
Abstract
Background:
Following below-knee surgery, the optimal medical mobility device remains controversial as adequate nonweightbearing of the operated extremity is critical to ensure successful healing. The use of forearm crutches (FACs) is well established but requires using both upper extremities. The hands-free single orthosis (HFSO) is an alternative that spares the upper extremities. This pilot study compared functional, spiroergometric, and subjective parameters between HFSO and FAC.
Methods:
Ten healthy (5 females, 5 males) participants were asked to use HFSOs and FACs in a randomized order. Five functional tests were performed: climbing stairs (CS), an L-shaped indoor course (IC), an outdoor course (OC), a 10-meter walk test (10MWT), and a 6-minute walk test (6MWT). Tripping events were counted while performing IC, OC, and 6MWT. Spiroergometric measurements consisted of a 2-step treadmill test with speeds of 1.5 and 2 km/h, each for 3 minutes. Lastly, a VAS questionnaire was completed to collect data regarding comfort, safety, pain, and recommendations.
Results:
Significant differences between both aids were observed in CS and IC (HFSO: 29.3 seconds; FAC: 26.1 seconds, P < .03; and HFSO: 33.2 seconds, FAC: 18 seconds, P < .001, respectively). The other functional tests showed no significant differences. The trip events were not significantly different between the use of the 2 aids. Spiroergometric tests showed significant differences regarding heart rate (HFSO: 131.1 bpm at 1.5 km/h and 131 bpm at 2 km/h; FAC: 148.1 bpm at 1.5 km/h and 161.8 bpm at 2 km/h) and oxygen consumption (HFSO: 15.4 mL/min/kg at 1.5 km/h and 16 mL/min/kg at 2 km/h; FAC: 18.3 mL/min/kg at 1.5 km/h and 21.9 mL/min/kg at 2 km/h) at both speeds (all P < .01). In addition, significantly different ratings regarding the items comfort, pain, and recommendation were recorded. Both aids were equally rated for safety.
Conclusion:
HFSOs may be an alternative to FACs, especially in activities that require physical stamina. Further prospective studies in patients with below-knee surgical intervention concerning everyday clinical use would be interesting.
Level of Evidence:
Level IV pilot-study.
Introduction
After foot and ankle surgery, a nonweightbearing status is often necessary to achieve optimal healing.
12
Records on walking aids date back to 2830
Furthermore, pain in the upper extremities due to the overuse of crutches is common and can lead to further injuries. In addition, crutches do not prevent patients from placing their weight on the operated limb and make it hard to walk on.10,22 Moreover, the feeling of immobility or insufficient mobility can have psychological effects, which in turn, delays the healing process. 22 Other auxiliaries have been developed to overcome these limitations, often based on wheels, have been developed, including already established ones such as the wheelchair or modern variants such as the knee scooter. However, these have the disadvantage that they are relatively large aids and thus require appropriate space for maneuvering. Moreover, obstacles such as stairs cannot be overcome without assistance.5,12,16,26 An alternative that combines unloading without crutches and high mobility is an HFSO (Figure 1) that promises higher patient satisfaction and comfort.12,17 The mode of action of such an orthosis is based on the orthosis being applied with the knee bent at 90 degrees on the affected operated side. This places the weight on the thigh, enabling nonweightbearing at the lower leg or foot to be achieved (Figure 2). We aimed to examine if there are differences between HFSO and FAC in terms of functional and spirometric parameters. In addition, we wanted to assess the participants' subjective evaluations, such as safety in using the aid or preference for one of the 2 aids, using a VAS questionnaire.

Hands-free single crutch iWALK 2.0 (iWALKFree, Inc, Long Beach, CA).

Image of the IWalk 2.0 in the worn state. Note the 90-degree bend of the knee and the positioning of the lower leg on the padding surface. This allows a nonweightbearing of the foot or lower leg without the use of the arms.
Materials and Methods
The study was approved by the appropriate ethics committee, and all participants provided written consent to participate in the study. This clinical study was randomized with a crossover design. 19
Ten healthy participants were tested with 2 different aids, the HFSO iWALK 2.0 orthosis (iWALKFree Inc, Long Beach, CA) and FAC (Ossenberg GmbH, Rheine, Germany). In addition, the order in which the 2 aids were used was randomized. The selection was based on the sex and age of the participants. Among the 10 participants recruited were 5 women and 5 men with an average age of 36.7 ± 14.4 years and a body mass index (BMI) of 23.3 ± 1.9. After randomization, the orthosis was adapted to the individual participant according to the manufacturer’s instructions, and the participants were instructed on its use. After a 5-minute training period, the functional trial series was started.
The following 5 tests were performed: climbing stairs (CS), an L-shaped indoor course (IC), an outdoor course (OC), a 10-m walk test (10MWT), and a 6-minute walk test (6MWT).3,6 During the climbing test, participants ascended and descended 6 steps measuring 30 cm in depth, 17 cm in height, and 120 cm in width. The L-shaped IC had a length of 4 m and, after the left turn, a section spanning 2 m in length (Figure 3). The course consisted of structural floor panels (Terrasensa BASIS trade company, Kassel, Germany) with 50 × 50-cm dimensions. Several bulges and depressions created an uneven surface at different heights. The OC was equipped with various floor coverings. The course was 46 m long, with two 17-m-long and two 6-m-long sections, each laid out in a rectangular shape. The pavements included 10 types of pavers, including 3 different coarse cobblestones and various concrete, brick, and clinker pavers. In addition, the course had a 3-step staircase and a downward-sloping ramp with a 10-degree incline. The challenge of this OC was to adjust to different ground conditions permanently. Therefore, the course was modeled based on movement in an urban environment (Figure 4). Although the required time was measured for the CS, IC, OC, and 10MWT, the distance traveled was documented for the 6MWT. In addition, tripping events were counted while performing the IC, OC, and 6MWT. A tripping event was defined as a clearly visible interruption in the gait process for more than 1 second.
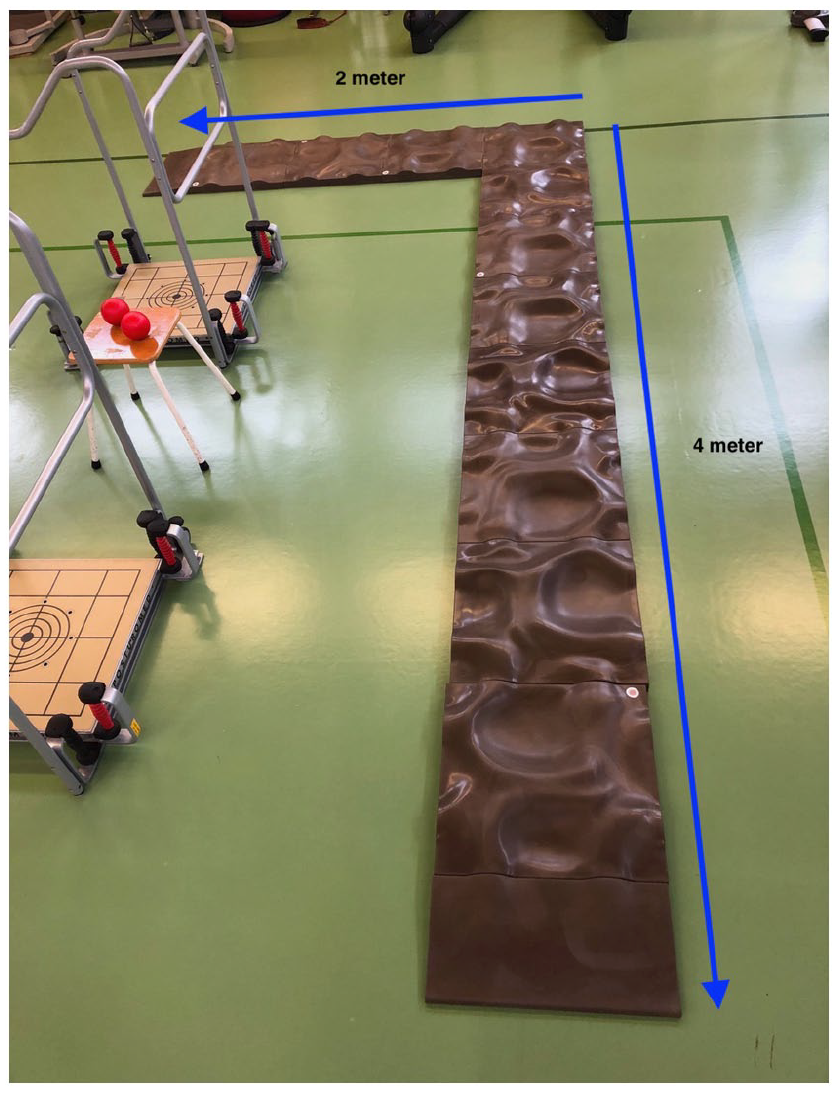
Indoor parkour setup with an L-shape design and the structural floor panels (Terrasensa BASIS trade company, Kassel, Germany).

The outdoor parkour used in this study with its obstacle elements such as a 3-step staircase or 10 degrees ramp.
Throughout the study, participants were required to take a break after each test for at least 5 minutes or until they no longer felt fatigued. A break of 30 minutes was taken after the first trial series and before testing with the second device.
Spiroergometric measurements were performed on another day to ensure sufficient rest and consisted of a 2-step treadmill test (Saturn 300/100 treadmill [h/p/cosmos; Sports & Medical Inc, Nußdorf, Germany]). It started with a resting interval to measure basal heart rate and oxygen consumption without physical exertion of the participant. The test was started at a speed of 1.5 km/h for 3 minutes with the first of the 2 aids. The same order was followed that was randomly assigned to the participant on participation. After 3 minutes, the speed was increased to 2 km/h. After 6 minutes, the test ended. A pause of at least 10 minutes was taken until the basal heart rate and oxygen consumption were achieved. The study participant then completed the same test procedure using the second aid. Heart rate was measured in beats per minute (bpm) and oxygen consumption in milliliters per minute per kilogram. After completing the tests, a questionnaire was answered regarding the items comfort, safety, pain, and recommendation on a visual analog scale (VAS, from 0 to 10 cm), whereby a longer distance represented a higher value, see supplemental material. For example, 10 cm means the highest imaginable pain or comfort and 0 cm absolutely no recommendation or safety feeling.
Statistical Analysis
The data were analyzed using the statistics program IBM SPSS Software (version 26, IBM, Armonk, NY). First, the D’Agostino-Pearson test was used to determine whether the data had a normal distribution. If a normal distribution was evident, a paired t test was used to compare utilities in the total cohort. When no normal distribution was present, the Wilcoxon test was used. A P value <.05 was determined to be statistically significant. The number of participants (n = 10) recruited for the present study resulted from a case number in planning for a paired mean comparison with an effect size of 1, a significance level of 5%, and a test strength of 80%.
Results
The time required to climb the stairs using the HFSO was significantly (P < .03) higher than that using the FAC (29.3 ± 7.8 seconds and 26.1 ± 6.5 seconds, respectively). The average time for completing the IC was 33.2 ± 9.8 seconds for the HFSO and 18.0 ± 6.5 seconds (P < .001) for the FAC. For the OC, the time required for completion using the HFSO (74.9 ± 27.4 seconds) was higher than that using the FAC (60.6 ± 21.8 seconds) (P = .06). Regarding the 10MWT, an average of 11.8 ± 4.1 seconds and 10.8 ± 4.7 seconds (P = .258) were recorded using the HFSO and FAC, respectively. The average distance covered in the 6MWT was 299.8 ± 81.2 m using the HFSO and 249.4 ± 68.7 m using the FAC (P = .102). Functional results are summarized in Table 1.
Overview of the Functional Tests.

Abbreviations: 6MWT, 6-minute walk test; 10MWT, 10-meter walk test; CS, climbing stairs; FAC, forearm crutch; HFSO, hands-free single crutch; IC, indoor course; OC, outdoor course.
Statistically significant differences.
Regarding tripping events, we found no significant differences between the 2 aids. However, on the IC with an uneven surface, the use of the FAC showed fewer tripping events, whereas on longer courses, such as the OC or 6MWT, the HFSO showed fewer tripping events (Table 2). For the subjective evaluation, ratings for the items comfort and recommendation were significantly higher for the HFSO, whereas the item pain was rated significantly lower. Both aids were rated equally for safety (Table 3).
Table Showing the Tripping Events in the Functional Tests IC, OC, and 6MWT.

Abbreviations: 6MWT, 6-minute walk test; FAC, forearm crutch; HFSO, hands-free single crutch; IC, indoor course; OC, outdoor course.
Subjective Outcomes Measured Using a Visual Analog Scale (VAS) Regarding Comfort, Safety, Pain, and Recommendation for Both Walking Aids.

Abbreviations: FAC, forearm crutch; HFSO, hands-free single crutch.
Statistically significant differences.
Spiroergometric testing revealed that the heart rate on the treadmill at a speed of 1.5 km/h was 131.1 ± 25.5 bpm using the HFSO and 148.1 ± 21.7 bpm using the FAC (P < .01). At a speed of 2 km/h, the average heart rate was 131.0 ± 24.4 bpm while using the HFSO and 161.8 ± 19.8 bpm while using the FAC (P < .001) (Table 3). Oxygen consumption measured during the treadmill ergometric test at a speed of 1.5 km/h averaged 15.4 ± 1.8 mL/min/kg using the HFSO and 18.3 ± 2.3 mL/min/kg using the FAC (P < .001) for the whole cohort. At a speed of 2 km/h, the average oxygen consumption was 16 ± 2.5 mL/min using the HFSO and 21.9 ± 2.4 mL/min/kg using the FAC (P < .001) (Table 4).
Overview of the Spiroergometric Results.

Abbreviations: FAC, forearm crutch; HFSO, hands-free single crutch.
Statistically significant differences.
Discussion
Our study showed that both aids had comparable results in the functional tests, whereby a trend could be detected that patients were faster while using the FAC at short distances. The HFSO could better facilitate covering longer distances in the 6MWT. Regarding safety, no falls were reported, and tripping events were equally distributed. In addition, spiroergometrics showed that energy consumption was lower when using the HFSO than when using the FAC.
Although the 6MWT showed no significant difference (P = .102), the distances covered were greater when using the HFSO than when using the FAC. In contrast, the difference in the results of 10MWT was smaller between the use of 2 aids, and shorter times were achieved using the FAC. Therefore, it can be assumed that the FAC is beneficial for a short period. However, as soon as this aid is used for a more extended period, the physical strain on the user increases significantly, leading to physical exhaustion and an increased tendency to trip.
However, a significant result was obtained when the IC was performed. On average, the time taken by the study participants to complete the course was shorter when using FAC than when using the HFSO. This result seems plausible because of the nature of the IC. The curved surface of the structural floor panels required special balance skills and coordination from the study participants. Because of the triple support when using FAC, the participants were provided sufficient stability. 2 Thus, completing the IC at a higher speed was possible. In contrast, when using the HFSO, the participants could hardly contact the ground because of the disproportion between the size of the foot of the orthosis and the curvature of the structural floor plates. This led to greater instability and gait insecurity in the study participants, which presumably manifested as slower locomotion.
When climbing the stairs, the study participants needed significantly more time, on average, using the HFSO than using the FAC. One explanation may be that, especially in tall participants, the foot of the lower leg, which was in the shell of the HFSO, was laid on the stair treads while descending the stairs. This made climbing stairs more difficult and resulted in slower locomotion when using the HFSO. This was the case for 2 participants.
Regarding the OC, no significant differences were found between the 2 groups. However, there was a tendency toward a higher time requirement when using the HFSO. This result can be explained by the fact that a greater distance can be covered in a shorter time when using the FAC with the help of the “swing-through gait.”9,20 By putting on both forearm crutches simultaneously and “swinging through” the affected leg, a greater distance is covered with one step than with a normal gait. In contrast, both lower extremities were involved in locomotion using the HFSO.3,20,23 Therefore, each step must be performed sequentially. In addition, when using the HFSO, contact with the ground occurred only via the test person’s healthy foot and the orthosis’s foot. On the other hand, when using the FAC, triple support is possible because of the 2 supports and the healthy foot. This offers the user more stability, especially when handling an uneven OC, and leads to a greater sense of security, consequently enabling faster locomotion. In addition, when assessing the time required to complete the OC, it must be considered that the use of HFSO requires greater physical balance from the participant. O’Sullivan described the difficulty of coordinating locomotion using an assistive device based on the movement of the contralateral lower extremity. 14 In contrast, it should be noted that fewer tripping incidents occurred overall with the HFSO when completing the OC.
A significant difference was found in the heart rate between the use of the 2 aids. It is possible that this significant difference can be explained by the activation of different muscles while using the 2 aids. Although the HFSO only requires the lower extremities for locomotion, the FAC places a double load on the upper and lower extremities.2,11,18 In particular, the muscles of the arms are heavily stressed by the FAC. 25 Increased muscle work results in increased energy consumption and heart rate. 25 In addition, locomotion using the FAC is not modeled on the physiological gait pattern, which leads to overall ineffectiveness and an increase in heart rate. 21 The HFSO allows weight relief through a 2-point alternating gait pattern. 12 This pattern allows for an energy-efficient reciprocal gait pattern in which both lower extremities participate in force generation and forward movement.8,12 In addition, the HFSO provides proprioception with full weightbearing owing to the wide support of the lower leg on the orthosis, thus providing improved feedback for gait stability. 15
A better sense of balance is required with an HFSO than with an FAC, as the participant must coordinate the contralateral lower extremity. 14 Therefore, despite the increased speed, the heart rate of the participants using the HFSO remained approximately the same at 131.1 ± 25.5 bpm at 1.5 km/h vs 131.0 ± 24.4 bpm at 2 km/h. In contrast, when the FACs were used, heart rate increased sharply from 148.1 ± 21.7 bpm to 1.5 km/h vs 161.8 ± 19.8 bpm at 2 km/h. A similar conclusion was reached by Waters et al, 24 who examined energy expenditure during 3-point walking using FAC. Waters’ study found that after 10 minutes of locomotion with crutches, the peak values for upper extremity endurance training were approached. Based on this, Waters et al concluded that rehabilitation using crutches presents a physically demanding challenge for the upper extremities. Nagpurkar and Troeller, 13 who compared the energy expenditure among normal walking, using crutches, and walking using an HFSO concluded that an HFSO was more efficient.
A preference was given to the HFSO in terms of comfort. Both HFSO and FAC appear to offer comparable safety. Pain perception was rated by the participants in the overall collective with an average of 1.4 points for the HFSO vs 3.6 points for the FAC. To explain this significant difference in the participants’ perception of pain, the design of the 2 aids and their respective forms of relief should be considered. With the HFSO, the lower leg of the affected extremity is placed on the shell, and the upper extremities are entirely free and unloaded; with the FAC, the hands serve as the only contact surface to the aid. Accordingly, when walking using the FAC, a high proportion of body weight rests on the upper extremities, especially the hands and forearms. This small contact surface must withstand a relatively high weight, which can lead to hand pain. While using HFSO, weights are placed on both the affected lower leg and the healthy lower leg to distribute the body weight evenly over both legs. On the one hand, this leads to more physiological weightbearing and, on the other hand, less pain in the stressed extremity. The significant results confirmed the secondary hypothesis regarding the category pain. All the test participants provided a higher recommendation toward HFSO. Because of the results in the categories comfort and pain, which were also significant and positive for the HFSO, this result seems plausible. This finding correlates with the results of a study conducted by Dalton et al. 4 They compared axillary supports commonly used in the Americas with hands-free orthoses in terms of patient preference, comfort, function, and safety.
On the other hand, general differences between FAC and HFSO should be mentioned. Although with FAC, a deliberate partial weightbearing in the affected extremity would be possible, such as allowing a slow weightbearing build-up, with HFSO only, nonweightbearing is possible. It also takes longer to apply the HFSO than to use the FAC adequately. Moreover, the cost should be considered. Unless the HFSO is covered by insurance, the cost of an HFSO is, on average, approximately 6-7 times higher than that of a pair of FACs.
The present study has some limitations. First, because of its pilot nature, only 10 participants were included. Although significant results could be achieved with a limited number of participants, this pilot study primarily served to identify initial trends regarding the suitability of HFSO compared to FAC in everyday clinical use. In addition, only participants with a BMI less than 35 were recruited. The average BMI of the participants was 23, corresponding to an adult’s normal weight. Consequently, the study results are based on a small sample of healthy and normal-weight individuals and cannot be generalized to debilitated or overweight individuals. Finally, all participants used the 2 aids, the HFSO and FAC, for the first time in the study and were only allowed a familiarization period of 5 minutes each. They were thus unpracticed, and even during the test, it was impossible to achieve sufficient habituation to the 2 aids, which would have occurred with their daily use. In addition, it also remains an open question whether the rest periods between the aid changes were sufficient. However, the crossover design should address a bias by the trial order.
Conclusion
The results of this study indicate that the HFSO is similar to FAC in achieving nonweightbearing of one lower extremity ambulation in healthy volunteers performing various ambulation tasks. Some disadvantages to the orthosis included higher cost and worse performance for short distances on uneven surfaces. There were some advantages to orthosis, specifically for longer distances on even surfaces. This would allow patients to use assistive devices as needed and achieve the highest degree of mobility. A follow-up study with a larger inclusion of patients who had undergone foot or ankle surgery should be conducted to corroborate the findings of this pilot study.
Footnotes
Supplemental Material
Ethical Approval
The study was approved by the Hannover Medical School ethics committee (No. 7801_BO_S_2018). All participants provided written consent to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.