
Abstract
Background:
This study compared the outcome of the L-shaped (L-AD) advancement of the periosteal and capsular complexes with or without augmentation using a free graft of the lower extensor retinaculum (AUG) in patients with chronic lateral ankle instability.
Methods:
A matched pair analysis was performed of retrospectively collected medical records of patients undergoing lateral ankle ligament repair who had completed at least 2 years of follow-up. Patients who underwent L-AD with AUG and patients undergoing L-AD alone were matched for age, sex, stress radiography findings, and body mass index. Patients with general joint laxity, osteoarthritic changes in the ankle, and subtalar symptoms and who underwent simultaneous surgical treatment for conditions other than that for lateral ankle ligament were excluded. A total of 46 patients were included in the study (23 patients in each group). Clinical outcome scores and postoperative mechanical instability were compared.
Results:
The median American Orthopaedic Foot & Ankle Society (AOFAS) score improved significantly (P < .001) from 72 to 97 in the L-AD alone group and from 77 to 100 in the L-AD with AUG group. The mean (±SD) talar tilt angles improved significantly from 11.1 to 4.7 degrees postoperatively (P < .001) in the L-AD alone group vs 9.7 to 5.2 degrees (P < .001) in the L-AD with AUG group. The mean anterior drawer distances were improved significantly postoperatively from 6.4 to 4.7 mm (P < .001) in the L-AD alone group, and from 6.5 to 4.5 mm (P < .001) in the L-AD with AUG group.
Conclusion:
The L-AD technique significantly improved AOFAS scores and mechanical instability of ankles with chronic lateral instability with a very low complication rate. Additional augmentation using a free graft showed no advantages in the ankle with a talar tilt of <20 degrees.
Level of Evidence:
Level III, retrospective case-control series.
Introduction
Until the late 1900s, tenodesis was a widely used treatment for chronic lateral ankle instability, but most procedures were invasive because they sacrificed one of the peroneal tendons.6,11,12,39 The nonanatomical route of classical tenodesis interferes with the physiological motion of the ankle and hindfoot. 18 The simple anatomical repair reported by Broström is less invasive and has fewer complications than tenodesis and does not interfere with the physiological motion of the ankle and hindfoot.4,5,20 The procedure has become the gold standard surgical treatment for chronic lateral ankle instability. 5
However, instability may recur depending on the remnant quality.27,45 When the ligament has lost tension but still has a residual ligament component (remnant), symptoms improve with suturing, and ligament tension is restored. The Broström-Gould technique is a modification of the Broström procedure for cases with poor-quality residual ligaments.16,17,26 This modification compensates for the weakness of the original Broström method, although the technique of pulling and suturing the extensor retinaculum to the fibula is not an anatomical repair.
Anatomic reconstruction with a tendon graft is a treatment choice when both the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) components are severely damaged or lost. 15 Using allogeneic tendons, there is no need to harvest the tendon from a site other than the ankle joint, and there are no donor site issues. Unfortunately, in countries such as Japan, where health insurance does not cover the use of allogeneic tendons, autologous tendon harvesting from the knee area is essential to obtain a voluminous tendon.15,34 Under such conditions, it is desirable to use the residual ligament as much as possible and complete an anatomic augmentation with local materials.
We developed a modified Broström procedure in which the ATFL is advanced as a single sheet in conjunction with the fibula periosteum and articular capsule to avoid additional damage to the residual ligamentous substance during surgical deployment. 38 This technique also allows for additional reinforcement with a free graft of the inferior extensor retinaculum.
Here, we report the results following these procedures and compare the outcomes of advancement alone vs advancement with augmentation by a free graft of the inferior extensor retinaculum (AUG). Comparisons were made by matching the patient’s baseline conditions and preoperative instability. We hypothesized that advanced surgery with augmentation would yield better outcomes than advanced surgery alone.
Materials and Methods
Patients
This study was approved by the Institutional Review Board. Informed consent was obtained from all patients.
The medical records of 191 patients who underwent operative treatment for chronic lateral ankle instability between 2000 and 2019 were reviewed. The operations were performed at Imperial Gift Saiseikai Nara Hospital in the first decade and at Nara Prefecture General Medical Center in the second decade by the same 2 orthopaedic surgeons (K.S. and S.I.) specializing in foot and ankle. All patients complained of pain and/or recurrent ankle instability despite conservative treatment consisting of an orthosis, strengthening of the peroneal muscles, and occasional treatment with nonsteroidal anti-inflammatory drugs for at least 3 months. Apprehension by the manual anterior drawer test or mechanical instability detected on stress radiography was essential for the diagnosis of chronic lateral ankle instability.
Ligament repair was performed with an L-shaped flap of the periosteal and capsular complexes (L-AD) with or without AUG in 155 ankles (148 patients) with repairable remnants. Twenty ankles (19 patients) that were treated with reconstructive surgery using auto-tendon grafts because of poor or empty remnants and 15 ankles (15 patients) that were treated with arthroscopic repair for isolated ATFL injuries were excluded. The other exclusion criteria were as follows: age <13 years or >65 years; presence of general joint laxity; incomplete records; follow-up period of <2 years; concomitant Takakura and Tanaka stage II to IV osteoarthrosis; or other previously treated foot and ankle diseases, such as anterior impingement syndrome, osteochondroma, osteochondral lesion, and arthroscopically treated os subtibiale (Figure 1).

Inclusion flowchart.
Twenty-three patients who underwent L-AD with AUG were matched by age, sex, body mass index, and preoperative mechanical instability in a 1:1 ratio with patients who underwent L-AD alone. Baseline demographic data and preoperative mechanical instability of the ankle did not differ significantly between the groups. Of the 46 patients who were active in sports, 12 were elite athletes, 13 were nonelite competitive athletes, and 5 were recreational athletes. There was no significant difference in the distribution of patient activity levels between the 2 groups (Table 1).
Basic Demographic Data and Preoperative Mechanical Instability of the Patients.

Mann-Whitney U test.
Fisher exact test.
Student t test.
Operative Technique
Arthroscopy
Operations in the early case were performed under spinal anesthesia at the Imperial Gift Saiseikai Nara Hospital and under general anesthesia at the Nara Prefecture General Medical Center. The patients were placed on the operation table in a semilateral decubitus position with the affected ankle facing upward (Figure 2). An arthroscopic examination was performed using an irrigation pump. A 2.7-mm, 30-degree oblique scope was introduced into the joint from the medial portal and a probe or a shaving instrument from the lateral portal. The scarred or inflamed synovium was removed.
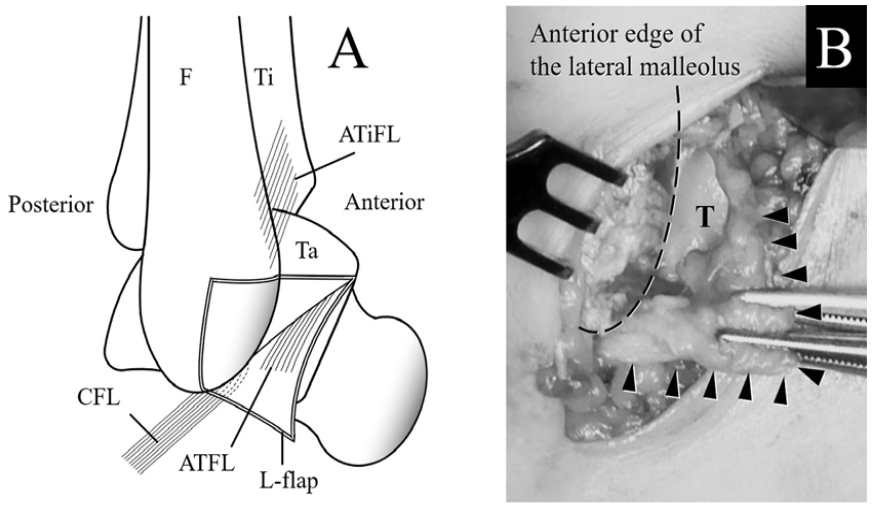
(A) Turning the L-shaped flap of periosteum and joint capsule including the ATFL enables surgeons to confirm the ligament condition. (B) L-shaped flap of periosteum and joint capsule including the ATFL are visualized. ATFL, anterior talofibular ligament; ATiFL, anterior tibiofibular ligament; CFL, calcaneofibular ligament; F, fibula; T, talus; Ta, talus; Ti, tibia.
Advancement of the ligament(s)
After arthroscopic examination, repair of the lateral ligament(s) was performed with the hip slightly flexed and internally rotated, and the knee flexed at 30 to 45 degrees, using a tourniquet with a pressure of 280 mm Hg. A 4-cm-long skin incision from the upper end of the talar attachment of the ATFL to the fibula at the attachment of the CFL was used to explore the joint capsule and periosteum of the lateral malleolus. The periosteum of the lateral malleolus was peeled from the bone in an L-shaped flap, and the proximal border of the flap was extended to the joint capsule, straight and parallel to the upper edge of the ATFL. The longitudinal border of the flap was extended to the end of the fibula (Figure 2, A and B). The remnant volume of the ATFL was easily observed directly from the joint side by turning the flap. The os subfibulare was detached from the fibula with the flap if present (Figure 3A). The ossicle was carefully peeled off from the flap membrane (Figure 3B). The condition of the CFL was also confirmed by a small hook device, such as a tendon tucker.

(A) Os subfibulare is easily detached from the fibula with the flap. (B) It is then removed from the flap without deteriorating the continuity of the periosteum and the capsule.
The proximal end of the ligament(s) was then advanced and reattached to the fibula using suture anchors. Absorbable suture anchors (Panalok; Mitek, Norwood, MA) were used in the early series and soft suture anchors (JuggerKnot Soft Anchor-1.4; Zimmer Biomet, Warsaw, IN) were used in the later series. Two anchors were used to suture the ATFL when the CFL was intact, and a third anchor was used to advance the CFL (Figure 4). If there was no space in the distal fibula for the third anchor in the early series, the CFL was advanced using a pull-out suture. The periosteum of the flap was also advanced with 3-0 absorbable monofilament sutures (Figure 4B).

(A) Two anchors are used at the fibular attachment of the anterior talofibular ligament, and the third anchor is used at the fibular attachment of the calcaneofibular ligament. (B) The remnant(s) are advanced with the joint capsule.
Augmentation
A free graft (8 mm × 20 mm) was harvested from the lower extensor retinaculum (Figure 5) and used to reinforce the ATFL (Figure 6, A and B). The graft was placed medial to the flap and fixed with 2 anchors each to the fibula and talus along the flap (Figure 7). The 2 anchors inserted at the talar attachment were used to fix the distal ends of the graft (Figures 6 and 7).

Harvesting of graft from the inferior extensor retinaculum. 31 EDL, extensor digitorum longus tendons; IER, inferior extensor retinaculum.

(A) Augmentation of the anterior talofibular ligament with a free graft from the lower extensor retinaculum. (B) The 2 additional suture anchors are used to fix the distal end of the graft to the talus. EDL, extensor dogotorum longus tendons; IER, inferior extensor retinaculum.

Position of suture anchors and the inferior extensor retinaculum graft.
Postoperative course
A below-the-knee cast was applied for 3 weeks. Touchdown of the operated leg was allowed from the next day using crutches, and full weight-bearing was allowed 1 week after the operation. A semi-hard ankle brace was used 9 weeks after cast removal. Jogging was allowed 10 weeks postoperatively. Exercise of the toe was encouraged immediately after the operation. The patients were instructed on daily ROM exercise and peroneal muscle training, supervised by physiotherapists, once a week.
Clinical Evaluation
The patients were evaluated using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot rating scale, while the mechanical instability assessed in the talar tilt angle and anterior drawer distance were measured on stress radiographs using a Telos stress apparatus with a stress of 10 daN. 7 Postoperative complications were also recorded. Pre- and postoperative AOFAS scores and measured instabilities were compared between patients who underwent an L-shaped flap advancement of the periosteal and capsular complexes with augmentation and those who underwent L-shaped flap advancement alone.
Statistical Analysis
The statistical analysis was performed using EZR (version 1.61; Saitama Medical Center, Jichi Medical University, Saitama, Japan; based on R ver. 4.2.2). 19 Propensity score matching was performed with a caliper = 0.2. With a significance level of P = .05 and a power of 0.8, the study’s sample size was sufficient to trust the results of the comparisons of the instability measure and clinical score. Variance normality and equality were measured using the Shapiro-Wilk and F tests. AOFAS scores were evaluated using the Mann-Whitney U test or Wilcoxon signed-rank test. The talar tilt angle and anterior drawer were compared using the Student t test or Welch t test. The sex ratio, retention of os subfibulare, and proportion of advanced CFL cases were assessed using Fisher exact test. Patient activity levels were compared between the groups using the Mann-Whitney U test. Statistical significance was established at a threshold of P = .05.
Results
Advancement of the CFL was performed in 7 patients without augmentation and 11 with augmentation. The os subfibulare was removed in 11 patients without augmentation and 9 with augmentation. The results are summarized in Table 2. With the numbers available, the median AOFAS score, mean talar tilt angle, and anterior drawer distance improved significantly postoperatively in both groups. No significant intergroup differences in the postoperative AOFAS scores or mechanical instability were detected. A partial tear of the longus extensor digitorum tendon occurred in 1 patient during harvesting of a free graft from the lower extensor retinaculum, but no dysfunction remained. In the 46 cases included in our study, complications such as deltoid ligament injury or longitudinal rupture of the peroneal tendon were not observed. There were no cases of delayed healing, wound infection, superficial nerve disturbance, or suture anchor–induced osteolysis. None of the patients showed decreased activity levels after surgery, and all athletes returned to their preinjury activity levels.
Comparison of AOFAS Scale Scores and Mechanical Instabilities.

Abbreviation: AOFAS, The American Orthopaedic Foot & Ankle Society.
Mann-Whitney U test.
Difference between pre- and postoperative scores or measurements.
Student t test.
Welch t test.
Discussion
In our L-flap procedure, the ATFL was advanced as a single sheet with the complex of the articular capsule and periosteum of the fibula. By avoiding a capsulotomy at the torn site of the ligament and isolation of the capsular ligament from the capsule, it is possible to restore the tension of the joint capsule and the residual ligament without causing additional damage. The CFL condition was easily confirmed during the L-flap procedure, and advancement of the CFL was performed in 18 of the 46 patients without extension of the skin incision. The os subfibulare was present in 20 of the 46 patients and was removed with no additional damage to the ligament or capsule surrounding the ossicle.
In the early cases of our series, additional augmentations were routinely performed using AUG, except in those who underwent simultaneous surgical treatment for other foot or ankle disorders. When the outcomes of patients who underwent L-AD alone were good, L-AD alone was performed in the subsequent series, except in ankles with significant mechanical instability that required tendon grafting.
This comparative study showed no advantage of augmentation by L-ADs, whereas L-ADs with or without AUG significantly improved the clinical scores and mechanical instability of ankles with chronic lateral instability, with a very low rate of complications. No difference was observed either because the L-flap advancement was effective without reinforcement or because reinforcement with the extensor reticulum did not increase the strength of the ligament. Because there were no cases of recurrent instability in the L-flap advancement alone group, it can be interpreted that L-flap advancement does not require augmentation. This study used propensity score matching and excluded ankles that showed a talar tilt angle of ≥20 degrees. Thus, it could not be determined whether additional AUG had an advantage over L-AD alone for ankles with significant instability. The value of L-flap advancement in comparison to the Broström or Gould variants was also unclear in this study.
Because of the different periods in which the operations were performed, the mean follow-up duration was longer in patients who underwent L-AD with AUG than in those who underwent L-AD alone. The quality of the extensor retinaculum used for augmentation varied and may have affected the effectiveness of the augmentation. This difference may have affected the evaluation of the study outcomes, although the follow-up intervals for each group were sufficient.
Arthroscopic repair or reconstruction of the lateral ligament(s) of the ankle has developed rapidly and has become increasingly popular.14,43 To date, arthroscopic repair or augmentation has focused on the ATFL1,2,9,10,21 -23,25,29,40; however, few reports have described arthroscopic repair of the CFL 42 because of its anatomical characteristics outside the capsule. Favorable results of arthroscopic repair have been reported in patients with a remnant isolated ATF injury.25,28,41 Unlike the ATFL, the CFL is an extracapsular ligament that is difficult to completely repair arthroscopically.27,45 The combined injury of ATFL and CFL produces more severe damage than a single injury, 27 and an additional arthroscopic augmentation did not improve the outcome. 45 Because of the difficulty in arthroscopic repair of the CFL, many surgeons who attempt complete arthroscopic surgery alone are likely to perform reconstruction using a tendon graft for all ankles, except in cases of isolated ATFL injury. In our opinion, this may be overtreatment for combined injuries of the ATFL and CFL with remnants. Reconstruction with tendon grafts should be limited to ankles in which the remnants of the ATFL and CFL are lacking or are of significantly poor quality, and ankles with repairable ligaments should be repaired with or without local tissue augmentation.
Augmentation of the ATFL through the periosteal flap of the fibula was first described in the 1980s by Reichelt and Weyrauch, 30 whereas CFL was reported by Glas et al. 13 Sjølin et al 33 reported favorable short-term results of these augmentation methods, although they required an 8-cm-long skin incision. Good short-term results of augmentation using an artificial ligament were recently reported. The artificial ligament may support good ligament healing, but its long-term efficacy is unknown.8,24
The lateral ligaments of the ankle include the ATFL, CFL, and posterior talofibular ligament. There are many variations of their involvement in combination injuries, the remnant quality, and the presence of the os subfibulare.3,32,36,37 The arthroscopic technique is minimally invasive and has allowed a breakthrough in the treatment of chronic lateral instability of the ankle, although in its current form, it may not be applicable to different ligament conditions.43,44 The Broström procedure and the modified Broström-Gould technique have been considered the gold standard; however, to date, consensus is lacking on a decision-making paradigm for determining the appropriate treatment for chronic lateral ankle instability, which has many variations. 35
The L-flap advancement method enables surgeons to restore the tension of the joint capsule and residual ligament and remove the os subfibulare without damaging the parenchyma by advancing the flap. The procedure requires a 4-cm skin incision and is applicable to various ligament conditions, except in ankles where the remnants of the ligaments are severely damaged or lost. In the current study, patients with a talar tilt angle of less than 20 degrees were selected for both comparison groups during the matching process; thus, the results may not be applicable to patients with talar tilt angles of greater than 20 degrees.
The significance of the study results is limited by the fact that a randomized comparison was not performed; a matched pair analysis was performed. Additionally, each group had fewer than 30 cases. Another study limitation is that the results should be cautiously interpreted because mechanical instability as measured on stress radiographs does not necessarily accurately indicate the severity of ligamentous injuries. Although the minimum follow-up period was 2 years, it varied widely between cases. Moreover, there may have been effects that were not clinically assessed during the follow-up period.
Conclusion
The L-AD technique significantly improved the clinical scores and mechanical instability of ankles with chronic lateral instability with a very low complication rate. Additional augmentation using a free graft showed no advantages in the ankle with a talar tilt of less than 20 degrees.
Footnotes
Author Note
This study was performed at the Nara Prefecture General Medical Center and the Imperial Gift Saiseikai Nara Hospital
Ethical Approval
This study was performed in accordance with the ethical standard in the 1964 Declaration of Helsinki. Details that might disclose the identity of the subjects under study have been omitted. This study was approved by the institutional review board (IRB ID: 368).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.