
Abstract
Background:
After astragalectomy, patients still have a shortening of the limb, which can require various reconstructive manipulations. We have developed a simple and versatile tibio-calcaneal-navicular arthrodesis (TCNA) technique to reduce limb shortening.
Methods:
The main difference from the standard method of arthrodesis between the tibia and calcaneus is that in our method after astragalectomy, the tibia rests with the anterior edge against the os navicularis, and the posterior edge against the calcaneus.
We have observed 14 patients (2 were female, 12 were male) operated by a new method of tibio-calcaneal-navicular arthrodesis (TCNA) from 2003 to 2020 years with various forms of osteomyelitis, fractures, and septic necrosis of the talus. The average age of the patients was 42.2 (ranged 20-75) years. Observation results will be assessed using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score 1-1.5 years after surgery and treatment time in the Ilizarov apparatus.
Results:
In all patients, the wounds healed by primary intention. The average time of immobilization in the apparatus was 4.9 (ranged 3.5-6) months. The average limb shortening 2.0 ± 0.5 cm. AOFAS ankle-hindfoot score (n = 14) in all patients came up to 77.9 ± 6.8 (min 68, max 86) SD 12.8. Nonunion was noted in the region of the anterior edge of the tibia in 1 patient (7.1%), and in another patient a painless nonunion was formed (7.1%). Patients wore ordinary footwear without arch supporter and with heels up to 2 cm.
Conclusion:
Good and satisfactory results were obtained in all patients. The new TCNA method allows restoring the supporting ability of a limb, reduces shortening, and improves the quality of life for patients.
Level of Evidence:
Level IV, case series, low-quality cohort or case- control studies.
Keywords
Introduction
Removal of the talus (astragalectomy) is the surgery that is used in modern traumatology and orthopaedics for complex pathology of the talus.
For the first time in 1641, Hildanaus described a patient with astragalectomy. In 1901, Whitman performed astragalectomy in 3 patients with paralytic equinovarus deformity of the foot. After that, this operation became known by his name.5,35
In severe open injuries of the talus, its necrosis or total osteomyelitis, to eliminate the purulent necrotic focus and restore the supporting ability of the patient’s limb, surgeons are faced with the need to perform an operation to remove the talus and create a tibiocalcaneal arthrodesis (TCA). As a result, there is a significant (up to 4-6 cm) shortening of the limb, gait disturbance, and formation of significant deformations of the soft tissues of the ankle joint.5,7,36
Removal of talus is practiced in children with severe rigid foot deformities with arthrogryposis, myelomeningocele, myeloplasia.2,10,12,16,37 Some authors recommend calcaneocuboid fusion after astragalectomy in children to improve the midterm results of surgical treatment. 26 Removal of talus with the subsequent TCA is often performed as a result of osteonecrosis of the talus in adult patients. TCA is currently recommended for patients with symptomatic, secondary consequences of osteonecrosis of the talus body.4,7,17,21,22,34
There are studies on TCA in diabetic Charcot foot, when destruction of the talus is present.3,20 An absolute indication for TCA is a total osteomyelitis of the talus of various genesis—posttraumatic, postoperative, etc.14,18,30,33 Some authors recommend performing astragalectomy with simultaneous TCA for severe fractures and fracture-dislocations of the talus.6,8,9,38 In case of osteomyelitic lesion of the talus, a necessary condition for the elimination of the purulent process is not only astragalectomy and thorough debridement but also the creation of a TCA. For stabilization in place of arthrodesis and elimination of the shortening that it leads to, the external fixation devices and various methods of both free and nonfree bone grafting according to Ilizarov are used.14,30 As the authors show, the patients were satisfied with the results obtained; nevertheless, one of the negative aspects in such procedures is the duration of treatment and the complications arising in the course of treatment that are inherent to bilocal osteosynthesis using the Ilizarov method (eg, suppuration in the area of the wires with prolonged wearing of the apparatus and nonunion in the extension area).13,22 These problems compel surgeons to look for methods of surgical intervention that would reduce the above disadvantages.
The aim of the study, therefore, was to develop a new arthrodesis technique after astragalectomy to reduce limb shortening and to study the results of this operation.
Patients and Methods
Fourteen consecutive patients who underwent astragalectomy using a new TCNA method between 2003 and 2020 were included in this study. This present prospective observational study was performed in accordance with the Declaration of Helsinki and was conducted in patients who voluntarily agreed to a new operation and gave oral informed consent to conduct the study. The operations were performed by one surgeon. This study included patients with septic arthritis and osteomyelitis of the talus and open and closed comminuted fractures of the talus. Patients with Charcot foot, with tumors of the talus, orthopaedic pathology of the feet, and rheumatoid arthritis were excluded. The average age of the patients was 42 (range 23-75) years. Of the 14 patients, 12 were male and 2 were female (Table 1).
Clinical Details of 14 Patients Who Had Talectomy.

Abbreviation: AOFAS, American Orthopaedic Foot & Ankle Society; F, female; L, left; M, male; R, right.
Observation results will be assessed using the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score 1-1.5 years after surgery and treatment time in the Ilizarov apparatus. The magnitude of postoperative shortening was studied. The patients were in the clinic for about 2 weeks. The Ilizarov apparatus was removed on an outpatient basis. After that, patients began to gradually load the leg, and after 20-30 days fully loaded the leg. All patients wore ordinary shoes with a heel of 2 cm.
Figure 1 shows the location of the distal end of the tibia in the area of the removed talus in the new operation (Figure 1A) and that in a conventional one (Figure 1B). We also made calculations on the computed tomographic (CT) image of the movement of the foot to study the subsequent shortening of the limb after astragalectomy. Studies on the CT model of the ankle joint showed that with our method of arthrodesis, the foot is displaced posteriorly by about 2 cm (2,19). The anterior and posterior edges of the tibia descend by about 2.15 cm. The total height of the talus on this CT scan is about 4 cm (3.95) (Figure 1C). The anterior distal angle of the tibia remains largely unchanged at approximately 81 degrees on this CT scan. (Figure 1D). (by Dror Paley, 2003).

Measurements made on computed tomographic scans. (A) New method of arthrodesis. (B) Old method of arthrodesis. (C) Height of the talus; the amount of movement of the anterior and posterior parts of the tibia is indicated. (D) A virtually unchanged anterior distal tibia angle of approximately 81 degrees.
Surgical Technique
Astragalectomy of the talus was performed through the lateral and medial approaches with resection of both ankles. In patients with chronic osteomyelitis after astragalectomy and necrectomy, the destroyed cartilage of the tibia, navicular, and calcaneus was removed. The posterior edge of the tibia was placed in the prepared groove, and the anterior edge of the tibia was compared with the treated surface of the navicular. In patients with fracture-dislocations of the talus, after astragalectomy the cartilage was resected in the region of the anterior and posterior edges of the tibia. The edge of the navicular bone was resected (using a chisel or a rasp, a thin layer of cortical bone was removed until the appearance of “bloody dew”). In the area of the facies articularis talaris posterior of the calcaneus, the cartilage was transversely removed to the bone using a 5- to 10-mm-wide chisel. The posterior edge of the tibia was placed in the prepared groove, and the anterior edge of the tibia was compared with the treated surface of the navicular. The space between the distal tibia and the calcaneus was not filled with anything. The foot was fixed in 2 half-rings from the Ilizarov apparatus using 3 wires. One ring with two 2-mm wires and one 6-mm rod were placed on the lower third of the tibia. The half rings and the ring were interconnected with threaded rods. The difference in the location of the distal end of the tibia in the new and old method
The patient was offered an astragalectomy operation, debridement, TCA, and bilocal osteosynthesis with the Ilizarov apparatus in order to eliminate the shortening. However, the patient refused to lengthen the tibia and gave voluntary consent for a new operation, TCNA.

Radiographs of examples of the results of arthrodesis after astragalectomy by the old and new methods: (A and C) during treatment; (B and D) after the removal of the devices. The yellow arrows indicate the location of the anterior end of the tibia, and the green arrows, edges of the navicular bone.

(A) Radiographs and (B) fistulographs of patient X. The fistulography shows that contrast material fully wraps up the necrotizing talus: (C) during treatment, and (D) after completion of treatment.
Operation
Ankle joint arthrotomy was performed with lateral and medial approach, the lateral and medial malleolus were resected because of their lesion by the osteomyelitis process. It has been found that the talus lies almost freely in its bed. Talectomy was performed.
Debridement
The destroyed cartilage of the tibia and the articular surface of the navicular bone and the calcaneus were removed as they were completely destroyed. Cartilage was removed along the edge of the navicular bone, and its edge was smoothed. The anterior and posterior edges of the tibia were rasped to bloody dew. In the area of the facies articularis talaris posterior of the calcaneus, a groove about 5 mm wide was made with a chisel in the transverse direction. After treating the wound with an antiseptic solution, the posterior edge of the tibia is placed in the prepared groove in the area of the calcaneus, and the anterior edge, devoid of articular cartilage, is placed on the edge of the scaphoid bone. The foot was fixed with the Ilizarov apparatus in accordance with the above method. The wounds were drained and sutured (Figure 3).
The wound healed primarily. The device was removed 4 months after complete fusion, and partial loading (with crutches) was started. Shortening by 2 cm was observed. The patient walks with full load on his leg without any discomfort after 4 weeks.

Radiographs of patient S: (A) closed fraction-dislocation of the talus (duration 2 days); (B) after astragalectomy; (C) after the treatment; (D) a year after the operation; and (E) 4 years after the operation.

(A) Radiographs and (B) ankle view of patient B with an open fracture-dislocation of the talus. (C) Radiograph after astragalectomy. (D) Radiographs and (E) ankle views after end of the treatment. (F) Radiographs after 14 years.

(A) Radiographs before surgery of patient A. (B and C) Intraoperative photographs. (D) Radiographs in the process of treatment. (E) Radiograph 1 year after the operation (patient 6).
Results
All patients underwent a 1-stage operation. The average limb shortening was 2.0 ± 0.5 cm. Mean AOFAS ankle-hindfoot score (n = 14) of the sample was 77.9 ± 6.8 (range 65-86) and SD 12.8 (95% CI for the arithmetic mean). These scores were assessed 1-1.5 years after surgery. In all patients, the wounds healed by primary intention. In 12 patients, the ankylosis obtained was radiographically determined to be good. In 8 patients with osteomyelitis of the talus, the purulent-inflammatory process was completely eliminated. The median time wearing the Ilizarov frame was 4.9 (range 3.5-6) months. A 60-year-old man (7.1%), patient 13, who reported mild foot pain while walking, did not have radiographically determined fusion between the tibia and navicular bone 22 months after surgery, but there was fusion of the posterior edge of the tibia and calcaneus. Painless nonunion was noted in another case (7.1%; patient 11) 19 months after surgery. Patient 13 has moderate pain after a long walk. Patient 11 has a full load in the absence of pain (Figure 7).
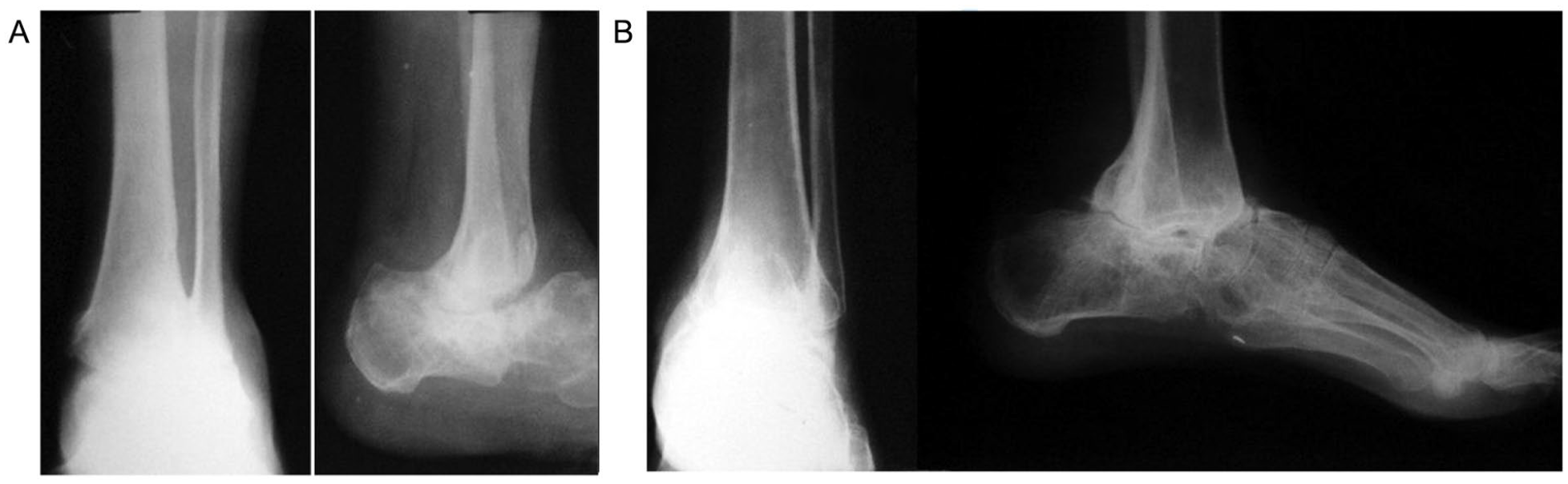
Radiographs of patients: (A) Patient 13, 60 years old, with nonunion of the anterior edge of the tibia 22 months after surgery. (B) Patient 11, 23 years old, with painless nonunion 19 months after surgery.
Biomechanics of walking was mostly maintained. Patients wore ordinary footwear and heels till 2 cm without arch support. Two women aged 70 and 71 years had minor pain in their foot and were using a walking stick. Other patients walk with full weightbearing. Nevertheless, all patients were satisfied with the result. They could move independently and take care of themselves. The condition of the skin and scars did not cause any specific problems due to the reduction in shortening, as can be seen in Figure 5E.
Thus, the proposed method of arthrodesis made it possible to significantly reduce shortening and deformity in the ankle joint.
Discussion
Some authors suggest a more differentiated approach to the question of astragalectomy in osteomyelitis of the talus. Canale and Kelly 1 describe negative results obtained after astragalectomy, which was performed as a result of aseptic necrosis of the talus following a fracture of the neck of the talus. Obviously, this is why others recommend not hurrying with astragalectomy. Saltzman 33 and Riesner et al 29 adhere to the same views. This tactic, in our opinion, increases the suffering of the patient as well as the cost of the treatment process.
On the other hand, with a fracture of the talus according to the classification of fracture of the talus of the Weber/Marti IV or Hawkins III type, a large percentage of subsequent complications and repeated surgeries makes some authors suggest immediately performing an operation to remove fragments of the talus followed by TCA or performing arthrodesis according to Blair.13,24
The use of autografts in order to eliminate the shortening after removal of the talus has been proposed by a number of authors.18,25,27 It is clear that such operations are very traumatic and are absolutely unacceptable in the presence of infection.
If astragalectomy for fractures of the talus or its aseptic necrosis is debated, then with its total osteomyelitis or septic necrosis, this operation is beyond doubt. The presence of an infectious focus excludes any internal fixation after the removal of talus. In this situation, most authors agree that the limb should be fixed with external fixation devices.14,18,22
Some suggest eliminating the shortening caused after astragalectomy by the bilocal osteosynthesis according to the Ilizarov method. This method requires long-term fixation, which slows down the process of social rehabilitation for patients.8,15,19,23,30,32
The TCA operation consists of several sequential procedures: surgical approach, debridement, which is accompanied by astragalectomy, creation of a bed for the contact of the distal end of the tibia and calcaneus, their alignment and stabilization; osteosynthesis; and wound closure. The less traumatic the operation, greater are the chances for success of the treatment—this is the axiom. Therefore, the main difference in the surgical procedures of various authors comes down to reconstruction or to the methods of creating a bed for contact between the distal end of the tibia and the calcaneus. The simpler this stage of the operation, the less traumatic the operation is. Dennison et al 7 suggested resecting the distal end of the tibia and part of the calcaneus after astragalectomy. The shortening was eliminated by osteotomy of the upper third of the tibia and bilocal osteosynthesis according to the Ilizarov method. 7 Fixation in the apparatus was carried out for an average of 10.7 months. The average lengthening was 3.5 cm. The authors point to a large number of various complications in the course of treatment that occur in the bilocal osteosynthesis. Weber et al 36 published the results of treatment of 6 patients who were treated in almost the same way. A slight difference was noted during the resection of the calcaneus. The average time spent in the apparatus was 12 months. 36 In our patients, the average treatment time in the device was 4.9 months. At the same time, the authors point out the absence of similar procedures in the literature. Good results have been obtained; however, similar problems associated with prolonged treatment in the apparatus have been described. Ettinger et al 11 reported on 3 patients (42.9%) treated by an external fixator who had moderate bone fusion radiologically, but a stable, asymptomatic nonunion. Among our patients, only 1 patient (7.1%) had stable and painless neoarthrosis. Rodriguez et al 31 resected the distal end of the tibia in the form of a wedge and created a V-shaped bed on the calcaneus; then the tibia wedge was inserted into the above-mentioned bed and the limb was stabilized with the Ilizarov apparatus. The authors noted that 25% of patients experienced nonfusion. In contrast to the above operations, we only use a chisel to create a transverse bed on the calcaneus of about 5 mm and a rasp to cut the anterior and posterior angles of the tibia and navicular bones. These manipulations exclude resection of the tibia and calcaneus bones. Reinke et al, 28 in their retrospective study of TCA using the Ilizarov apparatus, obtained a stable pseudarthrosis in 4 of 19 patients. On the other hand, the authors used the Ilizarov apparatus on the lower leg, consisting of 3 or 4 rings. In our patients, the device for fixation consists of 1 ring on the lower third of the leg and 2 half rings on the foot, which is much less traumatic and reduces the duration of the operation. The average fixation time was 22 weeks, which is comparable to our observation of 4.9 months. We agree with the authors that tibiocalcaneal arthrodesis is a life-saving operation in case of talus loss and in the presence of infection.
Study Limitations
Our observations are limited to a small number of patients (14). The work included patients with open and closed fracture-dislocation of the talus, chronic osteomyelitis of the talus of various aetiologies. Patients with Charcot foot, with tumors of the talus, and orthopaedic pathology of the feet were excluded. There was no randomization. Finally, no comparative analysis with other methods of arthrodesis for each pathology of the talus was performed.
Conclusion
The obtained results of TCNA allow us to say that this method can be successfully used in patients with purulent inflammation of the talus, its aseptic necrosis, open and closed comminuted fractures, and fracture-dislocations of the talus, who are to undergo astragalectomy. The proposed method of operation allows to reduce the shortening of the limb to 2 cm without any additional surgical procedures. It is less traumatic and its use virtually eliminates the problem of skinfolds resulting from the removal of the talus. Patients can wear ordinary shoes with a heel of 2 cm, and their social rehabilitation is almost completely restored.
Footnotes
Ethical Approval
Ethical Committee of HB Guven Clinic approved this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.