
Abstract
Background:
Percutaneous ankle fusion is an emerging technique with minimal published outcome data. The goal of the present study is to retrospectively review clinical and radiographic outcomes following percutaneous ankle fusion and provide technique tips to perform percutaneous ankle fusion.
Methods:
Patients >18 years of age, treated by a single surgeon, from February 2018 to June 2021, who underwent primary isolated percutaneous ankle fusion supplemented with platelet-derived growth factor B (rhPDGF-BB) and beta-tricalcium phosphate, with at least 1-year follow-up were included. Surgical technique consisted of percutaneous ankle preparation followed by fixation with 3 headless compression screws. Pre- and postoperative visual analog scale (VAS) and Foot Function Index (FFI) were compared using paired t tests. Fusion was assessed radiographically by the surgeon on postoperative radiographs and computed tomography (CT) at 3 months postoperatively.
Results:
Twenty-seven consecutive adult patients were included in the study. Mean follow-up was 21 months. Mean age was 59.8 years. Mean preoperative and postoperative VAS scores were 7.4 and 0.2, respectively (P < .01). Mean preoperative FFI pain domain, disability domain, activity restriction domain, and total score were 20.9, 16.7, 18.5, and 56.4, respectively. Mean postoperative FFI pain domain, disability domain, activity restriction domain, and total score were 4.3, 4.7, 6.7, and 15.8, respectively (P < .01). Fusion was achieved in 26 of 27 patients (96.3%) at 3 months. Four patients (14.8%) had complications.
Conclusion:
We found in this cohort with surgery performed by a surgeon highly experienced in minimally invasive surgery that percutaneous ankle fusion augmented with a bone graft supplement achieved a high rate of fusion (96.3%) and a significant improvement in pain and function postoperatively while associated with minimal complications.
Level of Evidence:
Level IV, case series.
Background
The main indication for ankle fusion is pain and deformity of the ankle joint secondary to multiple etiologies including trauma, infection, avascular necrosis, failed arthroplasty, or malalignment. Ankle fusions are often performed as open, arthroscopic, or via miniarthrotomy. 6 In a traditional open intervention, larger incisions may increase the risk of infection, wound dehiscence, and might negatively impact bone healing because of the more extensive soft tissue stripping. Conversely, arthroscopic techniques use small portals, thereby decreasing soft tissue insult and minimizing complications. 16 Nonetheless, it is a more technically challenging technique for surgeons who are not comfortable with ankle arthroscopy. Percutaneous fusion technique benefits from even smaller portals than arthroscopy and does not require the use of an arthroscope to complete the procedure. However, as the technique is relatively new, there is a paucity of data on the outcomes of percutaneous fusion.
Recent literature on percutaneous techniques includes a comparison of minimally invasive joint preparation versus open techniques in a cadaver model. Zhao et al 17 prepared cadaveric ankles using transcutaneous and open techniques and compared the percentage of the joint surface prepared in various joints of the foot and ankle. Although not statistically significant, there was a trend toward an increase in joint surface preparation using the percutaneous method. In another earlier study by Lauge-Pedersen, percutaneous ankle fusion was performed in 10 patients with rheumatoid arthritis with severe ankle arthritis. This technique resulted in bony fusion in all patients with all patients claiming to be satisfied and pain free. 9
To our knowledge, this is the first study to report on outcomes following percutaneous ankle fusion in an expanded cohort of patients.
Methods
Consecutive patients aged >18 years, treated by a single surgeon, from February 2018 to June 2021, who underwent isolated primary percutaneous ankle fusion, with at least 1-year follow-up were included in this study. Inclusion criteria were end-stage ankle arthritis in patients who were not candidates for arthroplasty or opted for primary fusion, as well as foot drop not eligible for a tendon transfer. Exclusion criteria included patients with an active infection, uncontrolled diabetes (HbA1c > 8.5%), and open pilon fractures. Patients requiring concomitant hindfoot fusion or supramalleolar procedures were excluded. Fusion was assessed radiographically by the operating surgeon on postoperative radiographs obtained at each visit, as well as computed tomography (CT) at 3 months postoperatively in all patients. Fusion was defined as at least 75% bone bridging on the coronal and sagittal cuts of the CT. Pre- and postoperative patient-reported outcomes were assessed with visual analog scale (VAS) and Foot Function Index (FFI). Data analysis was performed using GraphPad Prism version 9.4.1 for macOS (San Diego, CA, USA). Descriptive statistical analysis was performed on all variables, yielding frequency and percentages for categorical variables, and mean, SD, and ranges for continuous variables. Fisher exact test was used to determine association between categorical variables. A P value ≤.05 was considered to be statistically significant.
Surgical Procedure
The patient was placed supine with the surgical foot at the edge of the table and ipsilateral hip bumped so the operative ankle sagittal plane was directly perpendicular to the floor. The contralateral leg was positioned to avoid interference with the mini C-arm. In order to prevent the risk of heat necrosis or thermal injury to soft tissues and bone, copious saline irrigation via bulb syringe was used without the use of a thigh tourniquet.
A percutaneous Achilles tenotomy in patients with a fixed equinus contracture was completed first. Next, 3-mm anteromedial and anterolateral portals (in the same location as those used for ankle arthroscopy) accessing the ankle joint were established. A 3 × 30-mm cutting burr was advanced in either of the 2 portals and activated inside the joint debriding the tibia from posterior to anterior (Figure 1). Fluoroscopy was used repeatedly to confirm position of the burr. A wedge burr can be used for further debridement. The same steps were performed on the talus and medial gutter (Figure 2) through the same portals. A small curette was used to check the joint for remaining cartilage. As needed, further debridement of the ankle can be completed by using a curette, dental rasp, or pituitary rongeur.

Intraoperative image demonstrating debridement with the burr.

Intraoperative image demonstrating medial gutter debridement.
The joint was then fenestrated with a 2-mm wire advanced through the portals from posterior to anterior to stimulate bony healing and fusion. Bone graft substitute including platelet-derived growth factor B homodimer (rhPDGF-BB) with a bioresorbable synthetic bone matrix (beta-tricalcium phosphate (β-TCP) (Wright Medical Augment) was injected into the joint.
After joint preparation, the ankle was aligned in neutral flexion, mild valgus (<5 degrees), and 5 degrees of external rotation and stabilized with guidewires for two 7-mm headless compression screws from proximo-medial to distal-lateral, and 1 headless compression screw (5- or 7-mm) from proximo-lateral to distal medial. Patients were kept nonweightbearing in a splint for 2 weeks, followed by nonweightbearing in a CAM boot for 4 weeks, then allowed weightbearing as tolerated in a CAM boot for another 6 weeks.
Results
Twenty-seven adult patients (44% male/66% female) were included in the study. Mean patient characteristics are reported in Table 1. Mean follow-up was 21 months (range, 13-31 months). Mean age was 59.8 years (range, 39-89 years). Medical comorbidities included diabetes (3/27), smoking (1/27), rheumatoid arthritis (3/27), lupus (1/27), pilon fractures (2), and paralytic foot (3/27).
Patient Descriptive Data.

Mean preoperative and postoperative patient-reported outcomes are detailed in the Figures 3 and 4 and Tables 2 and 3. Statistically significant differences between pre- and postoperative VAS scores and all FFI domains were found. Mean preoperative and postoperative VAS scores were 7.4 and 0.2, respectively (P < .01). Mean preoperative FFI pain domain, disability domain, activity restriction domain, and total score were 20.9, 16.7, 18.5, and 56.4, respectively. Mean postoperative FFI pain domain, disability domain, activity restriction domain, and total score were 4.3, 4.7, 6.7, and 15.8, respectively. All pre- and postoperative differences in FFI were statistically significant (P < .01). Fusion was achieved in 26 of 27 patients (96.3%) at 3 months (Figures 5 and 6). Four patients (14.8%) had complications: a nonunion in a diabetic patient successfully converted to a tibiotalocalcaneal nail; 1 hardware removal for symptomatic hardware; superficial wound dehiscence; and transient superficial peroneal neuritis that resolved 4 months postoperatively without intervention (Table 3).

Pre- and postoperative Foot Function Index (FFI) domain scores.

Pre- and postoperative Foot Function Index (FFI) total score.
Patient-Reported Outcome Scores.

Abbreviation: FFI, Foot Function Index.
Complications Description and Resolution.

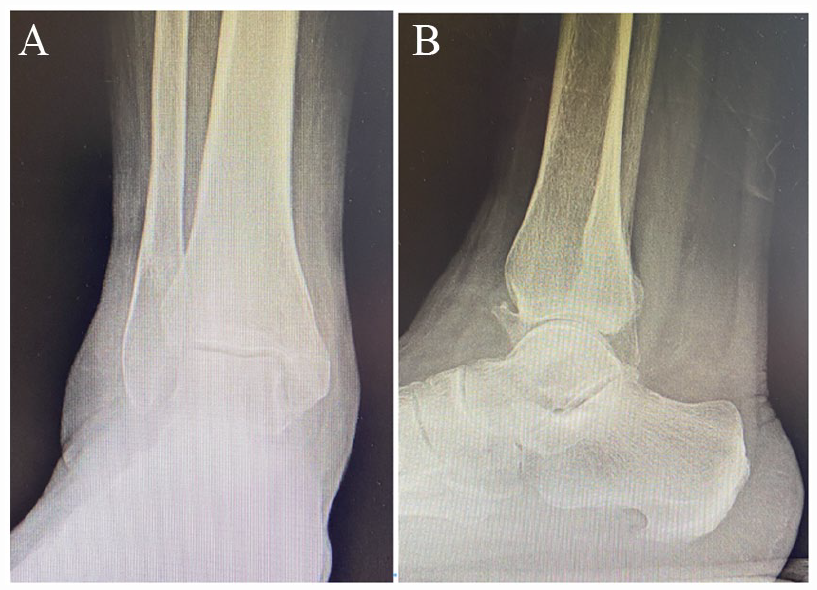
Preoperative anteroposterior (A) and lateral (B) ankle radiographs in a 79-year-old man undergoing ankle fusion for paralytic foot drop secondary to lower spine surgery complications.
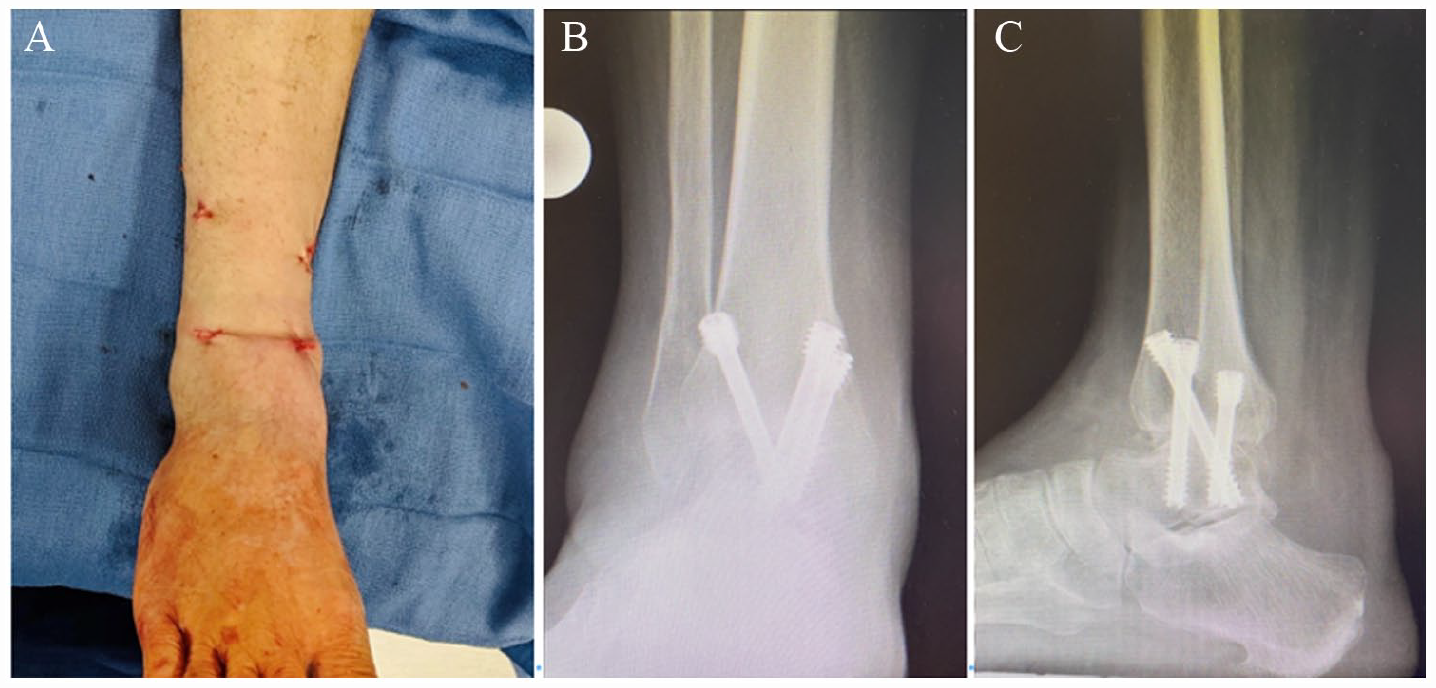
Postoperative ankle incisions (A), and anteroposterior (B) and lateral (C) ankle radiographs 3 months after surgery demonstrating completed ankle fusion.
Discussion
This retrospective study found significant improvements in all patient-related measures and nearly all patients achieved fusion with few complications. When evaluating these results against the literature for more invasive ankle fusion techniques, the rate of fusion is similar or better depending on the study. Fusion rates for ankle arthrodesis have been reported between 39% and 100% depending on technique, indication, and patient population.2,3,7,12,13,18 Similarly, a total complication rate of 14.8% reported in this study is approximately the same with current literature on both open and arthroscopic techniques. 12
In the absence of significant literature on percutaneous ankle fusion, we suspect that the technique more closely resembles arthroscopic ankle fusion as they share many similar advantages. Therefore, we present a brief summary of the large quantity of arthroscopic ankle fusion literature. Overall, the literature suggests significant advantages in arthroscopic over open fusion including decreased time to union, diminished postoperative pain, comparable union rates (to open fusion), shorter hospital stays, decreased blood loss, shorter tourniquet times, and earlier patient mobilization.4,5,10,11,14,15 In a recent meta-analysis of 1102 patients from 18 studies that included 15 randomized control trials and 3 retrospective cohort studies, Bai et al 2 found arthroscopic assisted fusion had a higher rate of fusion, shorter fusion time, less intraoperative blood loss, shorter hospital stay, and improved VAS scores. Arthroscopic fusion rates were reported as high as 100% and as low as 79%, whereas open fusion rates have been reported as high as 100% and as low as 39%. 2 A similar meta-analysis comparing open versus arthroscopic fusion reported improved fusion rates and shorter length of stay in arthroscopic fusion. 7 Complications in arthroscopic ankle fusion have been reported with varying results as some authors present a decrease in all complications and infections with others finding no differences in infection or overall complication rate when comparing arthroscopic vs open ankle fusion.1,2,7
Theoretically it is likely arthroscopic technique benefits from less insult to soft tissues and copious amounts of irrigation that help reduce infection rate and wound-related complications, which the current study technique benefits from as well with even smaller portals and continuous irrigation throughout the procedure. Complications after arthroscopic ankle fusion that have been reported include nonunion, deep infections, lymphedema, neuropraxias, and adjacent joint degeneration. 8 These reported complications appear consistent with those of the current study.
Although we did not perform a comparative study the results of the current study suggest that the percutaneous technique in experienced hands with use of supplemental bone graft substitute may be equivalent or perhaps even better than arthroscopic ankle fusion. The authors feel that the study technique has the advantage over traditional arthroscopy of decreased equipment set up. The percutaneous technique does not require an arthroscopy tower and specialized arthroscopic instruments. The necessary equipment for the percutaneous technique is a reusable burr device with exchangeable burr tips.
This initial report on 27 patients is the largest cohort to date to demonstrate that percutaneous ankle fusion with a specific bone graft substitute can improve patient outcomes comparable to those observed with arthroscopic ankle fusions without an increase in complications. However, this study does have weaknesses. It is a retrospective single cohort study without a comparative or control group. All surgeries were performed by a single, experienced surgeon familiar with the technique and therefore results may not be generalizable to less experienced surgeons. The selection and use of the grafting material that included a biologically active agent and specialized carrier may have had an additional positive effect we were unable to quantify. Additional studies should be performed to evaluate percutaneous ankle fusion compared to arthroscopic fusion without the presence of bone graft or with the exact same grafting material in equally experienced surgical hands and comorbid patients.
Conclusion
Percutaneous ankle fusion with the bone graft supplement used herein was associated with a high fusion rate (96.3%), and with mostly minor complications. Pre- and postoperative patient-reported outcomes suggest high patient satisfaction with the procedure.
Footnotes
Ethical Approval
This study was completed with IRB approval.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ettore Vulcano, MD, reports royalties or licenses from Novastep. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.