
Abstract
Background:
This study aimed to assess the preferred operative treatment for patients over the age of 60 with end-stage ankle arthritis and perspectives on total ankle replacement (TAR) among American Orthopaedic Foot & Ankle Society (AOFAS) members. Associated factors were analyzed for potential contraindications among members with different levels of experience.
Method:
A questionnaire containing 6 questions was designed and sent to 2056 members of the AOFAS. Responses were received from 467 orthopaedic surgeons practicing in the United States (76%), Canada (5%), and 26 other countries (20%). Participants were grouped for response comparisons according to country as well as experience level. Differences in contraindications were compared using χ2 tests or exact tests.
Results:
Respondents practicing in the United States and surgeons who perform 11 or more TARs per year tended to recommend operative treatments favoring TAR and displayed recognition of its increasing role (P < .05). Overall, respondents felt that 41% of typical patients over 60 years old with end-stage arthritis would be best treated with TAR. Talus avascular necrosis, morbid obesity (body mass index >40 kg/m2), and poorly controlled diabetes with neuropathy were most recognized as the absolute contraindications to TAR. Surgeon’s experience affected the consideration of these clinical factors as contraindications.
Conclusions:
Total ankle replacement has a substantial and increasing role in the treatment of end-stage ankle arthritis in patients over the age of 60. Absolute and potential contraindications of the procedures were indicated from a cross-sectional survey of AOFAS members. Surgeons more experienced with total ankle replacement felt more comfortable employing it in a wider range of clinical settings.
Level of Evidence:
Level III, therapeutic.
Ankle arthritis is a disabling condition affecting quality of life in thousands of patients throughout the world. 8 Using validated outcome instruments, physical impairment in patients with ankle arthritis was found to be equivalent to that reported in end-stage kidney disease and congestive heart failure. 29 Failure of nonoperative treatments of end-stage ankle arthritis in an older adult often leads to consideration of ankle arthrodesis (AA) or total ankle replacement (TAR). While AA has long been accepted as the standard treatment, several limitations of AA, including stiffness, abnormal walking gait, and adjacent joint arthritis, are well recognized.4,16 Despite the high early failures in first-generation TAR, the enthusiasm for motion-preserving reconstruction led to continued development of subsequent generations of prosthesis, both fixed and mobile-bearing models.7,40 The improvement in prosthesis design and instrumentation as well as positive experience among orthopaedic surgeons and patients may account for the 6- to 10-fold increase in the number of TARs over the past decade, as shown in national-level databases in the United States.24,26
Ankle arthritis is unique in its etiology, which is most commonly posttraumatic in 70%, as demonstrated in a consecutive series of 639 patients presenting to a tertiary care center. 28 This is in contrast to hip and knee arthritis, which are usually idiopathic in nature. Accordingly, many associated factors are considered when planning operative treatment for patients with ankle arthritis, including adjacent joint arthritis, bilateral ankle arthritis, talus avascular necrosis, coronal plane deformities, and history of infection.3,29 In addition, patient characteristics such as activity level, obesity, diabetes, and neuropathy also play an important role in the treatment decision.18,39
There is currently no universal guideline to indicate the use of TAR vs AA in patients over the age of 60 with end-stage ankle arthritis. 13 Orthopaedic surgeons may adopt a general philosophy of joint replacement by only selecting patients who are older, physically less demanding, not obese, and without limb deformities as they grow expertise. On the other hand, emerging information in the literature indicates highly satisfactory outcomes in TAR among experts in the field, including the success in the management of challenging conditions such as prior infection, severe deformity, and obesity.2,32,35 Information on outcomes from broader range orthopaedic surgeons is not available, especially regarding proper indications and contraindications. The purpose of this study was to assess the preferred operative treatment of end-stage ankle arthritis in patients over the age of 60 among American Orthopaedic Foot & Ankle Society (AOFAS) members with various exposures to both AA and TAR for over a decade. 5 Associated factors were analyzed for potential contraindications among members with different levels of experience.
Materials and Methods
We performed a questionnaire-based analysis of the operative preferences of orthopaedic foot and ankle surgeons regarding surgeon preference for AA or TAR in a variety of clinical situations. Specifically, the questionnaire was designed to capture baseline surgeon experience in both ankle arthrodesis and ankle replacement, current status of practice, location of practice, perception of trends, and absolute contraindications for ankle replacement. The 6 questions and their orders were approved by the Evidence-Based Medicine (EBM) Committee of the AOFAS and was subsequently approved by the Board of Directors. The questions are listed in Table 1.
American Orthopaedic Foot & Ankle Society (AOFAS) Member Ankle Arthritis Treatment Survey.

After the study was deemed by the institutional review board to be exempt, the questionnaire was sent by email to 2056 members of the AOFAS on May 19, 2017. The survey was opened for a month with 2 additional electronic reminders sent to the members approximately 10 days apart. A total of 467 members responded to the survey, making the response rate of 23%. Orthopaedic surgeons who responded were practicing in the United States (76%), Canada (5%), and 26 other countries (20%).
Statistical Analysis
Descriptive statistics, including means and standard deviations for continuous variables and proportions for categorical variables of AOFAS member responses, were conducted. The distributions of continuous variables were evaluated for normality using the Shapiro-Wilk test and through evaluation of histograms. Participants were grouped for response comparisons according to country (United States, Canada, other), as well as according to experience performing ankle surgery, defined as number of ankle surgeries performed per year (0, 1-5, 6-10, 11-15, ≥16). Differences in responses were compared between country groups (United States, Canada, and other) and ankle surgery groups using generalized linear models with P values adjusted for multiple comparisons (Tukey). Respondents were further categorized as having low (1-10 TAR surgeries per year) or high experience (≥11 TAR surgeries per year). Differences in contraindications for TAR in patients older than 60 years with end-stage ankle arthritis and failure of nonoperative treatment were compared using χ2 tests or exact tests, as appropriate.
Results
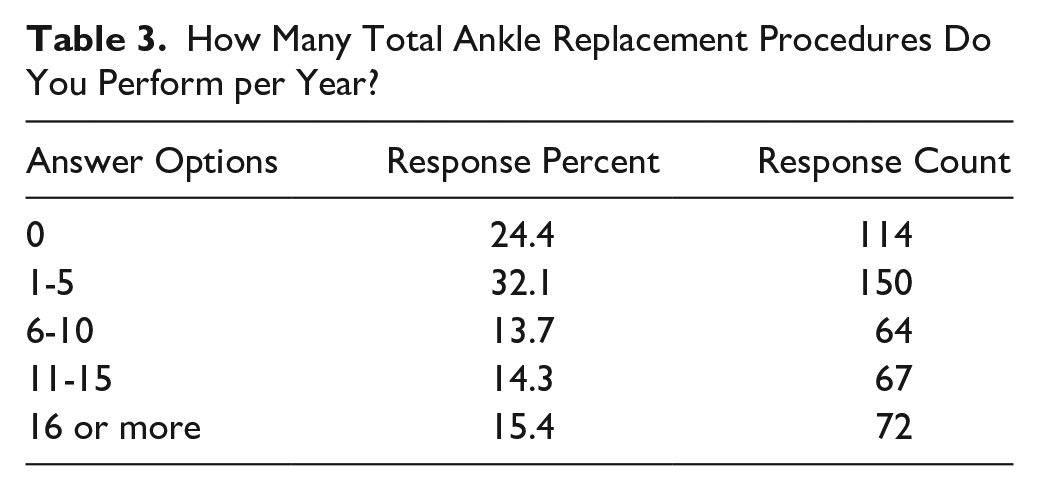
AA was found to be a more commonly performed procedure than TAA. Most of the respondents (56.6%) perform 6 to 15 AAs per year and only 1.3% of the respondents do not perform this procedure (Table 2). In contrast, most of the respondents (56.5%) perform 5 or fewer TAR procedures per year, and 24% of the respondents do not perform this procedure (Table 3).
How Many Ankle Arthrodesis Procedures Do You Perform per Year?

How Many Total Ankle Replacement Procedures Do You Perform per Year?
When presented with typical patients over 60 years old with end-stage ankle arthritis and failure of nonoperative treatment, the respondents reported that 53% of patients may benefit most from AA, 41% may benefit most from TAR, and 6% from other operative options. The tendency to recommend operative treatments favoring TAR is shown from respondents practicing in the United States vs other countries (Figure 1, P < .05 for all comparisons) and respondents who perform more frequent TARs per year (Figure 2, P < .05 for all comparisons). There were no significant differences in responses between those practicing in the United States and Canada.

Treatment of patients over 60 years old with end-stage ankle arthritis and failure of nonsurgical treatment, by country.

Relationship between total number of ankle replacement surgeries performed per year and percentage of patients in practice who might benefit from arthrodesis, replacement, or other surgical options.
Regarding the role of TAR now compared to 5 years ago for patients over 60 years old with end-stage ankle arthritis, 72% of the respondents found it to be increasing while 22% found it to stay the same, and only 6% found it decreasing. The tendency to indicate the increasing role of TAR is shown from respondents who perform more frequent TARs per year (Figure 3, P < .05 for all comparisons) and those practicing in the United States vs other countries (Figure 4, P < .05 for all comparisons) except Canada, where no significant differences were found.
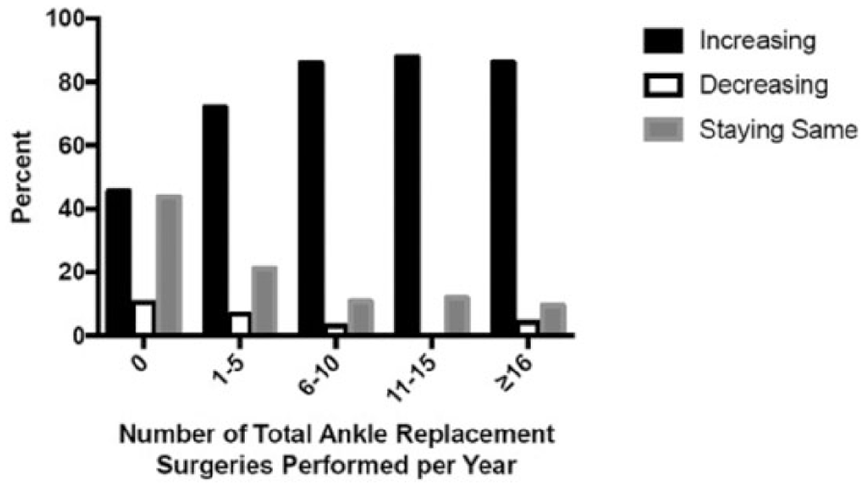
The current role of total ankle replacement compared with 5 years ago for treatment of patients over 60 years old with end-stage ankle arthritis (results shown by number of total ankle replacement surgeries performed by respondent per year).

The current role of total ankle replacement compared with 5 years ago for treatment of patients over 60 years old with end-stage ankle arthritis (results shown by country).
Considering patients over 60 years old with end-stage ankle arthritis and failure of nonoperative treatment, most of the respondents reported that talus avascular necrosis (64%), more than 25 degrees of varus or valgus deformity (63%), manual labor or physically demanding jobs (52.4%), morbid obesity (77%), poorly controlled diabetes with neuropathy (93%), and history of ankle or foot infection (55%) were absolute contraindications for TAR for most respondents (Table 4). In order to take into account surgeon’s experience in TAR, the data were analyzed to reflect the experience of those more frequent performers (≥11 cases per year) vs those less frequent performers (1-10 cases per year) (Table 4). Between the 2 groups, statistically significant differences (all P < .05) were found in the percentage of response of obesity, morbid obesity, 15 to 25 degrees of varus or valgus deformity, more than 25 degrees of varus or valgus deformity, manual labor or physically demanding jobs, and history of ankle or foot infection as potential absolute contraindications, with fewer experienced surgeons reporting these as absolute contraindications. Overall, greater than 50% of responders in both groups indicated that talus avascular necrosis, morbid obesity, and poorly controlled diabetes with neuropathy are absolute contraindications. Fewer than 50% of respondents in both groups indicated the following factors as absolute contraindications for TAR, including bilateral end-stage ankle arthritis, subtalar arthritis, midfoot arthritis, less than 15 degrees of varus or valgus deformity, 15 to 25 degrees of varus or valgus deformity, well-controlled diabetes, obesity (body mass index [BMI] >30 kg/m2), and smoking. It is worth noting that more than a third of both groups of respondents indicated smoking as an absolute contraindication.
In Patients Over 60 Years Old With End-Stage Ankle Arthritis and Failure of Nonoperative Treatment, What Are the Absolute Contraindications for Total Ankle Replacement?

Abbreviations: BMI, body mass index.
Statistically significant P value.
Considered as an contraindication by less frequent performers.
Considered as an contraindication by more frequent performers.
Discussion
The results from the survey of AOFAS members demonstrated a cross-sectional view of the current state of operative treatment of end-stage ankle arthritis. Our results have shown that AA is the most commonly used operative option among the respondents. While 24% of the respondents do not perform TAR, only 1% do not perform AA. This is in agreement with epidemiological studies that analyzed national and regional utilization rates. Two separate studies using different databases found the utilization of AA in the early 2000s to be over 6-fold of TAR.26,33 However, the trend in use of the TAR is dramatically increasing while the use of AA has been steady. 24 Most respondents from this survey have indicated their perception of the increasing role of TAR in the past 5 years. The positive perception of the role of TAR was significantly more common in subsets of respondents who have had more exposure to the procedure (eg, practicing in the United States or higher number of procedures per year). An appreciation of the value and increasing role of TAR in the treatment of ankle arthritis is reflected in the fact that respondents overall considered TAR as the best treatment for 41% of typical elderly patients with an isolated end-stage ankle arthritis. A recent systematic review including 7942 patients from 58 studies supports that TAR has a positive impact on patients’ lives regarding improvement in pain, function, gait, and range of movement, with the survivorship of 89% at 10 years. 41
The absolute contraindications to TAR from the perspective of AOFAS members were demonstrated by the survey results. Three conditions were identified by the majority of respondents regardless of their level of experience in TAR. Talus avascular necrosis has long been recognized a culprit for talar component subsidence, loosening, and early failure.9,22 Morbid obesity can theoretically put excessive load to the prosthesis-bone interface and causes other risks associated with metabolic syndrome.15,23 A retrospective study found an increased long-term risk of implant failure in obese patients (BMI 30-45 kg/m2), especially with the diagnosis of primary osteoarthritis. 31 While several studies have shown comparable success and complications between obese and nonobese patients, further studies are required to demonstrate outcomes specific to morbidly obese patients (BMI >40 kg/m2).1,2,6 Poorly controlled diabetes with neuropathy posed substantial challenge in wound healing, potential infection, postoperative weightbearing, and the development of Charcot’s arthropathy. 27 Choi et al 11 reported worse outcomes, higher wound complications, and lower implant survival in patients with poorly controlled diabetes compared to those with controlled diabetes and nondiabetics in a comparative study of 173 patients at a minimum follow-up of 2 years.
Several associated conditions, such as bilateral end-stage ankle arthritis, subtalar arthritis, and midfoot arthritis, were not recognized by the respondents as absolute contraindications to TAR. Adjacent joint arthritis or bilateral ankle arthritis may be considered unfavorable factors for AA due to the risk of symptomatic arthritis in those locations after a motion segment is lost from a fused ankle.12,16 On the other hand, these conditions may be better tolerated after a TAR where motion is preserved or improved.14,34 Mild hindfoot deformity (<15 degrees), well-controlled diabetes, and obesity (BMI >30 kg/m2) were identified by less than 10% of the respondents as absolute contraindications. Growing evidence in the literature supports the compatibility of these conditions with TAR. Deformity correction is an integral part of the success in TAR procedure. 10 Studies have demonstrated successful results of deformity correction in TAR at multiple stages, including soft tissue balancing, implant positioning, and corrective osteotomies.25,35,37 Degrees of deformity accounted for the highest differences in opinions between respondents with more or less experience in TAR. This could be explained by the need of expertise for ancillary procedures during the index surgery to achieve a plantigrade foot. 37 Patients with well-controlled diabetes have been shown to perform similar to nondiabetic patients after a TAR regarding clinical success, complications, and implant survival. 11 Obesity, defined as BMI more than 30 kg/m2 but less than 40 kg/m2, could indicate the comfort level of respondents in the treatment of this subset of patients, especially with the controversial influence of obesity and the lack of standardized thresholds. Smoking was not indicated by the majority of respondents as an absolute contraindication. However, more than a third of each group of respondents recognized the harmful effects of this modifiable perioperative factor. It has been shown that active cigarette smokers had a significant increase in the risk of wound breakdown and less improvement in functional outcome after surgery. 21 Interestingly, those effects appeared to be reversed by tobacco cessation.
Manual labor or physically demanding jobs, history of ankle or foot infection, and more than 25 degrees of varus or valgus deformity were demonstrated to be potential contraindications to TAR. The degree to which these 3 factors were considered a contraindication was highly dependent on the respondent’s level of experience. TAR has a steep learning curve. 30 A retrospective study looking into the learning curve of TAR found that most of the operative variables as well as clinical and radiological outcomes stabilized after a surgeon had performed 28 cases. 38 Surgeons who had more experience may be able to understand the functional need of patients with higher physical demands, which may require a more strategic approach to maximize stability and longevity of the construct. Examples of these potential options are the use of highly crosslinked polyethylene line, bone-preserving implants, computer navigation, component reinforcement, and revision prostheses.17,19 Potential source of infection in the foot and ankle could be assessed and effectively eradicated in certain cases prior to TAR. A retrospective study reported no infection after a TAR in 22 patients with a known history of ankle joint sepsis or osteomyelitis. 32 Perioperative workup to rule out quiescent infection was required, including the consideration of white blood cell count, erythrocyte sedimentation rate, C-reactive protein, radiographs, advanced imaging, joint aspiration, and frozen section.
There are pertinent limitations with the use of survey questionnaire in this study. The response rate of 23% may not truly represent the entire population effectively. However, the total response of 467 was similar to a most recent published AOFAS member survey with the total respondents of 462. 36 Information regarding the numbers of AA and TAR procedures performed per year was not verified. The associated factors offered to the respondents as potential absolute contraindications were presented unidirectionally without an opportunity for further clarification. Nevertheless, this study has its strength as a snapshot of an evolving practice in the treatment of ankle arthritis from worldwide membership over a decade after the introduction of third-generation total ankle implants. 20 Future studies involving large-scale prospective cohorts or registries are required to generate adequate information regarding associated factors of poor outcomes that can be considered contraindications.
Total ankle replacement has a substantial and increasing role in the treatment of end-stage ankle arthritis in older adults. The absolute contraindications of TAR for the majority of respondents were talus avascular necrosis, more than 25 degrees of varus or valgus deformity, manual labor or physically demanding jobs, morbid obesity, poorly controlled diabetes with neuropathy, and history of ankle or foot infection. Surgeons more experienced with total ankle replacement felt more comfortable employing it in a wider set of clinical settings. The information from this study could be used as a guideline when considering an operative treatment for end-stage arthritis.
Footnotes
This article was originally published as: Phisitkul P, Glass N, Ebeling PB, Klein SE, Johnson JE. Perspectives in treatments of end-stage ankle arthritis among orthopaedic surgeons: analysis of an American Orthopaedic Foot & Ankle Society (AOFAS) member survey. Foot Ankle Orthop. 2018 Jul 27;3(3):2473011418779976. doi:10.1177/2473011418779976.
Authors’ Note
Institution(s) at which the work was performed: American Orthopaedic Foot & Ankle Society, 9400 W. Higgins Road, Suite 220, Rosemont, IL 60018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.