
Abstract
Background:
Treatment with ultrasonography (US)- and color Doppler (CD)-guided mini surgery for insertional Achilles tendinopathy has shown good clinical results in a sports medicine setting. The aim in this study was to introduce this new methodology at a county hospital and study the clinical results on a traditional orthopaedic population.
Methods:
Twenty-six consecutive patients (12 men, mean age 61 years; 14 women, mean age 56 years) with a long duration (>12 months) of pain symptoms from insertional Achilles tendinopathy (a combination of bursae, bone, and tendon pathology) were included. US- and CD-guided surgical removal of bursae, bone, and tendon pathology, performed with local anaesthesia, was used. After surgery, there was immediate weightbearing loading without immobilization, followed by a structured rehabilitation protocol for 12 weeks. The VISA-A and SEFAS scores plus a questionnaire evaluating satisfaction with treatment and activity level was used for evaluation.
Results:
At the 1-year follow-up, there were 3 dropouts. Twenty-one patients were satisfied. Their VISA-A score had increased significantly from 26 to 81 (P < .001), and the SEFAS score from 17 to 38 (P < .001). Two patients were not satisfied. There were 3 complications, 2 superficial skin infections, and 1 wound rupture.
Conclusion:
For patients with chronic painful insertional Achilles tendinopathy, the US- and CD-guided surgical treatment method followed by immediate weightbearing loading showed a high satisfaction rate and improved functional scores at the 1-year follow-up in a majority of the patients. There are advantages using this method compared to other more tendon invasive surgical methods in use for this condition.
Level of Evidence:
Level IV, case series.
Introduction
Chronic pain in the Achilles insertion affects athletes and nonactive individuals10,15,20 and is considered difficult to treat.5,6,15,18,21 The condition is commonly called insertional Achilles tendinopathy and includes pathology in bursa, tendon, and bone tissue (Haglund deformity, intratendinous bone spurs, and prominences).3,8,19 The typical clinical finding is tenderness in a prominent tendon insertion. The diagnosis has previously mainly been based on clinical examination radiography and magnetic resonance imaging, but ultrasonographic (US) examination has been shown to be the best for examination of tendons and tendon insertions. 13
In a recent study on patients having a combination of pathology in the subcutaneous and retrocalcaneal bursa, the distal Achilles tendon, and a prominent upper calcaneus (Haglund deformity), immunohistochemically examined tissue samples from these tissues showed rich innervation patterns, especially in the subcutaneous bursae. 3 Recently, the plantaris tendon also has been shown to be involved in insertional Achilles tendinopathy.2,11,17
When conservative treatments6,7,9 fail, surgical treatment is indicated. Several different surgical treatment methods have been described, such as artroscopic removal of the retrocalcaneal bursa and resection of the upper calcaneus.14,22 More invasive methods include Achilles tendon detachment procedures, like the Nunley operation, where detachment is followed by removal of interfering bone prominences and intratendinous bone spurs and calcifications, and then reattachment of the Achilles tendon.5,12,16 Another method is the Keck and Kelly procedure, using an osteotomy in the calcaneus to offload the posterior part of the heel. 4 Most methods require a relatively long postoperative rehabilitation, including periods with immobilization, sometimes wearing a booth for 6-8 weeks. There is only 1 study using US- and Doppler-guided surgery, and that method allows for a realtively quick rehabilitation with immediate weightbearing loading and no immobilization. 1
The aim with this 1-year prospective study was to introduce the US- and CD-guided surgical treatment method and to study the results on a traditional orthopaedic population suffering from chronic painful insertional Achilles tendinopathy.
Material and Methods
Patients
Twenty-six consecutive patients (12 men, mean age 61 years; 14 women, mean age 56 years) with a long duration (>12 months) of insertional Achilles tendon pain were included in the study. All patients were Swedish, from the most southern part of the country, with a history of insertional pain during Achilles tendon loading and a tender swelling sensitive to compression from the shoe at the back of the heel. The activity levels ranged from walking (n = 11), recreational activities involved in jogging and running (n = 8), padel tennis (n = 3), football (n = 1), tennis (n = 1), golf (n = 1), and biking (n = 1). They were generally healthy, but 6 patients suffered from hypertension, 1 had asthma, 1 was HIV positive, and 1 had mild rheumatoid arthritis. For treatment, all patients had tried a period of rest and loading regimens including eccentric training, 7 and 3 patients had had local cortisone injections.
Inclusion criteria: More than 12 months’ duration of disabling pain in the Achilles insertion not responding to rest and physiotherapy including an eccentric loading regimen.
Exclusion criteria: Systemic chronic inflammatory conditions affecting the ankle joint-foot and previous fractures affecting the ankle joint and calcaneus.
Clinical Examination and US Plus Color Doppler examination
Clinical examination, US, and color Doppler (CD) examination and the surgical procedure was performed by the same clinicians at the local county hospital. At clinical examination, all patients had a tender thickening at the back of the heel, a widened distal Achilles, and suspected filling in the region for the retrocalcaneal bursa. Many patients also had a tender bony prominence in the insertion, or local tenderness in the region for the plantaris tendon on the medial side of the insertion.
High-resolution grayscale US and CD examination (SECMA) with a linear multi-frequency (8-13 MHz) probe, was used to verify the diagnosis showing pathology in the Achilles insertion (Figure 1).

Grayscale ultrasonographic pictures from a patient suffering from chronic painful insertional Achilles tendinopathy. (A) Grayscale ultrasonographic picture showing enlarged retrocalcaneal bursa (orange arrow), thickened tendinopathic distal Achilles tendon (marked with yellow line), and Haglund-like deformity of the upper calcaneus (green arrow). (B) Grayscale ultrasonographic picture showing enlarged and thickened subcutaneous bursa with high blood flow (asterisc) in bursa walls (white line). (C) Grayscale ultrasonographic picture showing intratendinous bone spur (white arrow) in the Achilles insertion.
Immediately preoperatively, we again used US and CD examination to verify the pathology in the insertion. The following was identified: an enlarged subcutaneous bursa (n = 26) and retrocalcaneal bursa (n = 20) with high blood flow inside the bursa walls, a thickened distal Achilles tendon with structural tendon changes (n = 26) located ventral and central in the tendon with localized high blood flow inside and outside the ventral part of the tendon, bone spurs and/or bone prominences inside the distal tendon (n = 12), a prominent upper calcaneus (n = 20), and a thickened plantaris tendon surrounded by high blood flow (n = 15).
Surgical Procedure
The operations were done in local anesthesia (5-10 mL of xylocaine 10 mg/mL with adrenaline 5 µg/mL) infiltrated subcutaneously, inside and around the superficial and retrocalcaneal bursae, toward the periosteum of the upper calcaneus, and on the ventral side of the distal Achilles tendon. After 10-15 minutes, the surgical procedure was started. Through a lateral or medial (depending on if the plantaris tendon was involved) longitudinal skin incision about 4-5 cm in length, the subcutaneous tissues were visualized. The first step was to locate the subcutaneous bursa, and first the posterior part of the bursa was carefully dissected from the skin, then the anterior part of the bursa was separated from the tendon. The whole bursa was removed (Figure 2). Next step was removal of the retrocalcaneal bursa. This bursa is located between the posterior smooth surface of the superior calcaneal tuberosity and the ventral side of the distal Achilles tendon. The bursa was visible by lifting the Achilles tendon posteriorly, and then the bursa was carefully dissected from the ventral side of the tendon and removed (Figure 3). Then the prominent upper calcaneus (Haglund-like deformity) was removed. This was done by using an osteotome (Figure 3C). By placing the index finger between the tendon and upper calcaneus and dorsiflexing the ankle joint, any remaining impingement was excluded. The next step was the scraping procedure, where the infiltrative fat tissue on the ventral side of the distal Achilles was carefully scraped away using a scalpel. Then, if there was suspected plantaris tendon involvement, via a medial incision the medial side of the insertion was inspected. If there was a thickened distal plantaris tendon, the distal 4-5 cm of the plantaris was carefully released and removed. Finally, bone spurs and intratendinous bone prominences were removed via a longitudinal tenotomy (Figure 4A). The prominent bone was carefully released from the tendon by sharp dissection with the scalpel, and if anchored to the underlying bone an osteotome was used to loosen and then extirpate the bony prominence (Figure 4B). The tenotomy was sutured side-to-side using 4/0 Vicryl sutures.

(A) Straight longitudinal incision on the lateral or medial side of the Achilles insertion. (B) The subcutaneous bursa is carefully released from the skin. (C) The subcutaneous bursa is carefully released from the tendon and removed.
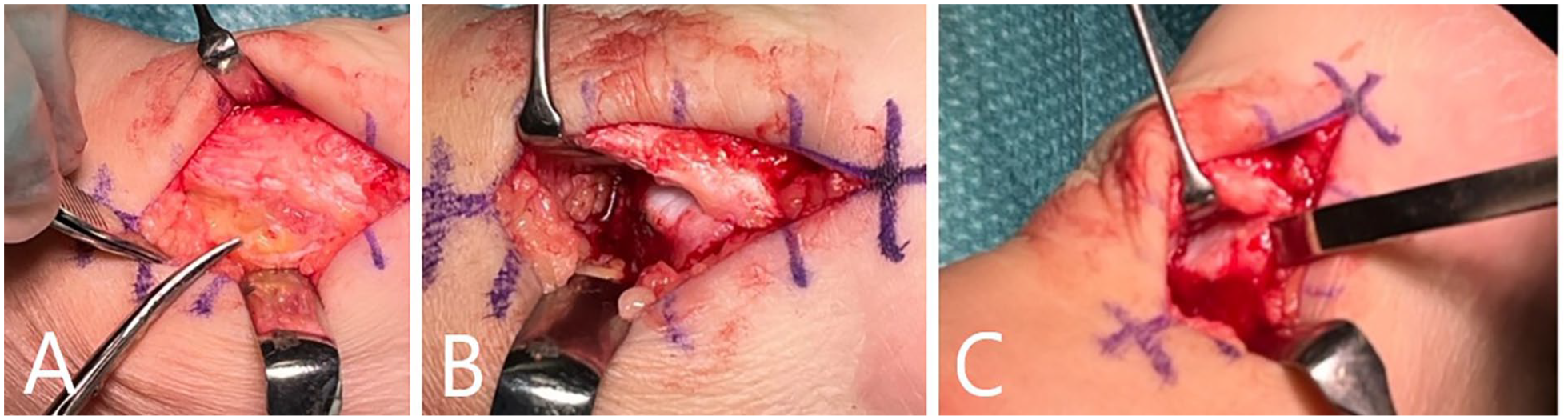
(A) The retrocalcaneal bursa is identified and removed. (B) The tendon is lifted, and the upper edge of the calcaneus is inspected to verify if there is impingement between the Achilles and the calcaneus. (C) The upper prominent edge of the calcaneus is removed to create space between the tendon and the calcaneus.
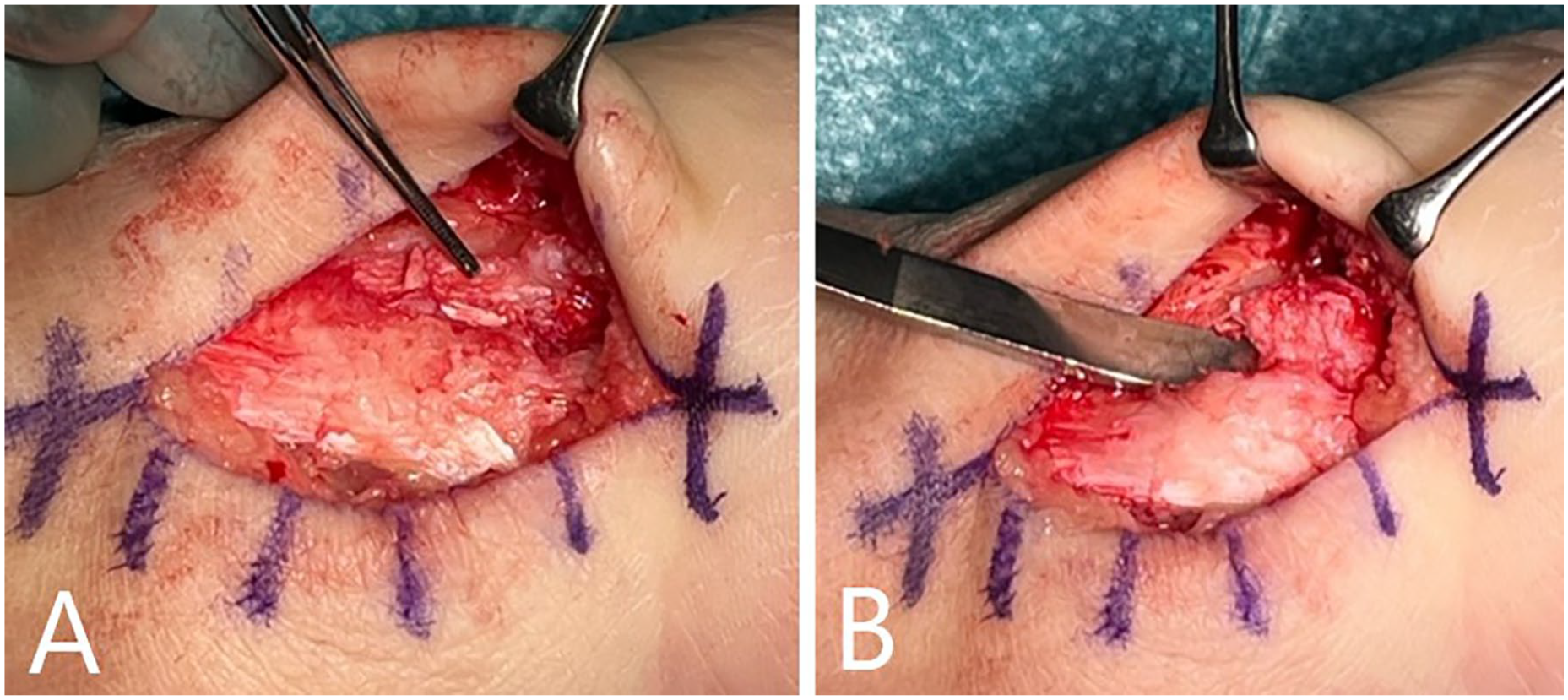
(A) Intratendinous bone prominences were removed via a minor longitudinal tenotomy. (B) Removal of intratendinous bone prominence.
Finally, cavities were flushed with 3-4 mL Marcain, and loose bone ossicles were removed. Careful hemostasis. The skin incision was sutured with nonresorbable sutures.
Postoperative rehabilitation
There was a structured rehabilitation protocol for 12 weeks.
1-6 weeks
A shoe with open heel was used to protect the sensitive skin at the back of the heel.
Weightbearing loading walking (half body weight) was allowed if there was intratendinous bone removal; others used full body weight loading. Gradually increased distances in slow speed was initiated. Light biking was advised.
Sutures were removed 3 weeks after operation.
Week 7-12
Patients were advised to adapt to use shoes with soft heel pad. Increased walking distances and speed were advised, along with gradually increased biking—including heavier intervals. Gradually increased strength training (heel raises and eccentrics) was started.
Week 13 onward
For sport actives, sport-specific exercises can be started, including light jogging (jog 50 m–walk 50 m, jog 100 m–walk 50 m, etc).
Evaluation
The evaluation was performed by an independent doctor who had had no previous contact with the patients and had not been involved in the operations or rehabilitation. All patients filled in a VISA-A and SEFAS score at baseline and 12 months after surgery and answered a questionnaire about satisfaction with the result of the operation (satisfied or not satisfied), activity level, occupation, smoking, and medication.
Statistical Analysis
Statistical analyses were done in the Statistical Package of Social Science (SPSS Inc, Chicago, IL). Paired Student t test was used to identify statistical differences in the VISA-A and SEFAS scores before and 1 year after surgery. A P value <.05 was considered significant.
Results
Twenty-three patients participated in the follow-up, and 21 patients were satisfied with the result of the operation. Their mean VISA-A increased significantly (P < .001) from 26 (range 4-64) before surgery to 81 (70-100) 1 year after surgery (Figure 5). Their mean SEFAS score increased significantly (P < .001) from 17 (range 5-29) before surgery to 38 (range 30-48) 1 year after surgery (Figure 6).

The VISA-A scores before and 1 year after surgery. There was a significant (P < .001) improvement after surgery.

The SEFAS scores before and 1 year after surgery. There was a significant (P < .001) improvement after surgery.
Two male patients were not satisfied, their VISA-A score had increased from 54 to 78 and 52 to 61, respectively, and their SEFAS score had increased from 23 to 29 and 27 to 30, respectively.
Dropout Analysis
Three patients (all women) did not participate in the 1-year follow-up. One patient was satisfied at the 3-month postoperative clinical control and did not want to be further followed up. One patient was not satisfied at the 3-month control and is going to undergo further surgical treatment. One patient did not want to participate in the follow-up because of private reasons.
Complications
Two patients had a verified superficial wound infection that was treated successfully with antibiotics. One patient had a minor wound rupture that healed successfully over time.
Discussion
This 1-year follow-up study on patients with chronic painful insertional Achilles tendinopathy, operated with ultrasonographic (US)- and Doppler (DP)-guided surgery in local anaesthesia, showed high satisfaction rate, and good functional results in a high proportion of the patients.
The patients included in this study represents the population seeking help for insertional Achilles pain at a local county hospital. It is clearly shown from the low preoperative VISA-A and SEFAS scores that the included patients had major pain and functional disabilities.
To try to minimize the risk for bias, an independent doctor, not involved in the inclusion, operations, or rehabilitation of the patients was responsible for the 1-year follow-up.
There were 3 dropouts at the 1-year follow-up. The results from the dropout analysis did not significantly change the main impression of the results.
It is well known that chronic painful insertional Achilles tendinopathy is difficult to treat, and a range of surgical methods have been presented for this condition. 21 There is no golden standard method, and the results after surgery are varying. At the county hospital where the current study was performed, the responsible foot and ankle surgeon was experienced in using the Nunley5,16 surgical procedure for many of his patients who suffered from chronic painful insertional Achilles tendinopathy.
The varying clinical results after surgical treatment in the Achilles insertion might be the lack of information about the innervation patterns in the different tissues involved in this condition. It was not until recently that the innervation patterns were clarified. In patients having pathology in the subcutaneous and retrocalcaneal bursa, distal Achilles tendon and upper calcaneus (Haglund-like deformity), immunohistochemical analyses showed that the most nerve-rich tissue was found in the subcutaneous bursa, followed by the retrocalcaneal bursa and distal Achilles. 3 These tissues could alone, or together, be responsible for the pain. Furthermore, the distal plantaris tendon,2,17 bone spurs, and loose bone fragments inside the distal tendon can be involved.
The US+CD-examination reliably verifies bursa, tendon, and bone pathology, 13 and the findings guide the surgical procedure. Thus, US examination replaces the use of radiographic and magnetic resonance imaging examination. The possibility to use dynamic examination makes it efficient to explore all tissues in the whole insertion and find the exact position of bone spurs and loose bone fragments. In addition, combining US with CD provides the unique ability to study blood flow in the Achilles tendon, which has been demonstrated to be helpful trying to find the nerves in Achilles tendinopathy. 13 However, operating an US probe is user dependent, and interpreting the images requires considerable experience, which could be a general limitation. In our study, the US and CD examinations were performed by experienced examiners.
In the current study, the findings at the preoperative US and CD examination guided the surgical procedure. An enlarged subcutaneous and retrocalcaneal bursa with high blood flow in the bursa walls was extirpated, a prominent upper calcaneus (Haglund-like deformity) was excised, the ventral side of a tendinopathic distal Achilles was scraped, bone spurs or intratendinous bone fragments were removed and the distal part of a tendinopathic plantaris tendon, was removed. For all patients in our study, the subcutaneous bursa was removed. In 20 of 26 patients, in addition, the retrocalcaneal bursa and upper calcaneus (Haglund-like deformity) were removed, together with a scraping procedure on the ventral side of the distal Achilles. In 12 patients, there was also removal of intratendinous bone spurs and bone fragments via a longitudinal tenotomi, and in 15 patients also removal of the distal part of the plantaris tendon.
Interestingly, to our knowledge, there is only 1 previous study on surgical treatment of patients with chronic painful insertional Achilles tendinopathy reporting specific importance of removing the richly innervated subcutaneous bursa. 1 Most other studies focus on removing the retrocalcaneal bursa and upper calcaneus. The background to pay specific interest to the subcutaneous bursa is that it has been shown that this bursa is richly innervated in patients suffering from chronic painful insertional Achilles tendinopathy. 3 A study using US- and CD-guided surgery showed good clinical results after removal of the subcutaneous and retrocalcaneal bursae and the upper calcaneus (Haglund-like deformity) and a scraping procedure on the ventral side of the distal Achilles. 1
The most commonly used surgical treatment method for chronic painful insertional Achilles tendinopathy at the hospital involved in the current study was the Nunley procedure. The preoperative evaluation by the responsible surgeon showed that in 10 of 26 patients included in the current study, he would have used the Nunley procedure for treatment. After using the US- and CD-guided surgical procedure instead, in 9 of these 10 patients, there was a good result of the operation. Comparing the Nunley procedure with the US- and CD-guided surgical procedure there appears to be several advantages using the US- and CD-guided procedure. US and CD guidance provides a reliable diagnosis, and the dynamic examination can properly locate all affected tissues. Preoperative US allows for proper positioning of skin incisions and tenotomi to minimize the tissue trauma. This mediates the possibility to avoid tendon detachment. The limited tissue trauma and lack of need for tendon detachment allows for a rehabilitation using immediate weightbearing loading and no immobilization. Furthermore, the operation is performed in local anaesthesia, and the risks for side effects using general or spinal anesthesia are avoided. The need for sick leave from work varies depending on the type of occupation, but not seldom is there no need for sick leave from work after that type of operation, compared to often a need for long sick leave periods after the Nunley procedure. Other methods in use for treatment of insertional Achilles tendinopathy are arthroscopic removal of the retrocalcaneal bursa and Haglund deformity, and the Keck and Kelly method using an osteotomy in the calcaneus. However, while using those methods, no treatment is done to the nerve-rich subcutaneous bursa and intratendinous bone formations.
A limitation of the current study is that it is a case series and not a randomized study comparing 2 methods. Therefore, the results in relation to the results from other studies cannot be compared but only be discussed. Another weakness of the current study is that we only had a 1-year follow-up; nevertheless, a longer-term follow-up is planned.
A negative effect of this operation is that after removal of the subcutaneous bursa, there is a loss of skin sensation at the back of the heel. Therefore, the patients are carefully informed about this before surgery, and the first 6 weeks after the operation the patients wear a shoe with an open heel. Over time, the skin sensation becomes more normal. Interestingly, no patient has this far raised complaints about the poor skin sensation after surgery; instead, all patients are happy that the burning pain at the back of the heel has disappeared.
To summarize, the advantages using the US- and CD-guided surgical approach are accurate diagnosis using US and Doppler examination, surgery performed in local anesthesia, no need for tendon detachment, immediate weightbearing loading, no need for brace or cast, fast rehabilitation, and need for sick leave only if the patient has a heavy loading occupation.
The results from the current study are good and indicate that the US- and CD-guided surgical method can be efficient in the treatment of chronic painful insertional Achilles tendinopathy. Prospective randomized studies comparing the results between the US- and CD-guided surgical procedure with the Nunley procedure, complications and costs for sick leave, on a material with the same insertional pathology, are needed before strong conclusions can be drawn. For the moment, we suggest that the US- and CD-guided surgical procedure is seen as an additional treatment method for this troublesome condition.
Footnotes
Ethical Approval
Ethics approval was obtained from the Ethical Board in Uppsala-dnr 2022-02889-01. Informed consent was obtained from all patients included in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.