
Abstract
Background:
Although percutaneous surgery for the treatment of hallux valgus is popular in Europe, there is sparse English written literature documenting its efficacy. This study described the operative techniques using percutaneous basal closing wedge osteotomy of the first metatarsal in correction of moderate to severe hallux valgus (HV) and its short-term clinical outcomes. We postulated that satisfactory correction of hallux valgus (HV) angle, intermetatarsal (IM) angle, and patients’ clinical outcomes could be achieved with this technique.
Methods:
We conducted a retrospective review of 25 feet in 23 patients who underwent a percutaneous basal closing wedge osteotomy of the first metatarsal (MT1) combined with a mini-open modified McBride procedure and mini-open resection of medial eminence. Follow-up averaged 21.5 months. Radiographic outcomes included pre- and postoperative HV angle, IM angle, absolute and relative shortening of MT1, and time to union. American Orthopaedic Foot & Ankle Society (AOFAS) scores were compared between pre- and postoperatively.
Results:
The average HV angle improved from 39.4 (range, 29-58.3) degrees preoperatively to 14.7 (range, 0.1-23.2) degrees postoperatively (P < .05). IM angle improved from 14.9 (range, 6.7-22.4) degrees to 6.6 (range, 0.9-14.8) degrees (P < .05). The average absolute shortening was 3.8 (range, 0.27-12.91) mm and the relative shortening was 0.8 (range, 0.05-1.91) mm. There was no delayed union or malunion at the osteotomy site. The average AOFAS score improved from 39 (range, 12-50) to 81 (range, 70-93) (P < .05).
Conclusions:
Satisfactory hallux valgus deformity correction and patients’ outcomes were achieved with this technique. Our results are similar to results reported in other studies using open techniques. There was no malunion or delayed union of the osteotomy.
Level of Evidence:
Level IV, case series study.
There are many different operations used for the correction of moderate to severe hallux valgus deformity. 15 Most are combinations of soft tissue release and bony procedure. Basal osteotomy of the first metatarsal (MT1) has been reported to be one of the most reliable techniques for the correction of moderate to severe hallux deformity associated with a large intermetatarsal angle.6,11,16 However, it has the inherent risks of delayed union and malunion. 14 The proximal osteotomy of the MT1 with removal of lateral-based bone wedge is a well-known procedure for treating metatarsus primus varus.3,16 However, it shortens the MT1, which can lead to transfer metatarsalgia. 12 With the advent of instrumentation and implants, hallux valgus is managed differently in other parts of the world. In Europe, hallux valgus is being treated with percutaneous techniques by a group of surgeons. Their operative principles are the same as open surgery. Percutaneous closing wedge osteotomy of the MT1 was also developed for the treatment of severe hallux valgus. 17
The goal of this study was to determine if percutaneous basal closing wedge osteotomy of the MT1 followed by percutaneous screw fixation could achieve (1) a satisfactory degree of deformity correction without a significant increase in the rate of delayed union or malunion and (2) satisfactory clinical outcomes.
Materials and Methods
A retrospective review of all percutaneous closing wedge osteotomies performed by 2 authors (K.B.C., R.Y.) for moderate to severe hallux valgus deformity from January 2013 to December 2016 was done. All patients who had preoperative and postoperative digital dorsoplantar (DP) and lateral radiographs of the foot were included. All patients had mini-open modified McBride procedures first, then mini-open resection of the medial eminence followed by percutaneous basal closing wedge osteotomy of the MT1. Over this period, the 2 authors performed a total of 25 percutaneous basal closing wedge osteotomies in 23 patients (7 male and 16 female). The average age was 58.9 (range, 41-71) years. Absolute shortening was measured in all patients, and the relative second metatarsal shortening was measured in all patients who had no lesser metatarsal osteotomy. The follow-up period averaged 21.5 (range, 12-38) months.
Operative Techniques
All patients had mini-open modified McBride procedures first. A 1-cm incision was made over first web space to cut the adductors and lateral capsule and release the intermetatarsal ligament. Mini-open resection of the medial eminence was then performed. It was done by making 1 small incisions, one proximal and the other distal to the bunion. Care was taken to avoid injury to the dorsal medial cutaneous nerve to the hallux (Figure 1). The skin was incised. A hemostat was then used to spread the cutaneous nerve away before the capsule was opened. A periosteal elevator was used to strip the capsule from the underlying medial eminence. A space was thus created for subsequent procedures. An Isham straight flute Shannon burr (2.0 mm) was passed underneath the capsule into this space but directly over the medial bony eminence (Figure 2A). The medial bony eminence was shaved at the speed of 2500 revolutions per minute (rpm) until no bony prominence was felt or seen under fluoroscopy (Figure 2B). Saline irrigation was used to remove bony debris upon completion of the medial bony eminence resection.

Percutaneous incision for bunionectomy.
(A) Mini-open resection of the medial eminence. (B) Complete excision of the medial bony eminence by an Isham burr.
Two sets of braided polyester sutures were employed for plication of the medial capsule. For the first set of sutures, one end was pierced through the plantar distal part of the capsule using an eye needle (inside out) and exited through the skin (Figure 3A). 8 A hemostat was used to spread the cutaneous nerve away from the capsular surface. This suture end was then retrieved superficial to the medial plantar capsule but deep to the skin by the hemostat. This suture end was then pierced through the capsule (outside in) once again using the eye needle. The suture holding the plantar distal part of the capsule was then passed deep inside the capsule and retrieved at the proximal wound. Both ends of the suture were then pierced through the proximal dorsal capsule at different sites and exited through the skin. They were retrieved superficial to the capsule but deep to the skin (Figure 3B). This set of sutures was used to adduct and supinate the proximal phalanx. 8

(A) Braided polyester sutures were pierced from the plantar distal capsule through the distal bunion wound (inside out). (B) Plication of the medial capsule by the first set of braided polyester sutures. Solid red line shows suture on the plantar capsular surface while the dotted red line shows the suture underneath the capsule. (C) Plication of the medial capsule by the figure-of-8 construct. Solid red line shows the suture on the dorsal and plantar capsular surface distally while the dotted red line shows the suture underneath capsule; the lax medial capsule can be tightened.
Another set of sutures was employed. One end was pierced through the distal plantar capsule while the other end was through the distal dorsal capsule. They were also retrieved over the capsular surface but deep to skin. Both suture ends were passed deep to the capsule and retrieved from the proximal wound. The plantar suture line (holding the distal plantar capsule) was then pierced through the dorsal plantar capsule. The dorsal suture line was pierced to the plantar proximal capsule. Both suture ends were retrieved superficial to the capsule but deep to the skin again (Figure 3C), creating a figure-of-8 suture construct.
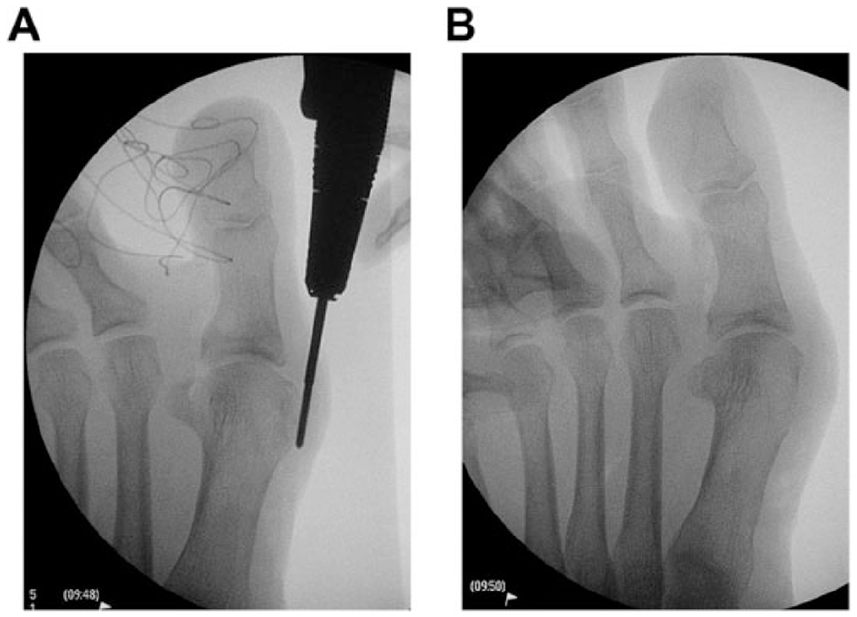
The osteotomy site (approximately 1 cm distal to the medial cuneiform–first metatarsal joint) was confirmed under fluoroscopy. An incision was made at the osteotomy site. Only the periosteum at the lateral and dorsal part of the osteotomy site was stripped with the mini-periosteal elevator. The periosteum at the medial side of the osteotomy site was left intact. An Isham straight flute Shannon burr (2.0 mm) was applied directly over the osteotomy site and drilled all the way to plantar side. The burr was then passed over the MT1 plantar-side lateral cortex first and then dorsally using the dorsal cortex of the MT1 as pivot point. A bone wedge was resected (Figure 4A). The medial cortex was left intact throughout the whole procedure. After completion of the osteotomy at the MT1 lateral side (both plantarly and dorsally), another larger diameter Isham burr (3.1 mm) was then passed through the osteotomy directly reaching the plantar side of the MT1. Slightly more bone was resected from the plantar side to achieve slight plantarflexion at the osteotomy (Figure 4B). The osteotomy was closed manually, and at the same time the first metatarsophalangeal joint was passively maximally dorsiflexed. By a windlass mechanism, the MT1 distal to the osteotomy would further be plantar flexed. A 4.0-mm headless cannulated Acutrak II screw (Acumed, United States) was passed from the dorsomedial corner of the MT1 through the osteotomy, reaching the plantar-lateral side of the MT1. At the final step, medial capsular plication was completed upon tightening both braided polyester sutures. The operative knots were tied over the joint capsule surface.

(A) A lateral bone wedge of the proximal first metatarsal was resected with an Isham burr, and the medial cortex was left intact throughout the bony procedure. (B) Slight plantarflexion was achieved at the osteotomy and fixed with guidewire for subsequent cannulated screw fixation.
Postoperative Care
A bulky dressing keeping the hallux in a corrected position was applied, and the patient was made nonweightbearing. Initial follow-up occurred 2 weeks after surgery. Nonweightbearing radiographs of the foot were obtained at 2, 4, and 6 weeks after surgery to assess osteotomy alignment and signs of healing (Figure 5). Patients’ full weightbearing walking was started after the 6-week postoperative visit (Figure 6).

Callus formation at the osteotomy 4 weeks postoperatively.

Left foot correction 9 months postoperatively.
Radiographic Measurements
All measurements were made by the senior author using the angle measurement software provided by the digital radiographs. The pre- and postoperative hallux valgus (HV) angle, intermetatarsal (IM) angle, and relative shortening of the MT1 were determined according to the methods suggested by Day et al. 4 Absolute shortening was determined as the difference in the distance from the subchondral bone at the proximal articular surface to the subchondral bone at the first metatarsal head between the preoperative and postoperative radiographs. Relative shortening was evaluated in patients without additional lesser metatarsal osteotomy by drawing a line connecting the most distal portion of the first and third metatarsal head. The distance from this line, as it crossed the second metatarsal shaft, to the most distal portion of the second metatarsal head was taken as the relative shortening of the MT1. In addition, the position of the medial sesamoid, both pre- and postoperatively, was classified with the grading system described by Hardy and Clapham. 7 The position of the medial sesamoid with reference to the longitudinal axis of the MT1 was also assessed in the following manner: in grade I, the medial sesamoid was situated medial to the MT1 longitudinal axis, while in grade VII, it was lateral to the MT1 longitudinal axis. The time from surgery to radiographic evidence of callus formation at the osteotomy site and the time to from surgery to radiographic evidence of trabeculations crossing the osteotomy site were documented. All the preoperative radiographic measurements were made on weightbearing anteroposterior (AP) radiographs. The postoperative radiographic measurements were made on the weightbearing AP radiograph at the latest follow-up.
Clinical Assessments
Clinical assessments before and after surgery included the presence of plantar callosity tenderness at the plantar aspect of the second metatarsophalangeal joint (MTP) joint (transfer metatarsalgia) and the American Orthopaedic Foot & Ankle Society (AOFAS) score.
Statistical Analysis
Statistical analysis was carried out using SPSS (version 20; SPSS, Inc, an IBM Company, Chicago, IL). The Wilcoxon signed-rank test was used for continuous variables, including preoperative and postoperative measurement, whereas the Fisher exact test was used for categorical variables. Statistical significance was determined from a 2-tailed test with P < .05.
Results
Two patients had bilateral operations. An additional operation of the second metatarsal (Weil’s osteotomy) was performed during the same operation in 4 of 23 patients, DuVries excisional arthroplasty of second toe proximal interphalangeal joint in 5 of 23 patients, and an additional percutaneous osteotomy of the first proximal phalanx (percutaneous Akin) in 4 of 23 patients.
The mean HV angle improved from 39.4 (range, 29-58.3) degrees before the operation to 14.7 (range, 0.1-23.2) degrees after operation (P < .05). The mean IM angle improved from 14.9 (range, 6.7-22.4) degrees before the operation to 6.6 (range, 0.9-14.8) degrees after the operation (P < .05). The average absolute shortening was 3.8 mm (range, 0.27-12.91 mm) and the relative shortening was 0.8 mm (range, 0.05-1.91) (Table 1). The average time for detection of callus formation and trabeculations at osteotomy was 4 and 6 weeks, respectively. The sesamoid position after the operation in nearly 90% of feet was classified grade IV or below (Table 2). 7 This result was statistically significant (P < .05). There was no transfer metatarsalgia in any patients after the operation. Fifteen patients with plantar callosity at the second MTP joint prior to surgery had resolution of callosity after the operation. One patient with multiple plantar callosities had resolution of 3 of 4 callosities. The AOFAS score improved from 39 (range, 12-50) preoperatively to 81 (range, 70-93) postoperatively (P < .05).
Relative and Absoulte Shortening After Basal Osteotomy of First Metatarsal.

Position of Medial Sesamoid.

Complications
One patient had mild permanent numbness over the medial side of the big toe. Another patient had a superficial infection at the bunion wound that was treated successfully with antibiotics alone.
Discussion
The use of percutaneous basal osteotomy of the MT1 for the correction of moderate to severe hallux valgus deformity is quite popular in Europe, especially France, Spain, and Italy. This technique has evolved from the first generation (osteotomy held in position by dressing alone without internal fixation) 1 to the third generation (percutaneous osteotomy with stable fixation of the osteotomy with screws). 2 Despite the popularity of this technique, only a few studies have documented its ability to correct the IM and HV angles, produce good patient outcomes, and avoid complications.9,17
In the current study, the average HV and IM angle correction was 24.8 degrees and 8.4 degrees, respectively, and the mean postoperative AOFAS score was 81. The effectiveness of the procedure as determined by angular correction and the clinical outcomes in the current study are similar to those of previous percutaneous and open studies. In 2016, in treatment of severe hallux valgus by European surgeon 17 who had reviewed his percutaneous basal osteotomy of MT1 showing that the average correction of HV and IM angles were 22.8 degrees and 6 degrees. A study of percutaneous basal closing wege osteotomy in treatment of severe hallux valgus found that the average correction of HV and IM angles was 22.1 and 6.5 degrees, respectively. 12 Another study of open basal closing wege osteotomy in 2011 found that the correction to be 20 and 8.8 degrees, respectively. 4
Proximal closing wedge osteotomy has always been criticized for shortening of the first ray, which subsequently led to transfer metatarsalgia. It was suggested that absolute shortening within 4 mm was acceptable. 3 Using the method of measurement as suggested by Day et al, 4 in our 23 patients (25 feet), the average absolute shortening was 3.8 mm (range, 0.27-12.91 mm) and the relative shortening was 0.8 mm (range, 0.05-1.91 mm), which were comparable to their results (2.2 mm and 0.6 mm) and fell within the range as suggested. 3 We agree with the suggestion that with basal closing wedge osteotomy, the MT1 was actually rotated parallel to the second metatarsal (MT2), and thus the MT1 was actually relatively lengthened. 4
Slightly more bone was resected on the plantar side at the osteotomy of the MT1. Slight plantarflexion at the osteotomy could be achieved to avoid dorsiflexion malunion. 4 We shared their concept, and our percutaneous basal osteotomy was done in a similar manner. A larger diameter burr was passed directly to the plantar osteotomy site. Slightly more bone was resected on the plantar side. The osteotomy was gently plantarflexed further manually and then fixed with a headless cannulated screw percutaneously. We believe that slight plantarflexion at the osteotomy explains the absence of transfer metatarsalgia in our patients. However, limitations in our study were the small sample size and short follow-up. Further biomechanical study has to be conducted to understand the relationship between the degree of plantar flexion at the osteotomy of the MT1 with corresponding changes in forefoot plantar pressure at different rays.
For percutaneous bone shaving or osteotomy, the speed of the burr must be not too fast (2000 to 8000 rpm, to avoid burning of the surrounding skin around the incision), and the torque provided by the power instrument should be strong enough to accomplish its task. As the flute of the Isham burr is not helical, there will be bone paste left behind after bone shaving, which will act as a bone graft to hasten bony union.
Caution should be exercised when doing percutaneous basal osteotomy as the burr was in close proximity to dorsalis pedis. During the basal percutaneous osteotomy, the burr was in close proximity to the dorsalis pedis vessel, which passes directly into the interval between the base of the MT1 and MT2 and then all the way to the plantar side. As the osteotomy was approximately 1 cm distal to the first tarsal-metatarsal joint, the Isham burr should be kept close to the base of the MT1 to minimize the chance of vascular injury. Detailed cadaveric study of this vessel should be done to minimize iatrogenic injury. 5
The importance of sesamoid position preoperatively and postoperatively should be elaborated. From a classical textbook description, it was believed that plication of the medial capsule helps to restore the capsulo-ligamentous structures around the first MTP joint and may partly help on reduction of sesamoid position. 10 A study of postoperative sesamoid position showed that incomplete reduction of sesamoid is a risk factor. 13 In our techniques, a mini-open resection of medial eminence was done. The medial capsule was not exposed as wide as in the open technique. We believed that by using 2 sets of braided polyester sutures for medial capsular plication, a similar effect could be achieved. This could be reflected in our comparison between the sesamoid position pre- and postoperatively (Table 2) in which nearly 90% of the medial sesamoid was classified grade IV or below. 7 As suggested by Lui et al, 8 the first set of braided polyester sutures pierces through the distal plantar capsule supinates and adducts the proximal phalanx on the MT1, while the second set, placed in figure-of-8 manner, tightens the lax medial capsule further. However, complications like medial side numbness were seen in our series. As our average follow-up was short, a longer follow-up was needed to assess the sesamoid position and recurrence.
Conclusions
Satisfactory HV angle correction, IM angle correction, and patients’ clinical outcomes can be achieved with a percutaneous basal closing wedge osteotomy fixed with percutaneous screw. There was no malunion or delayed union in this series.
Footnotes
This article was originally published as: Chan KB, Yeung R. Percutaneous basal closing wedge osteotomy of the first metatarsal in the treatment of moderate to severe hallux valgus and its short-term clinical outcomes. Foot Ankle Orthop. 2017 Apr 11;3(1):2473011417748895. doi:10.1177/2473011417748895.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.