
Abstract
Background:
Ankle arthrodesis is an established treatment for ankle arthritis. For patients with ankle arthritis, the position of the talus during ankle arthrodesis may affect the radiographic parameters of the foot. The purpose of this study is to assess the radiographic relationship between talar alignment and the longitudinal arch of the foot before and after ankle arthrodesis.
Methods:
We retrospectively reviewed a single-surgeon series of 30 patients who had undergone ankle arthrodesis. Measured parameters included the lateral tibiotalar angle (LTTA), lateral talometatarsal angle (LTMA), lateral talocalcaneal angle (LTCA), cuneiform height (CH), and calcaneal pitch (CP). Additional data collected included demographics, fusion construct type, and visual analog scale (VAS) measurements.
Results:
LTTA was increased from 68.2 ± 7.4 degrees preoperatively to 75.0 ± 6.4 degrees postoperatively (P = .001), LTMA increased from −2.0 ± 10.7 degrees to 4.0 ± 10.1 degrees (P < .001), CH increased from 20.1 ± 7.5 mm to 26.1 ± 8.4 mm (P < .001), LTCA and CP had no statistically significant change. VAS score decreased from 5.7 ± 2.7 to 1.3 ± 1.9 (P < .001).
Conclusion:
Correcting the talar alignment in the sagittal plane during ankle arthrodesis improved the radiographic parameters of the foot, contributing to restoration of the longitudinal arch. The clinical significance of these findings is that in patients undergoing ankle arthrodesis, the surgeon should be aware that the alignment of the foot will be altered at the time of ankle arthrodesis and should be considered in preoperative planning. Further research is needed to determine the effect of ankle arthrodesis in patients determined to have pes planus preoperatively.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Ankle arthrodesis is an established treatment for ankle arthritis.1,8,13,18,28 It has been shown that alignment of the ankle at the time of arthrodesis is important.12,26 Literature discussing alignment of the ankle has been in the context of coronal and sagittal planes, and establishing an anatomically neutral ankle joint.9,26 It has been recommended to place the arthrodesis at neutral dorsiflexion/plantarflexion within the sagittal plane relative to the plantar aspect of the foot.4,9,21 Studies discussing talar declination angle recommend correcting the talar declination angle to 25 degrees.5,6,24 Excess dorsiflexion is thought to cause heel overload whereas excess plantarflexion can result in a back-knee thrust and vaulting gait pattern. 8
In patients with pes planus, the talus is relatively plantarflexed relative to the tibial axis.10,17,25 In addition to this increased talar declination angle, these patients often have a decreased cuneiform height (CH) and increased lateral talometatarsal angle (LTMA).10,14,20,29 It is unclear how these measurements change with ankle arthrodesis, particularly with relation to a change in the talar position after an ankle arthrodesis. Sealey et al 26 demonstrated that there is an inverse association between the calcaneal pitch angle and the sagittal range of motion following an ankle arthrodesis. This is important following ankle arthrodesis, because flexibility through the foot has been shown to have a positive correlation with patient function and satisfaction. 19 Furthermore, quality of life has been positively associated with increased compensatory motion of the hindfoot and midfoot after ankle arthrodesis. 26
An important consideration during ankle arthrodesis is the position of the talus relative to the tibia. In patients with a plantarflexed talus, correcting this deformity with the ankle arthrodesis may correct the longitudinal arch.
To our knowledge, few have assessed the relationship between ankle position and the longitudinal arch of the foot. We hypothesize that dorsiflexing the talus while performing an ankle arthrodesis will improve the sagittal alignment of the foot, helping to restore the longitudinal arch. The purpose of this study is to assess the relationship between ankle position in the sagittal plane and the longitudinal arch of the foot before and after ankle arthrodesis.
Methods
Patients who underwent an ankle arthrodesis were retrospectively examined in this single-institution, single-surgeon study from January 2015 through December 2021. Inclusion criteria consisted of patients 18 years of age or older undergoing isolated ankle arthrodesis. Patients excluded were those with prior or additional subtalar arthrodesis, prior or additional midfoot reconstruction, structural complications after arthrodesis, lack of adequate radiographs, or lack of 6-month follow-up. Twenty-seven patients met the inclusion criteria.
Preoperative and 3-month postoperative radiographic measurements were obtained utilizing the Merge Unity, version 11.0 (Merge Healthcare, Hartland, WI) picture archiving and communication system. Radiographic measurements obtained on weightbearing radiographs included the following: lateral tibiotalar angle (LTTA), lateral talometatarsal angle (LTMA), lateral talocalcaneal angle (LTCA), cuneiform height (CH), and calcaneal pitch (CP) as described previously in the literature (Figure 1).7,8,11,22,27 Patient charts were reviewed for age, sex, body mass index (BMI), comorbidities including diabetes, smoking status, fusion construct type, complications, and visual analog scale (VAS) scores.
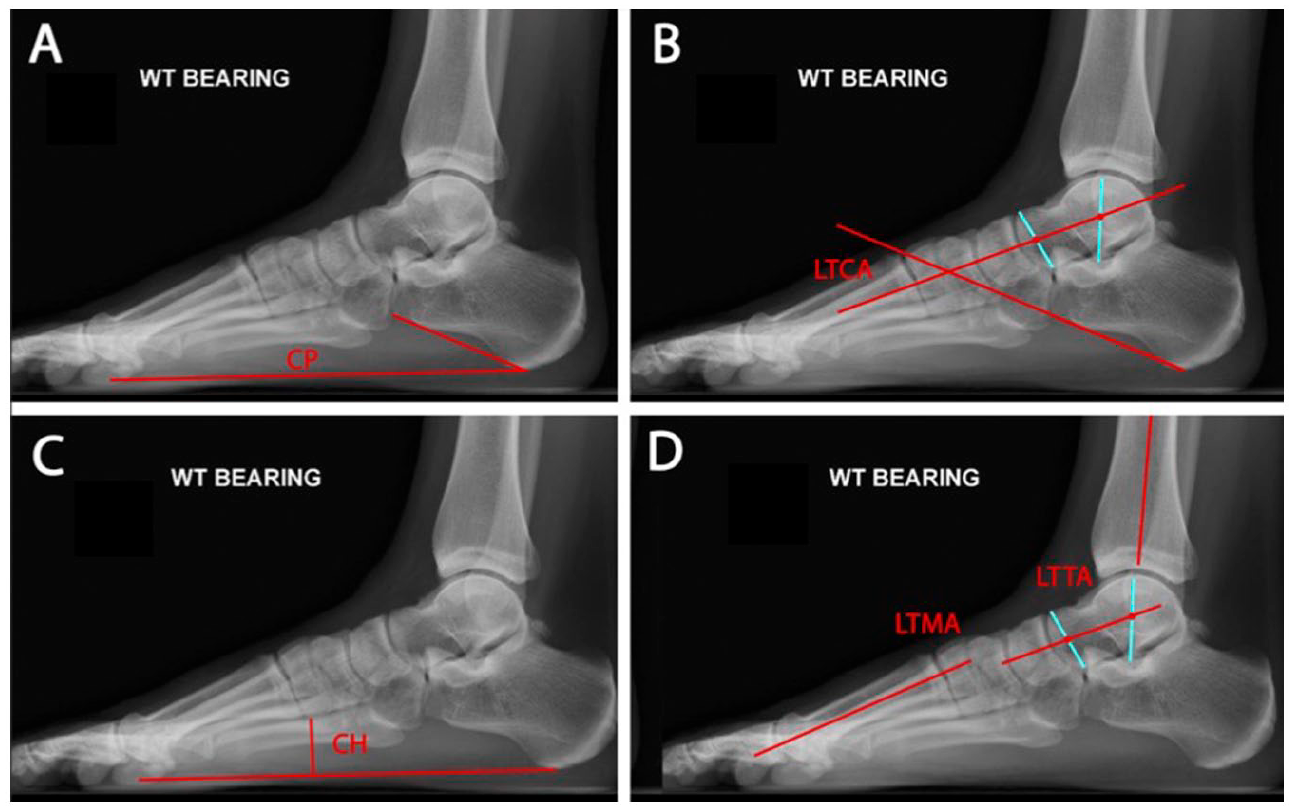
Example radiographic measurements of (A) calcaneal pitch, (B) lateral talocalcaneal angle, (C) cuneiform height, and (D) lateral talometatarsal angle and lateral tibiotalar angle.
Statistical Analysis
Descriptive and comparative statistics including mean, SD, percentage, and t tests were calculated where appropriate. t test was calculated using a paired 2-tailed t test within Microsoft Excel. Statistical significance was set at P <.05.
Results
A summary of the demographics is shown in Table 1. The average age was 58.0 ± 11.0 years with a range from 31 to 78 years old. Males accounted for 16 of the 27 patients included and 11 of 27 had the left ankle operated on. The average BMI was 33.1 ± 5.8 with a range of 24.0 to 44.3. Only 1 of 27 patients was diabetic. Smokers accounted for 5 of 27 patients, whereas the rest were former or never smokers. Various constructs were used for the arthrodesis. Interfragmentary screws alone in 13 patients, interfragmentary screws with plate augmentation in 7 patients, and anterior compression plating in 7 patients.
Demographic Information of Patients Undergoing Tibiotalar Arthrodesis.

On radiographic examination, the LTTA was increased from 68.2 ± 7.4 degrees preoperatively to 75.0 ± 6.4 degrees postoperatively (P = .001), LTMA increased from −2.0 ± 10.7 degrees to 4.0 ± 10.1 degrees (P < .001), LTCA measured 43.2 ± 10.3 degrees preoperatively to 44.0 ± 6.0 degrees postoperatively (P = .555), CH increased from 20.1 ± 7.5 mm to 26.1 ± 8.4 mm (P < .001), and CP measured 21.8 ± 8.1 degrees preoperatively to 23.6 ± 6.2 degrees postoperatively (P = .146). Table 2 provides a summary of the radiographic measurements pre- and postoperatively. The range of the LTTA 45 to 79 degrees condensed to 64 to 77 degrees, LTMA −36 to 21 degrees condensed to −24 to 31 degrees, CH 1 to 38 mm increased to 1 to 48 mm, LTCA 12 to 66 degrees condensed to 32 to 63 degrees, and CP 7 to 44 degrees condensed to 13 to 38 degrees. VAS scores decreased from 5.7 ± 2.7 to 1.3 ± 1.9 (P < .001). Average follow-up was 12.4 months.
Summary of Radiographic Measurements Pre- and Post-operatively.

Complications in our study were present in 6 patients. One patient underwent hardware removal 1.5 years postoperatively because of hardware irritation. The pain resolved following removal. One patient had a nonunion demonstrated on CT scan that underwent a revision arthrodesis and was excluded. One patient underwent 2 revision surgeries for a chronic wound and saphenous nerve neuroma. One additional patient had a saphenous nerve neuroma that was excised 2 months postoperatively. One patient developed a postoperative infection that required incision and drainage hardware removal, antibiotic spacer placement, and eventual tibiotalocalcaneal fusion and was excluded. The last patient sustained a periprosthetic fracture at the proximal end of the anterior plate after jumping out of a moving vehicle on postoperative day 3. This patient subsequently underwent surgical fixation with an additional anteromedial plate and went on to successful fusion. This patient was excluded.
Discussion
This study demonstrates that lateral radiographic parameters were improved with ankle arthrodesis. By correcting the talar alignment during ankle arthrodesis, the sagittal plane alignment improved, contributing to restoration of the longitudinal arch. The clinical significance of these findings is that in patients undergoing ankle arthrodesis, the surgeon should be aware that the longitudinal arch can be corrected at the time of ankle arthrodesis. The LTTA in the current study increased by 6 degrees on average. The LTMA improved nearly 6 degrees. The normal angle is 0 ± 10 degrees whereas patients with pes planus often are >20 degrees apex plantar. 29 The arch height measured by the CH changed significantly, which indicates that the longitudinal arch was restored. The CP and LTCA did not have a significant change. All but the CH range condensed following arthrodesis. This points to improved correction of patients with worse deformities as the ankle joint is placed in the optimal position for arthrodesis. Figure 2 demonstrates this change. These changes likely do not meet clinical significance as a whole, but the patients with more severe deformities achieve greater correction and potentially benefit more from the procedure.

(A, B) Preoperative and (C, D) 3 year postoperative lateral radiographs in patients who underwent isolated ankle arthrodesis. Note the improvement of the medial cuneiform height.
This study is especially important to consider as ankle arthritis and pes planus can happen concurrently. When ankle arthritis is thought to be secondary to pes planus, it is considered stage IV pes planus.2,3,16,23,25,28 Evidence is limited to case series and expert opinion regarding stage IV pes planus treatment outcomes because of the rarity of progression. 15 Numerous treatment options have been used to address symptomatic pes planus. Many of these are used in combination with surgical options addressing the tibiotalar joint depending on rigidity of the deformity. 15 If the surgeon is able to correct the talonavicular sag with isolated ankle arthrodesis, this may avoid additional surgical procedures and the potential complications or morbidity that result.
This study has several limitations. First, this study was retrospective, which does not allow us to conclude causal relationships. Second, the study has a small sample size, which limits generalizability. Third, there was no intent to correct the sagittal alignment at the time of surgery through the ankle arthrodesis. Fourth, the surgical construct varied throughout the study period. However, the results did show consistent radiographic changes from all constructs. Fifth, the only clinical outcome measure utilized was the VAS score, and more detailed outcome scores is a potential future research objective.
Conclusion
Correcting the talar alignment at the time of ankle arthrodesis improved the lateral radiographic parameters of the foot, contributing to the restoration of the longitudinal arch. The clinical relevance of these findings is that in patients undergoing ankle arthrodesis, the longitudinal arch can be corrected with positioning of the talus at the time of ankle arthrodesis. Future research could focus on the benefits to patient with pes planus undergoing ankle arthrodesis.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114231187888 – Supplemental material for Radiographic Measurements of the Foot and Ankle After Ankle Arthrodesis
Supplemental material, sj-pdf-1-fao-10.1177_24730114231187888 for Radiographic Measurements of the Foot and Ankle After Ankle Arthrodesis by Jordan Boivin, Christopher Traynor, Kevin Stehlik and James Jastifer in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
IRB Exempt Status from WMED IRB: WMED-2021-0790. Reason: “meets the criteria for exempt status as described in 45 CFR Part 46.104 (d) Category 4(iii): Secondary research uses of identifiable private information if the research involved only information collection and analysis involving the investigator’s use of identifiable information when that use is regulated under 45 CFR parts 160 and 164, subparts A and E [HIPAA], for the purposes of "health care operations" or "research" as those terms are defined at 45 CFR 164.501.”
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.