase). The 10-year implant survival rate was 91.8%, of which 73% of revisions and 83% of explants occurred in the first 3 years following index TAR.
Conclusion:
TAR utilization has grown substantially over the past decade, with minimal increases in the annual rate of revision surgery with respect to index procedures performed.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
End-stage ankle arthritis is a debilitating condition, significantly impairing patient mobility and quality of life. 13 With improvements in total ankle replacement (TAR) device and instrumentation, 4 its utilization has steadily increased over the past decades.12,35 Studies indicate that more than 5000 TARs are being performed globally each year with high levels of long-term postoperative satisfaction.1,12,20,21,24,25,28,29,36 Notably, most of these studies have used either large billing-claims databases or been limited to small institutional studies. Importantly, the trends and predictors of revision surgery following TAR have not been well characterized.
Adverse events following TAR have been reported to be between 13.5% and 17.5%.7,14,36 Common complications include surgical site infection, thromboembolic events, joint instability, aseptic loosening, and cyst formation.2,14,26,36 These have been associated with patient factors, such as age, smoking status, length of stay, and preoperative comorbidity level.7,8,16 Such complications may predispose to revision, explant, or even amputation following the initial ankle replacement. 37
Current data on revision rates following TAR is mixed. A Medicare study by Tucker et al 32 reported the 9-year revision rate of TAR at 11%. Another meta-analysis by Onggo et al 22 reported the all cause 10-year revision rate of TAR to be 30.5%. The study by Tucker et al may present a disproportionally older patient population as its analysis was limited to the Medicare population, whereas that of Onggo et al was limited by small sample sizes—with only 262 cases available for 10-year follow-up analysis.
The current study aims to expand on prior research by defining the incidence of TAR, revisions, and explants from 2010 to 2020 and defining demographic predictors of such subsequent surgeries. Furthermore, the timing of revision or explant procedures were characterized from the time of TAR. We hypothesized that, despite an increase in the gross number of revision TAR and explant surgeries in the past decade, the proportional incidence of revision surgery relative to the number of TARs performed annually has remained stable or declined. This could be due to surgical advancements reducing the need for revision surgery. Further, we hypothesized that younger age and higher comorbidity index are risk factors for revision surgery. These populations could be at greater risk for revision due to increased activity burden on the implant and greater risk for postoperative complications, respectively.
Methods
Database and Cohort
The large, national, multiinsurance, administrative 2010-2020 PearlDiver M151Ortho database was used to conduct this retrospective cohort study. The M151Ortho database contains billing claims information on more than 151 million patients across all sites of care and payer types in the United States. Given its massive scope, this data set is ideal for characterizing overall trends in orthopaedic care. This is a well-validated database that has become commonly used for orthopaedic research.9 -11,27,29 PearlDiver data is patient matched at the analysis level but is exported in deidentified and aggregated form. As such, individual patient-level analysis can be performed without compromising patient confidentiality. Our Institutional Review Board granted all studies using this database exemption from review.
Patients who underwent primary TAR between 2010 and 2020 were identified by Current Procedural Terminology (CPT) code 27702 (total ankle reconstruction with implant). Those who underwent TAR revision were identified by either CPT-27703 (total ankle reconstruction revision) or other CPT/ICD-P codes indicating revision of TAR if performed on the same day as CPT-27704 (removal of total ankle replacement implant). Patients who had TAR explant without concurrent revision TAR were identified by CPT-27704.
After cohort identification, patient characteristics were tabulated, including age, sex, and Elixhauser Comorbidity Index (ECI, a longitudinal summary measure of patient comorbidity burden constructed via ICD diagnosis code). ECI was grouped by units of 3 for ease of analysis and to maximize even distribution of patients in each group.
Characterizing Trends, Predictors, and Outcomes of Primary TAR, Revision, and Explant Surgery
The incidence of primary, revision TAR, and TAR explant was characterized for each year from 2010 to 2020. The incidence of primary TAR was normalized per 100 000 covered lives in the data set for each year of study, whereas the incidence of revision TAR and TAR explant was normalized per 100 TARs performed annually. The percentage change in annual incidence between 2010 and 2020 was determined for each procedure.
Univariate analysis was performed to compare the characteristics of those who underwent TAR revision or explant surgery. Differences in sex between patients in the 2 groups was determined by Pearson chi-squared analysis. Welch t test was used to compare average age and ECI between the patients in the 2 groups.
Multivariate analysis was then performed to determine independent patient-level predictors of having revision surgery or explant surgery with respect to the index TAR population. Odds ratios were calculated for each variable analyzed and compared to respective reference categories. All statistical analysis was performed within the PearlDiver system, with statistical significance reached at P < .05. Prim9 (GraphPad Softwares, San Diego, CA) and Microsoft Excel (Microsoft Corporation, Redmond, WA) were used to create all figures.
Outcomes following TAR explant without same-day revision surgery were characterized as arthrodesis, amputation, arthroplasty, or no identified procedure/other procedure based on the incidence of manually grouped CPT or ICD codes related to these procedures in the 2 years following explant surgery.
Timing of Revision or Explant in the 10 Years Following TAR
The timing of revision surgery or explant following TAR was determined by characterizing the annual incidence of these events in the 10 years following patients’ index TAR. The PearlDiver system was configured to output the timing of revision surgery with respect to individual patients’ index TAR. Bilateral TAR patients were excluded from this analysis by limiting the incidence of TAR surgery (CPT-27702) among included patients to 1 occurrence. This ensured revision or explant surgery was performed on the same ankle as initial TAR.
Ten-year Kaplan-Meier survival analysis was performed to determine survival of TAR to revision surgery or explant accounting for patient attrition from the data set because of change in patient insurer, death, or any other factor causing loss of follow-up within the data set. As noted above, bilateral TAR patients were excluded from this analysis to ensure laterality of revision, or explant surgery was the same as index TAR.
Results
Study Cohort
From 2010 to 2020, a total of 10 531 primary TAR patients, 1218 revision TAR patients, and 1735 patients who had TAR explant were identified in the data set. Patient characteristics of those in the 3 groups are shown in Table 1. On average, primary TAR patients had an average ± SD age of 62.4 ± 10.3 years and were approximately evenly split between males and females (50.3% vs 49.7%). TAR patients were of moderately high comorbidity burden, with an average ECI of 3.96 ± 3.1.
Univariate Analysis of Characteristics of Patients With Total Ankle Replacement or Revision Surgery From 2010 to 2020.
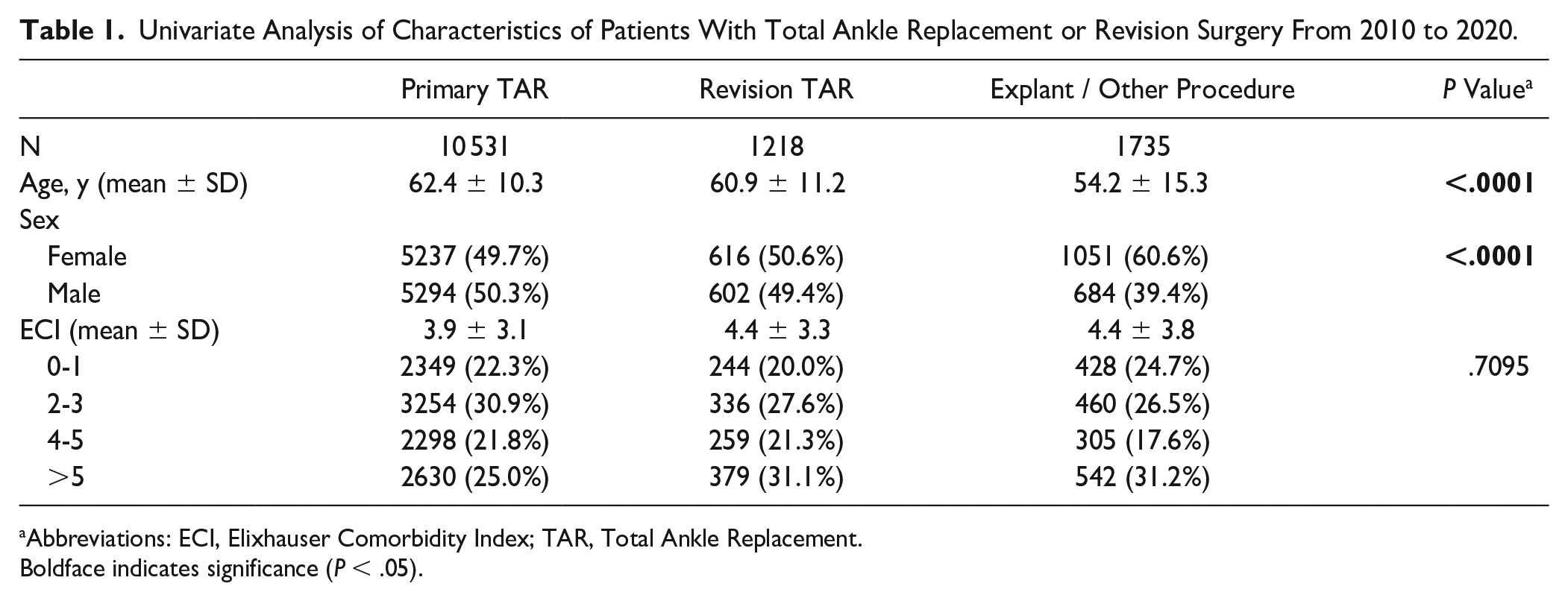
Abbreviations: ECI, Elixhauser Comorbidity Index; TAR, Total Ankle Replacement.
Boldface indicates significance (P < .05).
Notably, TAR revision and explant patients were younger than primary TAR patients (average age of 60.9 ± 11.2 and 54.2 ± 15.3 years, respectively) (P < .0001 for both), with explant patients being significantly younger than revision patients (P < .0001). Revision and explant patients were also more female predominant than index TAR patients at 50.6% and 60.6%, respectively, with explant patients being significantly more female predominant than the revision cohort (P < .0001). Revision and explant patients had a higher ECI than primary TAR patients (average ECI 4.4 ± 3.3 and 4.4 ± 3.8, respectively) (P < .0001 for both).
Trends in TAR, Revision, and Explant
Trends in annual utilization of TAR from 2010 to 2020 are shown in Figure 1. The annual utilization of TAR increased from 0.49 procedures performed per 100 000 covered lives in 2010 to 1.38 per 100 000 covered lives in 2020—constituting a +284% change.

Incidence of total ankle replacement from 2010 to 2020.
Trends in annual TAR revisions and explants are shown in Figure 2. The gross annual burden of TAR revisions was 57 in 2010 and increased to 227 in 2020 (+398% change). The gross annual burden of TAR explants was 167 in 2010 and increased to 183 in 2020 (+9.6% change). Normalized per 100 TAR procedures performed during each year of study, annual TAR revision burden rose from 12.1 per 100 TAR procedures in 2010 to 15.5 per 100 TAR procedures in 2020 (+28% change). In contrast, after normalization, annual TAR explant burden decreased from 35.3 per 100 TAR procedures in 2010 to 12.5 per 100 TAR procedures in 2020 (−65% change).

Incidence of total ankle revision or explant with other procedure from 2010 to 2020.
Of the 1735 patients who had an explant without revision TAR, 654 (37.7%) had arthrodesis performed within the subsequent 2 years, 453 (26.1%) had amputation, 255 (14.7%) had total ankle arthroplasty, and 373 (21.5%) either had no identified procedure or an alternative procedure performed.
Independent Predictors of TAR Revision or Explant
Multivariate analyses for independent patient-level predictors of undergoing either TAR revision or explant are shown in Table 2. Relative to primary TAR, TAR revision was independently associated with younger age (per decade decrease, odds ratio [OR] 1.29, 95% CI 1.24-1.34, P < .0001) and higher ECI (per 2-point increase, OR 1.23, 95% CI 1.19-1.26, P < .0001).
Multivariate Analysis of Predictive Factors for TAR Revision or Explant With Other Procedure.
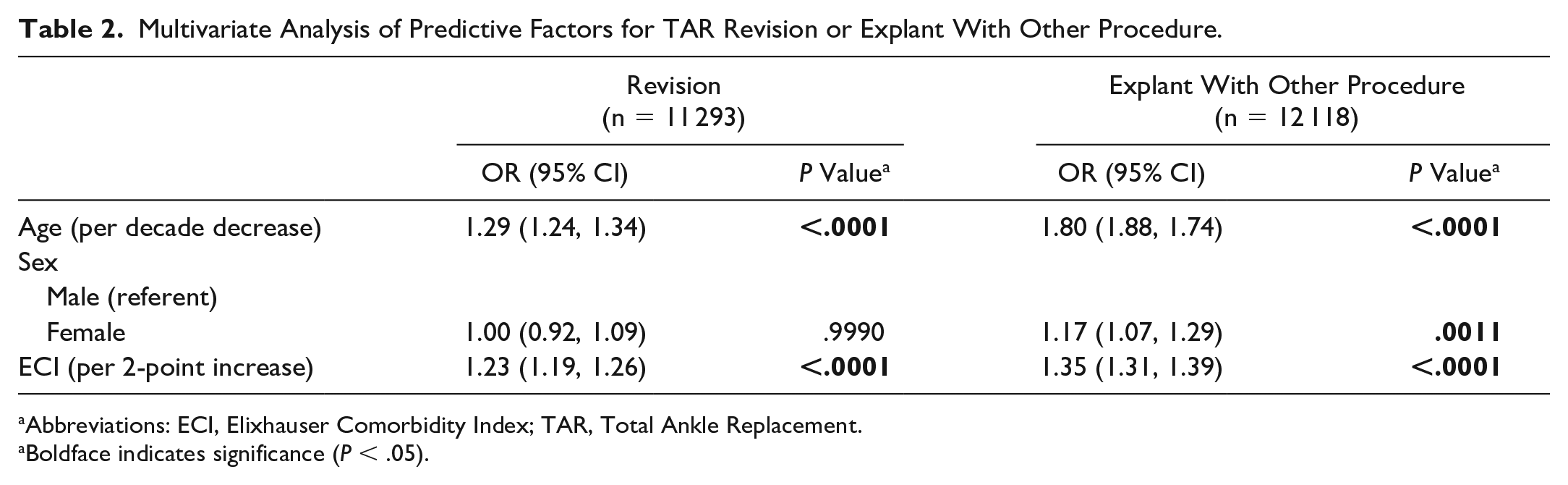
Abbreviations: ECI, Elixhauser Comorbidity Index; TAR, Total Ankle Replacement.
Boldface indicates significance (P < .05).
Relative to TAR, TAR explant was independently associated with younger age (per decade decrease, OR 1.80, 95% CI 1.88-1.74, P < .0001), female sex (compared to male, OR 1.17, 95% CI 1.07-1.29, P = .0011), and higher ECI (per 2-point increase, OR 1.35, 95% CI 1.31-1.39, P < .0001) (Table 2).
Timing of Revision or Explant Following TAR
The timing of revision surgery or explant in the 10 years following index TAR among unilateral TAR patients are shown in Figure 3. For TAR revision, 73% occurred in the first 3 years following surgery, with 39% in the first postoperative year, 22% in the second, and 12% in the third. For TAR explants, 83% took place in the first 3 years postoperatively, with 46% in the first year, 26% in the second, and 11% in the third. The incidence of TAR revision and explant surgeries gradually declined followed the first 3 postoperative years, reaching 1% of all revisions and 0% of all explants by postoperative year 10.
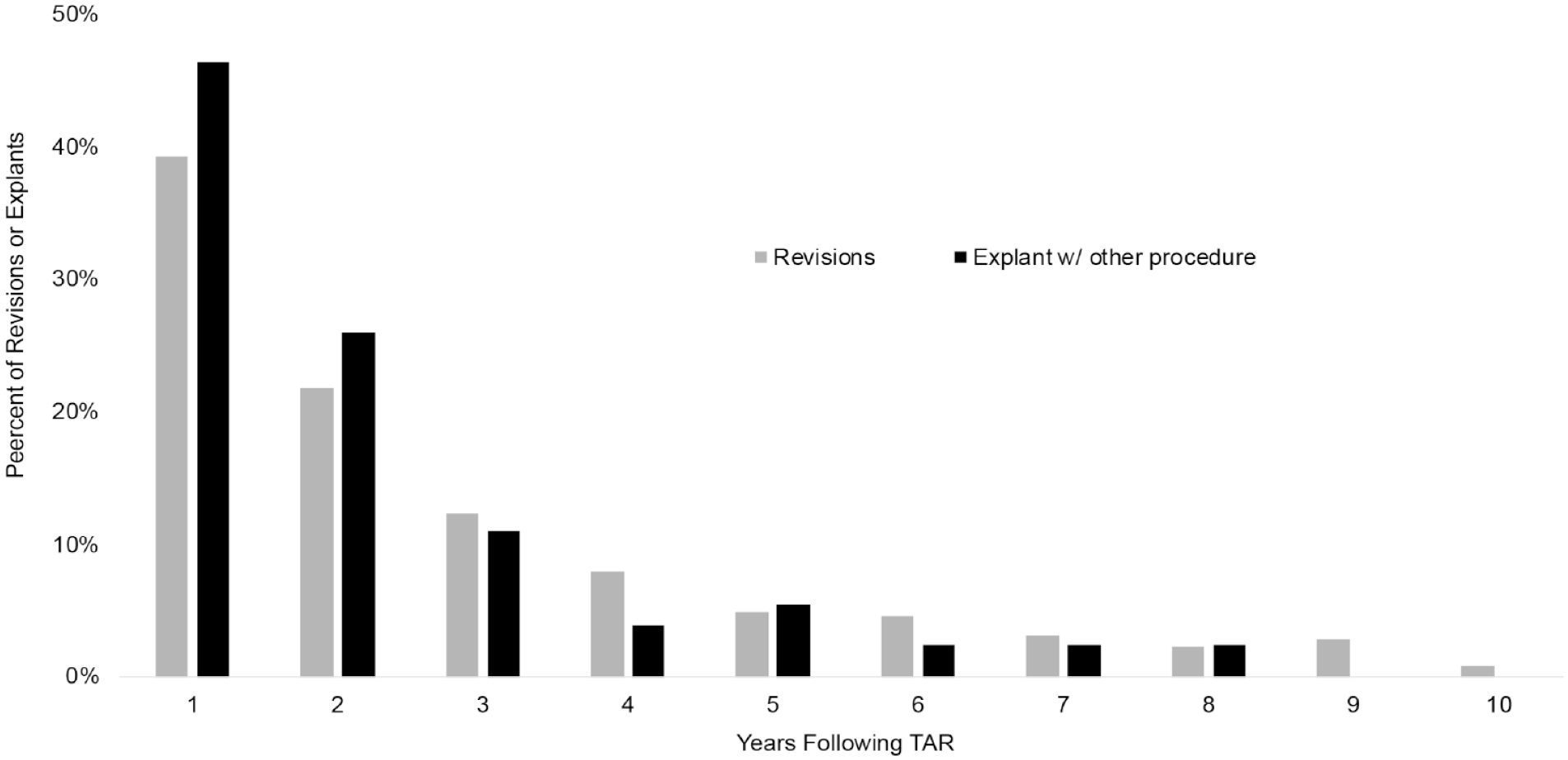
Annual incidence of revision or explant in the 10 years following unilateral total ankle replacement.
The results of 10-year Kaplan-Meier survival analysis with primary endpoints of revision surgery or explant after unilateral TAR are shown in Figure 4. The 10-year survival to revision or explant surgery was 91.8% (95% CI 90.8%-92.8%).

Ten-year survival to revision or explant following unilateral total ankle replacement.
Discussion
With improvements in implant design and postoperative outcomes, TAR has become an increasingly popular option for the treatment of end-stage ankle arthritis. 12 Given the greater use of primary TAR, it is important to consider how the burden of revision surgery has changed. Thus, the present study aimed to characterize trends in the incidence of revision and explant surgery, patient risk factors, and the timing of these procedures following primary TAR.
Patients identified for the current study included 10 531 TAR patients, 1218 TAR revision patients, and 1735 patients who had TAR explant. After normalizing per 100 000 covered lives in the data set for each year of study, the annual utilization of TAR increased 284% between 2010 and 2020. Tucker et al 32 previously reported a 265% increase in TAR utilization in a Medicare population from 2005 to 2014; taken together, these data suggest that TAR has continued to gain popularity in recent years.
The current study also found that, although the gross number of TAR revisions increased 398% between 2010 and 2020, the number of TAR revisions normalized per 100 TAR procedures performed annually only grew 28% over the same interval. Further, although the gross number of TAR explants increased 9.6% from 2010 to 2020, the number of TAR explants normalized per 100 TAR procedures performed annually decreased 65% during this time period. These data suggest that the risk of TAR revision and explant surgery is not growing proportionally with increased TAR utilization, likely reflecting improved surgical outcomes over the years. Previous studies indicate that improving outcomes following TAR are due to continually evolving surgical techniques, implants, and postoperative care and guidance.25,36 Similarly, decreased use of TAR explant surgery is likely secondary to more advanced implants that are more amendable to revision surgery—primarily due to the use of more biocompatible materials, modular implants, and precision surgical techniques that minimize bone resection.4,5 To our knowledge, this is the first study to report trends in the incidence of TAR revision and explant procedures in a national sample.
Patient-level risk factors for revision and explant surgery were evaluated. On multivariate analysis, revision and explant surgery were more common in younger patients. Younger age has been proposed to contribute to an increased risk of TAR revision because of higher life expectancy and higher activity levels among younger patients, both of which increase mechanical stress on the implant. 33 Patients with higher ECI scores were also more likely to undergo revision and explant surgery. This finding aligns with previous reports that comorbidity burden is associated with perioperative complications following TAR. 7 Finally, female sex was found to be an independent predictor of undergoing explant surgery. The reason underlying this difference remains unclear; however, past studies have shown female sex to be an independent predictor of poorer functional outcomes, postoperative complications, and reoperations following joint replacement surgery—including TAR.3,19,23 Given these findings, younger, more comorbid, and female patients should be appropriately risk stratified and counseled regarding their greater risk of suboptimal postoperative outcomes before undergoing TAR.
Of the patients who underwent TAR explant, in the subsequent 2 years arthrodesis was later performed for 654 (37.7%), amputation was later performed for 453 (26.1%), reimplantation of an arthroplasty was performed for 255 (14.7%), and no identified procedure or alternative procedures were performed for 373 (21.5%). These data show that there is a considerable amputation risk for those requiring TAR explant, highlighting the importance of carefully selecting TAR surgical candidates. Notably, past studies have shown similar long-term patient satisfaction following TAR or ankle arthrodesis for management of end-stage ankle osteoarthritis, with TAR being associated with consistently higher revision rates.17,34 Although TAR may be appropriate for some patients—particularly older patients who hope to maximize ankle motion postoperatively—ankle arthrodesis may provide adequate results for most patients while minimizing the risks associated with revision surgery.
In terms of the timing of reoperations, 73% of the 10-year revisions and 83% of the 10-year explant procedures occurred within 3 years of the index surgery. From there, the incidence of TAR revision and explant surgeries declined gradually, reaching 1% of all revisions and 0% of all explants by postoperative year 10. The predominance of early reoperations aligns with a previous report that TAR failure requiring reoperation occurs at an average of 16.4 months postoperatively. 15 This pattern suggests that reoperations are likely driven by early surgical complications, rather than implant failure due to prolonged mechanical stress. As such, future studies should explore surgical technique, operative complications, and perioperative care to elucidate causes of TAR reoperation in the early postoperative period.
Finally, the percentage of TAR patients requiring reoperation was assessed. The 10-year survival to revision or explant surgery was 91.8%. A systematic review published in 2007 reported a 10-year implant survival rate of 77%. 6 More recent studies of 5-year TAR outcomes have reported reoperation rates ranging from 9.1% to 23%.15,18,30 -32 Taken together, data from the current study suggest improved TAR survival to revision and explant surgery in recent years. This finding further supports improved outcomes following TAR as a driver of minimal increases in annual TAR revisions with respect to the rapidly increasing number of TAR procedures performed each year.
As with any study that uses national administrative data, the current study is limited by the accuracy of the data coding. Additionally, causation cannot be determined because of the retrospective nature of the study, preventing a more definitive characterization of the reasons for the observed trends. Additionally, outcomes following TAR explant were not identified for all patients in the study, likely secondary to coding limitations. Despite these limitations, this is the largest study to date characterizing trends in both inpatient and outpatient TAR utilization and outcomes. Given the large sample size enabled by the national administrative database used, overall trends in TAR utilization and outcomes can be ascertained with fair confidence.
Overall, the present study found that although the incidence of TAR procedures performed annually nearly tripled between 2010 and 2010, the annual incidence of TAR revision surgery only modestly increased. In contrast, the incidence of TAR explant surgery declined. The majority of revision/explant procedures occurred within 3 years of initial TAR, with explant patients found to have a substantial risk of subsequent amputation. Several patient factors were identified as independent predictors for revision and explant surgery, including patient age, sex, and comorbidity burden. The minimal increase in revision surgery and decline in explant surgery despite exploding rates of TAR likely suggest improving postoperative outcomes—establishing a positive outlook for the future of TAR. Despite this, there is still a risk of revision and explant surgery following TAR—with potentially devastating consequences for patients. With several patient-level predictors of complications following TAR identified, candidates for TAR should be carefully selected and counseled on the risks of surgery as well as alternative management options—and particular care should be taken in the first postoperative years.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231198234 – Supplemental material for The Burden of Revision Total Ankle Replacement Has Increased From 2010 to 2020
Supplemental material, sj-pdf-1-fao-10.1177_24730114231198234 for The Burden of Revision Total Ankle Replacement Has Increased From 2010 to 2020 by Philip P. Ratnasamy, Gwyneth C. Maloy, Oghenewoma P. Oghenesume, Sean C. Peden, Jonathan N. Grauer and Irvin Oh in Foot & Ankle Orthopaedics
Footnotes
Appendix 1. CPT / ICD codes for TAR revision if performed on the same day as TAR explant ( CPT -27704)
CPT-27700, CPT-27702, ICD-9-P-8156, ICD-10-P-0SRF07Z, ICD-10-P-0SRF0J9, ICD-10-P-0SRF0JA, ICD-10-P-0SRF0JZ, ICD-10-P-0SRF0KZ, ICD-10-P-0SRG07Z, ICD-10-P-0SRG0J9, ICD-10-P-0SRG0JA, ICD-10-P-0SRG0JZ, ICD-10-P-0SRG0KZ, ICD-9-P-8456, ICD-10-P-0SHF08Z, ICD-10-P-0SHF38Z, ICD-10-P-0SHG08Z, ICD-10-P-0SHG38Z, ICD-10-P-0SHG48Z, ICD-10-P-0SWF08Z, ICD-10-P-0SWG08Z, ICD-9-D-V4366, ICD-9-P-8159
Appendix 2. CPT /ICD codes for outcomes following TAR explant
CPT-27703, CPT-27702, ICD-9-D-V4366, CPT-27870, CPT-28705, ICD-9-P-8111, ICD-10-P-0SGF04Z, CPT-27880
Ethical Approval
Ethical approval for this study was waived by Yale Institutional Review Board because no human subjects were involved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.