
Abstract
Background:
Inversion ankle injuries are extremely common, sometimes causing injury to the peroneus brevis tendon. If more than 50% of the tendon is injured, it oftentimes requires tenodesis to the adjacent peroneus longus tendon. Both Pulvertaft (PT) and side-to-side (SS) techniques have been used for joining the 2 tendons. The purpose of this study was to compare the strength and stiffness of these 2 techniques.
Methods:
Five matched pairs of cadaver ankle specimens were randomized to receive either an SS or PT tenodesis of the peroneus brevis to longus tendons. Following the tenodesis, the specimens were tested for failure load, displacement, energy absorbed at failure, and peak load. Stiffness was also calculated. Paired t tests were performed to detect differences between the 2 conditions.
Results:
There were no statistically significant differences between the SS and PT tenodesis for any of the metrics measured. For stiffness, the techniques were very similar (SS = 10.14 [4.35], PT = 12.85 [1.72]).
Conclusion:
There is no difference in failure load, displacement, energy absorbed at failure, peak load or stiffness between the PT and SS techniques for peroneal tenodesis.
Level of Evidence:
Level V, cadaver study.
Introduction
Tears of the peroneus brevis in which more than 50% of the tendon is torn are frequently treated with tenodesis to the peroneus longus tendon. 9 A variety of techniques have been used for tenodesis including side-to-side (SS) and Pulvertaft (PT) weaving.3,18 The SS technique consists of fixation of the peroneus brevis tendon proximally to the longus with a single proximal connection point. The PF technique involves approximately 3 weaves of the peroneus brevis tendon through the peroneus longus tendon with 1 connection point at the distal aspect of the tendon. A comparison of the 2 techniques has previously been described in the hand literature, with the SS technique being found to be stronger and stiffer than the PT technique.1,14 The procedures are equivalent in technical difficulty. The choice of which to use has depended solely on surgeon preference as biomechanical evidence supporting the use of one over the other is lacking.
Early return to activity and range of motion depends on a secure repair; thus, the initial strength of repair is an important consideration in the choice of tenodesis technique. The objective of this study was to investigate whether the strength of an SS tenodesis is comparable to that of a PT weave for tenodesis of the peroneus longus to brevis. We hypothesized that the PT tenodesis technique would be stronger than the SS as a result of the multiple passes through the peroneus longus tendon.
Methods
Specimen Preparation
Five matched pairs of cadaver ankle specimens were used. The procedures were performed by a fellowship-trained foot and ankle surgeon. Prior to tendon harvest, the right side was randomized to receive either an SS or a PT tenodesis, with the opposing limb subsequently prepared with the alternate technique. An 8-cm incision was made posterior to the lateral malleolus and curved anteriorly at the distal extent over the course of the peroneus longus and peroneus brevis. The superior peroneal retinaculum was divided to access the 2 peroneal tendons (Figure 1). Tenodesis is generally performed approximately 3 to 4 cm proximal to the tip of the lateral malleolus to avoid scarring within the groove. 16 For this study, we chose 3 cm proximal to the tip of the lateral malleolus. The SS or PT tenodesis of the peroneus brevis to the peroneus longus was performed after appropriately tensioning the peroneus brevis by suturing the peroneus brevis to the longus prior to tenotomy. A 2-0 Ethibond Excel suture (Ethicon, Somerville, NJ) was used to perform the tenodesis with a total of 4 figure-of-8 sutures placed at equal positions along the 3 cm of overlap of the tendons (Figure 2). A tenotomy was then performed at the musculocutaneous junction of the peroneus longus and peroneus brevis tendons. Finally, a tenotomy was performed of the peroneus longus distally as it crossed underneath the cuboid.

Operative exposure of the peroneus brevis and peroneus longus tendons through a lateral incision curved around the posterior aspect of the fibula.

Comparison of side-to-side (SS) and Pulvertaft (PT) tenodesis techniques.
Biomechanical Testing
The peroneus brevis tendon was secured proximally within a soft tissue tendon clamp 1 attached to the actuator of an MTS 858 Mini-Bionix (MTS Corp, Eden Prairie, MN; Figure 3). The distal end of the tendon was secured in a matching tissue clamp attached to a 10-kN load cell. Conditioning was performed with a load of 5.0 N for 10 cycles to seat the tissue within the setup. This conditioning load was within the elastic region and well below the first failure point of the tendons. Each specimen was then loaded to failure at a rate of 10 mm/min. Displacement and load were recorded and used to create load versus displacement curves from which the following metrics were obtained: failure load, displacement, and energy absorbed at first instance of failure and the peak load. The first failure load was defined as the first negative inflection point in load; peak load was the highest achieved load of each construct. Stiffness was calculated as the slope of the linear elastic region (Figure 4). The tendons were observed during the failure test to determine the physical mode of failure. Paired t tests were performed to detect differences in the above metric between the 2 graft constructs.
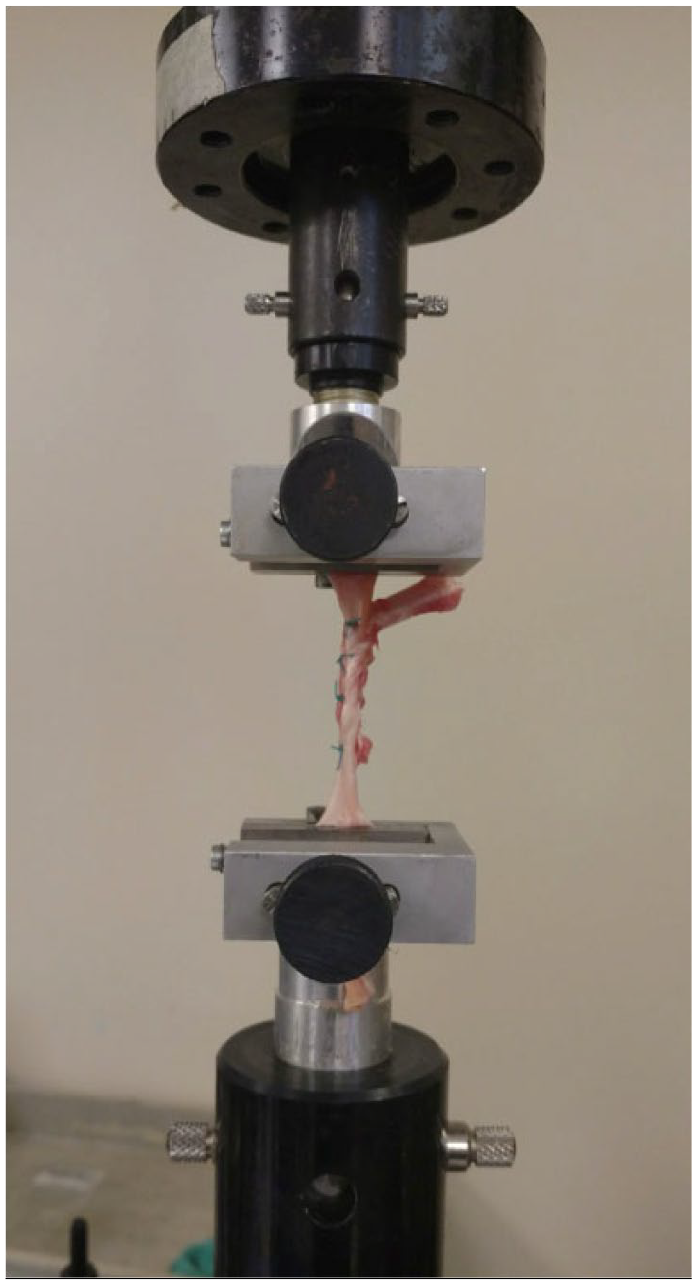
The peroneus brevis tendon was secured proximally and peroneus longus tendon was secured distally into a soft tissue tendon clamps secured to the actuator and load cell of an MTS 858 Mini-Bionix.

An example of a side-to-side versus Pulvertaft peroneus brevis tenodesis load curve for one pair.
Results
There were no statistically significant differences between the SS tenodesis and the PT tenodesis for any of the metrics measured. The largest difference between the tenodesis techniques was found in the load at first failure and peak load (Table 1). For 4 of the 5 SS repairs, the first failure occurred at the distal-most stitch, whereas the fifth failed at the weave site. For 4 of the 5 PT repairs, the first failure occurred at the distal-most stitch, with the fifth failing at the proximal-most stitch (Table 2). Ultimate failure in all tenodesis constructs was a result of the distal stitched tearing proximally through the tendon.
Biomechanical Comparison of Peroneus Brevis Tenodesis Fixations: Side-to-Side Versus Pulvertaft.

Characteristics of the Two Tendon Tenodesis Techniques.

Discussion
No significant difference in strength was found between the 2 fixation techniques in our testing. Although the study was similar to that performed involving the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons, the results are much different. In a previous study in the hand literature comparing flexor tendon repair using the SS and PT techniques, the SS repair was significantly stronger than the PT repair. 1 In our study, we found no difference between the repair techniques. The SS and PT technique methods previously described 1 involves more suture material with more areas of fixation. We simplified the tenodesis procedure with 4 figure-of-8 sutures. However, based on the results showing neither suture technique to be significantly stronger, we conclude that either repair technique can be used when performing the tenodesis procedure.
A cadaveric study calculating muscle forces on various plantarflexors and dorsiflexors of the lower extremity found the forces on the peroneus longus and peroneus brevis at full body weight were 55 and 37 N, respectively. The force on the peroneus longus and peroneus brevis decreased to 14 and 9 N at one-fourth body weight. 11 It is unclear if these values have any relevance in the postoperative period as many surgeons delay full weight-bearing postoperatively for several weeks.2,13 In fact, the median duration of immobilization following a peroneal tendon tenodesis is approximately 7.0 weeks, with range-of-motion exercises limited for a median of 4.5 weeks. 17 With this consideration, all of the repairs performed exceeded the normal physiologic force on the peroneus longus and peroneus brevis even if full weight-bearing was begun immediately in the postoperative period.
Much of the literature shows that active and passive range of motion reduces adhesion formation, assisting with recovery of range of motion of the joint, and reducing postoperative recovery time has come from the hand literature.5,6,12,15 Although some surgeons have used extended periods of up to 6 weeks of cast immobilization and nonweight-bearing, there have been some reports of surgeons shortening their immobilization and starting weight-bearing much earlier at 2 to 4 weeks.4,7,8 Whichever technique the surgeon uses to perform the tenodesis, the surgeon can safely prescribe either partial weight-bearing or begin mobilization much earlier. An important consideration, however, is that biologic effects occur on the tendon in the postoperative period, including a reduction in strength for several days after surgery before healing begins. 10
Fresh-frozen cadaveric tendons were shown to be similar to those of tendons in vivo. 11 To control for variation, the repair techniques were randomized with regards to laterality, and handling each tendon was consistent to reduce variation in the methods and technique. Therefore, we assume that the tendons tested immediately following tenodesis represent the immediate postoperative period.
Our sample size was a limitation in the study. We used 5 matched pairs of cadavers without evidence of previous peroneal tendon injury. A 2-tailed post hoc power analysis revealed that the study was adequately powered for first failure load (79%), whereas power for all other metrics was below 52%. Thus, a total sample size of at least 18 would be required to achieve 80% power. Also, this study only provided a comparison of the tenodesis techniques at time zero. The repair strength may be affected over several weeks as the tendon begins to heal. The load cell size of 10 kN was a limitation as the failure loads were measured at around 1% of the load cell capacity.
Conclusion
We were unable to find a significant difference with regard to load at failure or stiffness between the PT and SS techniques for peroneal tenodesis. Surgeons may use either technique for peroneus brevis to peroneus longus tenodesis. Further clinical research is needed to determine which technique is more beneficial in patients.
Footnotes
This article was originally published as: Janney CF, Iloanya M, Morris R, Panchbhavi VK. Peroneus brevis tenodesis: side-to-side or weave? Foot Ankle Orthop. 2018 Nov 28;3(4):2473011418797267. doi:10.1177/2473011418797267.
Disclaimer
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government. LCDR Cory Janney is a military service member (or employee of the U.S. Government). This work was prepared as part of his official duties. Title 17, USC, §105 provides that ‘Copyright protection under this title is not available for any work of the U.S. Government.’ Title 17, USC, §101 defines a U.S. Government work as a work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.