
Abstract
A 77-year-old woman presented with a mucous cyst on the lateral aspect of the interphalangeal joint of the first toe caused by contact pressure with the second toe from hallux valgus. She complained of discomfort and discharge from the left first toe for approximately 4 months. Physical examination showed the second toe pressing strongly against the first toe due to hallux valgus and discharge from the skin on the lateral aspect of the interphalangeal joint of the first toe. Magnetic resonance imaging showed a cystic lesion at the same level. The patient underwent a modified scarf osteotomy of the first metatarsal for hallux valgus to resolve the contact pressure between the toes—considered the cause of the mucous cyst—and resection of mucous cyst. Forefoot weight bearing was allowed 6 weeks after surgery. As of 1 year after surgery, she has had no recurrence of the cyst. The score on the Japanese Society for Surgery of the Foot hallux metatarsophalangeal-interphalangeal scale improved from 59/100 points to 92/100. This outcome suggests that hallux valgus correction should be considered when a mucous cyst is associated with contact pressure due to a hallux valgus deformity. To the best of our knowledge, there are no previous reports of a mucous cyst caused by contact pressure between the first toe and second toe due to hallux valgus.
Introduction
Mucous cysts commonly present as a cystic lesion located eccentrically on the distal phalanx of a finger or lesser toe.44,46,47 They are also known as ganglion, mucoid, myxoid, synovial, or myxomatous cysts, as these conditions all have similar histopathology.2,4,6,8,11,14,23,32 Histologically, they extend from the joint capsule and consist of a fibrillated inner layer of randomly arranged collagen fibers and mesenchymal cells, which are thought to produce a viscous fluid that fills the cyst.12,18,21,25,34
Mucous cysts and similar cysts of the toes cause disability due to pain and discomfort from ill-fitting footwear.15,25 They occasionally become ulcerated because the skin overlying the cyst is usually thin, and the resulting discharge may be troublesome.16,43 Only 2% of ganglion cysts occur in the toes, and most of these occur in the lesser toes. 36 However, they less commonly present over the interphalangeal (IP) joint of the first toe.1,28 There was a report that 1 of 15 cases of mucous cysts of the IP joint of the first toe was symptomatic and was thus treated with operative excision. 9 Four of 27 cases of mucous cysts of the first toe IP joint or ganglion cyst of the ankle were treated with operative excision. 26
Recent reports have described mucous and similar cysts caused by repetitive stress or trauma from ill-fitting shoes. 10 However, to the best of our knowledge, there has been no reported case of a mucous cyst associated with contact pressure between the first and second toes caused by hallux valgus where the first metatarsal deviates medially and the first toe deviates laterally and presses strongly against the second toe.
Here, we report a case of a mucous cyst on the lateral aspect of the first toe IP caused by second toe contact pressure due to hallux valgus, which we successfully treated with resection of the cyst and reduction of the pressure by metatarsal osteotomy.
Case Report
The patient provided informed consent for this report.
A 77-year-old woman, who noticed left toe deformity about 30 years ago, was referred to our department with a history of 4 months of serous discharge from the left first toe, causing progressive discomfort when wearing shoes and walking. Physical examination revealed no limitation of range of motion of the first toe. However, the second toe was seen to be pressing strongly against the first toe at the IP joint, resulting in contact pressure between the 2 toes (Figure 1a). There was also serous discharge from the first toe at this site (Figure 1b). No neurovascular deficit was noted. The score on the Japanese Society for Surgery of the Foot (JSSF) hallux metatarsophalangeal-interphalangeal scale was 59/100 (pain 30/40, function 29/50, alignment 0/10). The patient gave a visual analogue scale (VAS) pain score of 6/10. Scores on the Self-Administered Foot Evaluation Questionnaire (SAFE-Q)40,41 were 69.4/100 points for pain and pain-related symptoms, 50.4/100 points for physical functioning and daily living, 41.6/100 points for social functioning, 58.3/100 points for shoe-related problems, and 65.0/100 points for general health and well-being.
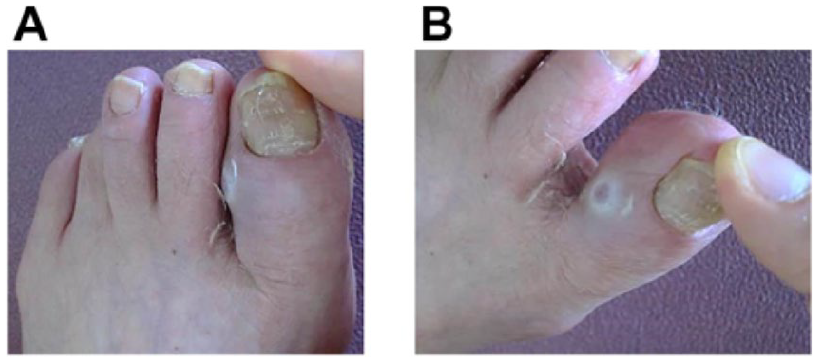
(A) Preoperative photographs of the left first and the second toes. The second toe was in close contact with the first toe. (B) Discharge from the medial aspect of the first interphalangeal joint is seen.
A weight-bearing anterior-posterior (AP) view of the left hallux demonstrated no osteoarthritic changes in the IP joint of the first toe. Hallux valgus deformity was seen, and the hallux valgus angle (HVA) was 30 degrees; the intermetatarsal (M1M2) angle was 16 degrees (Figure 2). Magnetic resonance imaging (MRI) showed a cystic mass measuring 8 × 5 × 5 mm, with regular smooth borders, localized to the IP joint and communicating with the IP joint space. On T1-weighted images, the entire mass had a relatively homogeneous low-intensity signal (Figure 3a). T2-weighted images and fat-saturated T2-weighted images revealed a homogeneous high-intensity signal within the tumor (Figure 3b, c). MRI findings were consistent with the features of mucous and similar cysts such as ganglion, mucoid, myxoid, synovial, and myxomatous cysts.

Preoperative radiograph (anterior-posterior view, weight bearing) showing hallux valgus deformity. No degenerative changes associated with osteophyte formation are seen.
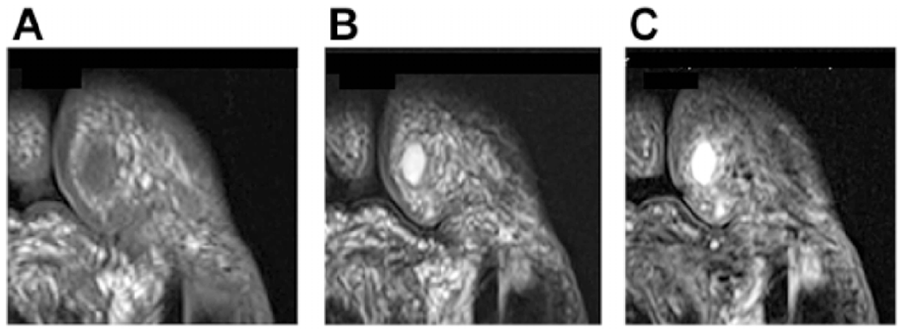
(A) Preoperative magnetic resonance image showing a homogeneous low-intensity in 8 × 5 × 5-mm soft tissue mass with regular borders on T1-weighted imaging. (B) A homogeneous low-intensity signal on T2-weighted imaging. (C) A homogeneous high-intensity signal on T2 fat-saturated imaging.
Therefore, the preoperative diagnosis was a mucous or other cyst caused by contact pressure from the second toe due to hallux valgus. We decided to perform complete resection of the cyst with metatarsal osteotomy to relieve the contact pressure between the first and second toes, which we considered to be the cause of the cyst. However, we did not perform osteophytectomy at the first toe IP joint because of the absence of osteoarthritic signs in this joint.
We made a 5-cm longitudinal skin incision along the first metatarsal over the medial aspect of the foot. A modified scarf osteotomy13,33 with lateral release was performed to relieve the contact pressure between the first and second toes. Next, we performed resection of the cyst. A spindle-shaped skin incision encircling and including the cyst was made over the cyst at the level of the IP joint of the first toe. As the skin incision was deepened, a thick, colorless gelatinous fluid began to exude from the well-encapsulated, thin-walled, fibrous mass adherent to the lateral aspect of the IP joint capsule (Figure 4a). Complete excision of the cyst with connected soft tissue adjacent to the joint capsule was performed, and all excised soft tissue was sent for histologic examination (Figure 4b). The skin was closed with 4-0 nylon sutures. There were no intraoperative complications. Postoperative radiography showed the HVA had improved to 13 degrees and intermetatarsal angle improved to 10 degrees (Figure 5). The patient was allowed to resume full weight bearing on the heel the day after surgery, and forefoot weight bearing, including toe-off of the first toe, was allowed 6 weeks after surgery. The postoperative course was unremarkable.

(A) Intraoperative findings showing the cyst originating from the first interphalangeal joint capsule (arrow) and (B) the gross specimen after excision.

Postoperative anterior-posterior radiograph showing proper alignment of the first metatarsal.
Histopathologic examination of the lesion revealed a multiloculated cystic structure and fibroblastic proliferation associated with a mucous, mucoid, or myxomatous synovial stroma (Figure 6). These findings were consistent with the diagnosis of a mucous cyst.
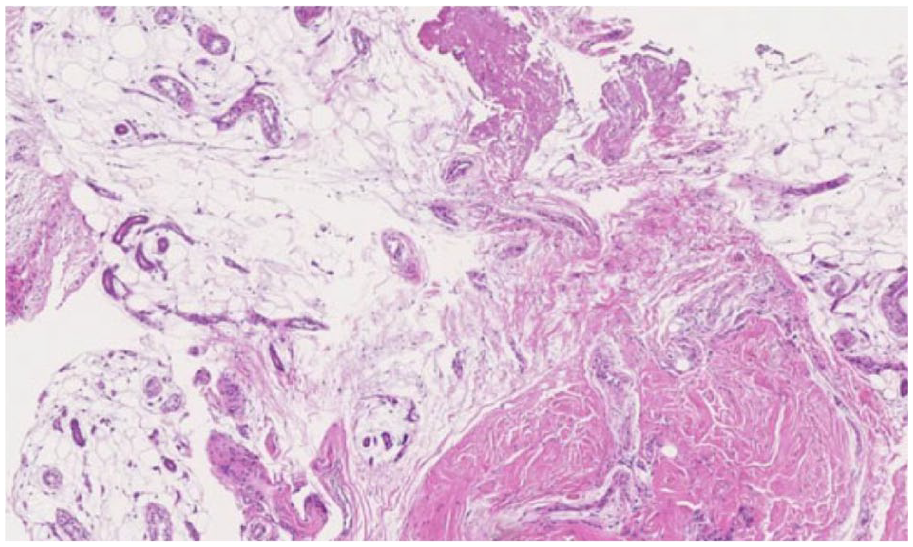
Histopathological micrograph showing a dense fibrous wall of the cyst and fibroblast proliferation in a mucous, mucoid, or myxomatous synovial stroma (hematoxylin and eosin stain).
On postoperative evaluation, the left hallux appeared normal, the contact pressure between the first and second toes was completely relieved, and there was no discharge from the first toe (Figure 7). At the 1-year follow-up visit, the patient had remained asymptomatic, and MRI showed no recurrence of the mass. The JSSF hallux metatarsophalangeal-interphalangeal score improved to 40 points for pain, 37 points for function, and 15 points for alignment, totaling to 92/100, and the VAS score improved to 0/10. The SAFE-Q scores improved to 77.7/100 points for pain and pain-related symptoms, 70.4/100 points for physical functioning and daily living, 75.0/100 points for social functioning, 83.3/100 points for shoe-related problems, and 80.0/100 for general health and well-being.

Postoperative photograph showing the first and the second toes after simple excision. No discharge is seen from the medial aspect of the first interphalangeal joint, and the contact pressure between the first and second toes has been relieved.
Discussion
Here, we report the case of a 77-year-old woman who presented with a mucous cyst on the lateral aspect of the IP joint of the first toe caused by contact pressure on the second toe from hallux valgus. The differential diagnosis included rheumatoid nodule, acquired fibrokeratoma, 3 periungual fibroma of tuberous sclerosis, 31 acral mucinous fibrokeratoma, 39 fibrous histiocytoma, 30 myxoma, 20 superficial acral fibromxyoma, 37 and superficial angiomyxoma, 38 glomus tumor, or neurofibroma. 5 Our preoperative diagnosis based on history, physical examination, radiographic images, and MRI was a mucous or similar cyst. This diagnosis was confirmed by the postoperative histologic examination.
Numerous theories exist as to the etiology of mucous and similar cysts. The reported prevalence of mucous cysts in osteoarthritis varies widely,11,22,29,32,35 and it is possible that the development of osteophytes and an increase in synovial fluid associated with osteoarthritis are contributing factors to the formation of mucous cysts. 6 However, in our patient, there were no osteoarthritic changes at the IP joint of the first toe. Instead, there was contact pressure between the first and second toes due to a hallux valgus deformity, and the mucous cyst was seen at the contact point on the first toe. In this case, the mucous cyst most likely developed because of this excessive contact pressure, and so the mucous cyst would recur if the contact pressure persisted, even if we had resected the cyst. Therefore, we corrected the hallux valgus deformity to relieve that contact pressure.
Some authors describe conservative treatment, including orthoses for hallux valgus deformity,19,24,27,45 but none have described orthoses for mucous and similar cysts of toes. A toe splint or spacer to offload the contact area might be useful to avoid or minimize pressure. However, they were unlikely to relieve related symptoms directly in this case, as conservative treatment has a limited capacity to correct and cannot reverse hallux valgus deformity, while successful surgery can.17,21
Many methods have been proposed for the treatment of mucous and similar cysts. These include conservative treatment, such as cyst wall puncture and aspiration, electrical and chemical cautery, cryotherapy, injection of steroids or sclerosing agents, and irradiation.7,12,16 Operative excision yielded more consistent results in a study showing that recurrence rates were 11% after excision and 63% after conservative therapy. 42 Therefore, we opted for operative treatment. In other studies of recurrence rates, Constant et al 11 and Crawford et al 12 reported rates of 0% to 5% after more aggressive operative excision involving the use of skin grafts or advancement of local flaps. In contrast, the less aggressive operative excision of cysts, with deep soft tissue excision, was reported to be much higher, at 30%. 35 Nonetheless, our patient experienced no recurrence following excision of the cyst and relief of the contact pressure between the first and second toes. This strongly suggests that the mucous cyst was caused by the contact pressure due to the hallux valgus deformity. Moreover, it is possible that correction of a hallux valgus deformity or other pressure-relief measures may improve outcomes after resections of mucous cysts.
One limitation of this report is the short follow-up period. Although the mass has not recurred as of the latest follow-up visit 1 year after surgery, further follow-up is necessary. Another limitation in terms of concluding that hallux valgus correction might improve outcomes after mucous cyst resection is the slight possibility that there could be ongoing degenerative changes in the first toe IP joint or the synovial tissue. Such degenerative changes must be considered given the patient’s advanced age, although no signs of osteoarthritic changes were detected on the imaging studies.
In conclusion, we report here a rare case of a 77-year-old woman with a mucous cyst on the lateral aspect of the first toe IP joint caused by contact pressure with the second toe due to a hallux valgus deformity. This combination was successfully treated by performing hallux valgus correction with a first metatarsal osteotomy to reduce the contact pressure with simultaneous resection of the mucous cyst. The patient has had a favorable outcome at 1 year with relief of the pain and associated symptoms including discharge from the first toe. This report demonstrates that reducing the contact pressure between the first and second toes by performing metatarsal osteotomy for hallux valgus should be considered when a mucous cyst is associated with such contact pressure and hallux valgus deformity.
Footnotes
This article was originally published as: Tonogai I, Yamasaki Y, Nishisho T, Sairyo K. Mucous cyst at the interphalangeal joint of the first toe caused by contact pressure with the second toe due to hallux valgus: a case report. Foot Ankle Orthop. 2018 Jul 27;3(3):2473011418775101. doi:10.1177/2473011418775101
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.