
Abstract
Background:
Medial cuneiform dorsal opening wedge (Cotton) osteotomy is often used for treating forefoot varus in patients undergoing surgery for stage II posterior tibialis tendon dysfunction. The goal of this study was to examine the radiographic outcomes of Cotton osteotomy with bioactive glass wedge to assess for both maintenance of correction and clinical results and complications. We hypothesized that bioactive glass wedges would maintain correction of the osteotomy with low complication rates.
Methods:
Between December 2015 and June 2016, the charts of 17 patients (10 female and 7 male) who underwent Cotton osteotomy using bioactive glass wedges were retrospectively reviewed. Patient age averaged 56.8 years (range, 16-84). The average follow-up was 6.5 months. Radiographs were reviewed to assess for initial correction and maintenance of correction of medial column sag as well as for union. Charts were reviewed for complications.
Results:
The medial column sag correction averaged 15.6% on the final postoperative lateral radiograph. Meary angle averaged 19 degrees (3.14-42.8 degrees) preoperatively and 5.5 degrees (0.4-20.7 degrees) at final follow-up. All patients achieved clinical and radiographic union. One patient developed neuropathic midfoot pain and was managed with sympathetic blocks. One patient had a delayed union that healed at 6 months without surgical intervention. No patients required the use of custom orthotics or subsequent surgical procedures.
Conclusion:
Cotton osteotomy with bioactive glass wedges produced consistent correction of the medial column with low risk.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Adult acquired flatfoot deformity is a common condition characterized by hindfoot valgus, forefoot abduction, and forefoot varus. While these deformities can occur in varying degrees, they are most often the result of posterior tibialis tendon dysfunction with eventual loss of the medial arch and incompetence of the spring ligament complex. 14 Johnson and Strom have previously categorized posterior tibialis tendon dysfunction into 3 stages and is the most common classification system used today. 8 There have been various treatment options presented in the literature for stage II flatfoot deformities; however the most commonly accepted treatment is a combination of medial displacement calcaneus osteotomy, flexor digitorum longus (FDL) transfer, lateral column lengthening, spring ligament reconstruction, and assessment of a tight gastrocnemius muscle or Achilles tendon. Medial column collapse, manifest as forefoot supination on examination, may be corrected with naviculocuneiform arthrodesis, plantar closing wedge osteotomy of medial cuneiform or first metatarsal, first tarsometatarsal arthrodesis, and opening wedge plantarflexion (Cotton) osteotomy of the medial cuneiform. 6 In the absence of joint instability or arthritis, Cotton osteotomy has been found to give good correction of forefoot supination and decrease lateral forefoot plantar pressures while avoiding fusion of a healthy joint.2,6 The ability to easily tailor the amount of correction and the avoidance of internal fixation to maintain correction are added benefits of the procedure.3,6
Cotton osteotomies can be grafted with iliac crest autograft or allograft. Good results with high union rates have been achieved with both grafts. 6 There are strengths and weaknesses to both autograft and allograft. Iliac crest autograft subjects the patient to potential complications and morbidity of an additional procedure to harvest the graft.6,11 Although allograft avoids another operative procedure, there is concern of bone collapse, increased nonunion rates, and disease transmission.5,12,18 Additionally, allograft is not always an option because of cost, supply, or patient religious beliefs.5,16
A highly porous resorbable bioactive glass wedge is a recently developed graft for use in Cotton osteotomy (Figure 1). These wedges are composed of calcium, phosphate, and silica and have higher compressive strength than both bone allograft and autograft. Bioactive glass was first discovered in 1969 in an attempt to create a material that was bioactive. It had been noted that bioinert materials trigger fibrous encapsulation and would not integrate with bone. It was found that glass composed of 46.1 mol% SiO2, 24.4 mol% Na2O, 26.9 mol% CaO, and 2.6 mol% P2O5 formed a very strong bond with bone such that the bone had to be broken to remove the implant. 9 Consequently, bioactive glass was identified. Bioactive glass has a long history of use in dentistry, craniofacial surgery, and in spinal fusions, where it has been found to be as effective as iliac crest bone graft, while maintaining corrections, with lower complication rates.7,9,17 When implanted into the body, a number of reactions take place, modifying the surface of the material and attracting bone-forming constituents including bone morphogenic proteins. These early reactions allow for the rapid precipitation of calcium and phosphate, which then crystallize into a hydroxyapatite mineral phase that helps cells differentiate into osteoblasts. 9 This leads to the generation of extracellular matrix that results in bone formation. 10 The rate of these surface reactions, along with the gradual resorption of the bioactive glass matrix, results in robust bone formation and replacement of the glass with newly formed bone.9,10

Bioactive glass wedge (Vitrium Bio2 Technologies, Inc, Woburn, MA)
The purpose of this study was to evaluate the clinical and radiographic outcomes of cotton osteotomy with a bioactive glass wedge, specifically we aimed to assess the maintenance of radiographic correction of Meary angle over time. We hypothesized that bioactive glass wedges would maintain correction of the osteotomy with low complication rates.
Methods
Between December 2015 and June 2016, 17 patients (10 females and 7 males; age 56 ± 16 years, range, 16-84 years; Table 1) who underwent Cotton osteotomy for the correction of residual forefoot varus during flatfoot reconstructive surgery using bioactive glass wedges (Vitrium Bio2 Technologies, Inc, Woburn, MA) were retrospectively reviewed. Follow-up averaged 6.5 months (range, 3.2-16.3 months). This study was approved by the Institutional Review Board at 3 institutions, with a single surgeon at each institution.
Demographic Data.

Operative Technique
Patients enrolled in the study had had a symptomatic stage II flatfoot deformity that had failed conservative treatment and had undergone a Cotton osteotomy in conjunction with a variety of hindfoot procedures, including: subtalar fusion, medializing calcaneus osteotomy, FDL to navicular transfer, and posterior tibialis tendon to FDL tenodesis. After the hindfoot had been surgically realigned, the forefoot had been evaluated with the hindfoot held in neutral. In this position, a line connecting the metatarsal heads should be perpendicular to the long axis of the tibia. 6 If the forefoot remained supinated while plantar pressure was applied to the fifth metatarsal head, then a Cotton osteotomy was performed in the following fashion: A dorsal incision was made over the medial cuneiform. A 0.062-inch Kirschner wire was placed into the cuneiform to mark the expected plane of the cut, parallel to the proximal and distal cuneiform articular surfaces. Fluoroscopy was used to identify the midportion of the cuneiform and orientation for the osteotomy, which was then made with an oscillating saw from dorsal to plantar. An osteotome was placed into the osteotomy to gently lever open the medial cuneiform. A Hintermann distractor was used to distract the osteotomy until adequate plantar flexion of the first ray was achieved. The trial implant was then placed into the osteotomy and the foot was inspected for residual forefoot supination with the ankle in neutral. The implant was then placed, the Hintermann distractor was removed, and stability was checked.
Following surgery, the patient was placed into a posterior splint and kept nonweight-bearing. At 2 weeks, sutures were removed, anteroposterior and lateral radiographs were obtained, and the patient was placed into a short nonweight-bearing leg cast. At 4-6 weeks postoperatively, the patient was placed into a CAM boot and allowed weight bearing as tolerated. At 8-12 weeks, radiographs were assessed and the patient was transitioned out of the CAM walker boot into supportive shoes.
Data Collection and Analysis
Charts were reviewed for demographic information including age, sex, and indication for surgery. Standard anteroposterior, lateral, and oblique radiographs were obtained for each patient at the pre- and postoperative visits. Three patients did not have preoperative imaging available at the time of this study. The medial column sag was calculated from the lateral radiograph as the ratio of the length of the dorsal to the plantar cortex of the medial cuneiform. This nonstandard metric of arch height was used because we found this method to be unaffected by slight variations in quality of the lateral radiograph in a computer-aided drawing simulation. Percentage correction was calculated as the difference between the pre- and postoperative ratios (Figure 2). Meary angle was also calculated for all patients preoperatively and at final follow-up with weight-bearing radiographs. Union was defined radiographically by bridging trabeculae at either side of the implant with the adjacent medial cuneiform in addition to clinical union, which was defined by lack of pain at the osteotomy site with weight-bearing, stable medial column with weight bearing and minimal swelling.

Measurement of the dorsal and plantar cortex of the medial cuneiform. These measurements were used to calculate ratios in order to assess the amount of correction from the Cotton osteotomy.
Paired t tests were performed, comparing (a) pre- to postoperative ratios, (b) postoperative to final ratios, and (c) preoperative to final ratios. The null hypothesis was that there was no change in the ratios with the significance threshold set at 0.01.
Results
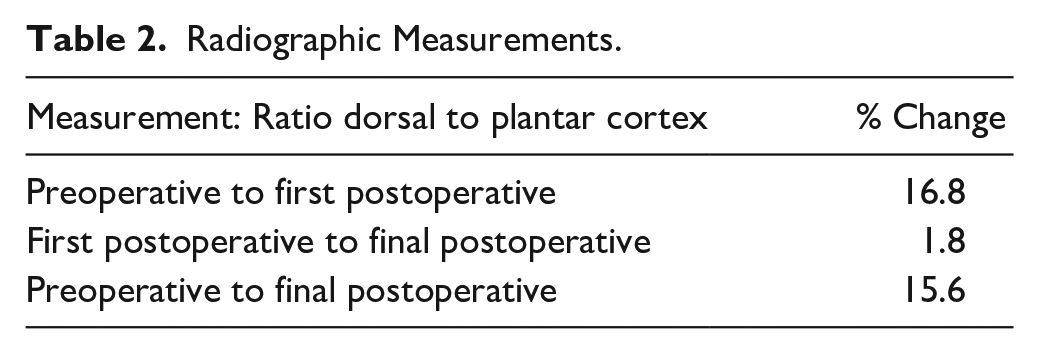
The average correction of medial column sag from preoperative to first postoperative (2 weeks) visit was 16.8% (n=14 P < .001; Table 2). At the first postoperative visit, patients had radiographic correction of their medial column sag dorsal to plantar cortex ratio from 6.4% to 33% (n=14). The average change from the first postoperative visit to the last follow-up visit was 1.8%. (n=17, P = .04). The patients had significantly increased correction of medial column sag of 15.6% with maintenance of the Cotton osteotomy from preoperative to final postoperative lateral radiograph (n=14, P < .001, Table 2). Meary angle changed for 19 degrees (3.14- 42.8 degrees) preoperatively to 5.5 degrees (0.4- 20.7 degrees) at final follow-up (Figure 3).
Radiographic Measurements.

(A, B) Anteroposterior and lateral preoperative weight-bearing, (C, D) first postoperative nonweight-bearing, and (E, F) final postoperative weight-bearing foot radiographs of a patient with successful Cotton osteotomy with bioactive glass wedge.
There were no nonunions of the osteotomy site, but one patient did have a delayed union that healed without surgery by 6 months. No patients required subsequent operative procedures or custom orthotics. One patient had continued midfoot pain that was consistent with neurogenic pain managed with sympathetic blocks. One patient developed ankle arthritis requiring multiple cortisone injections. This patient had a previous triple arthrodesis with residual flatfoot deformity and developed deltoid laxity. At the time of medial cuneiform plantarflexion osteotomy and medial sliding calcaneus osteotomy, she also had a deltoid reconstruction; however, the ankle continued to fail in valgus.
Discussion
We found that the Cotton osteotomy with a bioactive glass wedge produced consistent correction of the medial column with low risk of nonunion. Prior studies have evaluated the corrective power of this osteotomy and shown correction of forefoot varus, first metatarsal elevation, and medial column sag. 13 A recent study looking at midfoot sag was able to demonstrate correction of midfoot sag using the Cotton osteotomy while controlling for concomitant procedures. 1 Additionally, in a biomechanical study of 12 cadaveric feet, another group demonstrated that this osteotomy decreases lateral forefoot plantar pressure and increased medial column pressure. 2
Cotton osteotomies are classically performed using iliac crest autograft. Although iliac crest autograft is often considered the gold standard of graft material, it is not without its drawbacks. Allograft bone is often used but concerns regarding availability, bone collapse, and union rates exist. 5 Bioactive glass is an osteoconductive, osteoinductive, and osteogenic graft material. Additionally, bioactive glass has a significantly higher compressive strength than cancellous or cortical bone, making it less prone to collapse. 10 Unlike porous metal, which always remains present in the bone, bioactive glass remodels to normal bone over time. 19 One of the few studies to assess the effectiveness of this material looked at the ability of bioactive glass to maintain deformity correction in scoliosis surgery. They reviewed 88 patients who underwent posterior spinal fusion for adolescent idiopathic scoliosis with either iliac crest autograft (n=40) or bioactive glass (n=48). At a mean 40-month follow-up, they found an average loss of correction of 15.5% in the autograft group and 11% in the bioactive glass group (P = .025). Additionally, they found fewer infections (5% vs 2%) and overall fewer complications in the bioactive glass group. 7
Bioactive glass has best been described in the craniofacial and periodontal literature. A recent review demonstrated that bioactive glass used in craniofacial reconstructive surgery was associated with good functional and aesthetic results. It is unknown whether this antibacterial effect extends past oral bacteria. Other authors have described grafting cranial vault defects with autologous graft and bioactive glass particles in 2 patients. At 6 months postoperatively, computed tomography (CT) showed that the majority of the defect was converted to bone. 4 In a 5-year prospective study comparing treatments for intrabone defects in cases of aggressive periodontitis, it was demonstrated that bony defects treated with bioactive glass had significantly higher rates of filling (65% ± 50% vs 47.5% ± 38.3%, P = .001). 15
The cost of a new implant is an important factor in its adoption in a cost conscious market. Autograft cost is due to type of graft taken, additional operative time, and patient regional anesthesia not to mention postoperative morbidity. Therefore, the cost of autograft can vary depending on surgery center/hospital type (surgery center, large academic hospital, for-profit hospital, community hospital, etc). One method to estimate cost factors is an additional 30 minutes of operation theater time along with the surgeon’s fee for large autograft harvest. For allograft, a fibula section, iliac crest, or precontoured wedge allografts is often utilized. Depending on the size, the cost can range from $550 to $1400 per allograft. The bioactive glass wedge costs $800 to $1500.
This study has limitations. It is a retrospective review and is therefore prone to lack of blinding, randomization, recall bias and limitations of chart review. Additionally, there were no autograft nor allograft control groups. We did not collect data on patient pain, satisfaction or functional outcome. Because of variability in radiographic quality, we did not use previously reported parameters to measure correction due to lack of reliability, but instead used a CAD method of calculation. Average follow-up was short (6.5 months) and it is possible there would be loss of correction over more time, although in animal studies the bioactive implant has been shown to be more than 95% replaced by bone at 6 months.
In conclusion, the results of this retrospective review demonstrate that Cotton osteotomy using bioactive glass wedges produced similar union rates and maintenance of correction compared to other operative techniques described in the literature. We demonstrated sustained radiographic correction over an average of 6.5 months.
Footnotes
This article was originally published as: Borenstein T, Gonzalez T, Krevolin J, Den Hartog B, Thordarson D. Preliminary experience using bioactive glass wedges for cotton osteotomy. Foot Ankle Orthop. 2018 Dec 11;3(4):2473011418796861. doi:10.1177/2473011418796861.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bryan Den Hartog, MD, and David Thordarson, MD, report personal fees from Bio2 Technologies Inc, outside the submitted work. Janet Krevolin, PhD, is an employee of Bio2 Technologies, inc. In addition, Dr. Krevolin has a patent US-2012-0179271-A1 pending, and a patent US-2015-0073556-A1 pending. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.