
Abstract
Background:
The peroneus longus (PL) and peroneus brevis (PB) tendons comprise the lateral compartment of the leg and stabilize the foot during weightbearing. Peroneal tendinopathy can precipitate lateral ankle pain and induce functional disability. The progression of peroneal pathology to lateral ankle dysfunction is thought to stem from asymptomatic, subclinical peroneal tendinopathy. There may be clinical benefit to identifying asymptomatic patients with this condition before progression to disability. Various ultrasonographic characteristics have been observed in peroneal tendinopathy. The purpose of this study is to identify the frequency of subclinical tendinopathic characteristics in asymptomatic peroneal tendons.
Methods:
One hundred seventy participants underwent bilateral foot and ankle ultrasonographic examination. Images were assessed for abnormalities of the PL and PB tendons by a group of physicians who recorded frequencies of abnormalities. This team consisted of an orthopaedic surgeon specializing in foot and ankle surgery, a fifth-year orthopaedic surgery resident, and a family medicine physician with musculoskeletal sonographer certification.
Results:
A total of 340 PL and 340 PB tendons were assessed. Sixty-eight (20%) PL and 41 (12.1%) PB tendons had abnormal traits. Twenty-four PLs and 22 PBs had circumferential fluid, 16 PLs and 9 PBs had noncircumferential fluid, 27 PLs and 6 PBs had thickening, 36 PLs and 12 PBs had heterogenicity, 10 PLs and 2 PBs had hyperemia, and 1 PL had calcification. In Caucasian participants, male gender was associated with increased frequency of abnormal findings, but there were no other significant differences based on age, body mass index, or ethnicity.
Conclusion:
In our studied population of 170 patients who had no complaints of associated symptoms, we found that 20% of PLs and 12% of PBs displayed ultrasonographic abnormalities. When we included all unusual findings within and around the tendons, prevalence rates of ultrasonographic abnormalities were 34% for PLs and 22% for PBs.
Level of Evidence:
Level II, prospective cohort study.
Introduction
The peroneus longus (PL) and peroneus brevis (PB) are in the lateral compartment of the lower leg and function primarily to evert and pronate the foot, while secondarily plantarflexing the ankle. 9 Additionally, these tendons work to stabilize the foot during weightbearing, which can lead to overuse injuries. These muscles are the first to contract in response to ankle inversion and are thus at risk of sustaining injury during acute forceful inversion stress as seen with a common ankle sprain.3,10,12 Peroneal tendon dysfunction can manifest as tendinosis, tenosynovitis, tendinopathy, degenerative or acute rupture, or subluxation.12,13
The incidence of peroneal tendon pathology is currently unknown, in part due to missed or misdiagnosis of peroneal dysfunction. 2 It has been demonstrated that there is often a protracted delay from the onset of symptoms to the diagnosis of peroneal injury in both acute and attritional injuries.2,17 Even then, only about 60% of peroneal tendon disorders are accurately diagnosed at the first clinical evaluation. 6 When left untreated, peroneal tendinopathy can precipitate lateral ankle pain and functional disability.1,4,15,16
In addition to acute peroneal tendon ruptures, peroneal pathology can progress chronically to incite lateral ankle dysfunction, which is thought to stem from initially asymptomatic peroneal tendinopathy.1,7 Although in some patients this tendinopathy can remain subclinical, other patients can develop functional limitation of the lateral ankle. In fact, among patients undergoing surgery for chronic lateral ankle instability, more than three-fourths had peroneal tenosynovitis, whereas more than half had an attenuated peroneal retinaculum and one-quarter had a peroneus brevis tear. 5 The underlying course by which some patients with peroneal tendinopathy remain asymptomatic whereas other patients develop significant dysfunction has not been elucidated. As such, there may be clinical benefit to identifying asymptomatic, subclinical peroneal tendinopathy before it causes disability. Recently, some features of subclinical tendinopathy have been observed with modern ultrasonography (US).
Ultrasonography has emerged as a widely used imaging technique to aid in the diagnosis of many conditions. Because of its low cost and high resolution, and ability to record dynamic images, US has become a key resource in the evaluation of musculoskeletal pathology. 18 Peroneal tendinosis can present as hypoechoic swelling, and peroneal tenosynovitis can be visualized with tendon thickening, synovial effusion, and a hypoechoic synovial sheath on US.8,11 As such, US can be used to identify asymptomatic, subclinical peroneal tendinopathy before progression to more severe clinical dysfunction. Despite this utility, the frequency of these abnormal US findings in asymptomatic peroneal tendons has not been previously described in a large cohort. The purpose of the present study is to identify the frequency of subclinical tendinopathic characteristics in asymptomatic peroneal tendons to aid physicians in diagnosing peroneal tendinopathy before progression to more severe disease.
Methods
Following IRB approval, patients presenting to an orthopaedic foot and ankle clinic were given the opportunity to participate in this study. Participants were asked to provide demographic information, along with a medical and social history. Patients were excluded if they were under the age of 18 years, reported symptoms associated with peroneal tendon dysfunction (by history or physical examination during the visit), demonstrated lesions or ulcers over the ultrasonographic examination site, or were diagnosed with a related condition (eg, acute ankle sprain or chronic ankle instability).
The bilateral US examination of the foot and ankle was conducted by a single registered musculoskeletal sonographer (RMSKS) using a GE (GE Healthcare, Chicago, IL) LOGIQ e US machine with L8-18i-RS transducer. The supra- and inframalleolar portions of the peroneus longus and peroneus brevis tendons were the focus of this examination. A static image of each of these tendons was saved; 1 cm above and below the tip of the lateral malleolus and both the long axis (LA) and transverse (TRV) measurements were obtained.
The reviewers had a collective meeting to review pathology, terminology, and determine how we would categorize each type of pathology. Saved static images were then reviewed by a group of physicians, which consisted of a board-certified orthopaedic surgeon specializing in foot and ankle surgery, a fifth-year orthopaedic surgery resident, and a board-certified family medicine physician with an RMSKS certification. The images from each of the 170 patients were independently reviewed by the physicians, who recorded their findings and classified each image as either normal or abnormal. Abnormalities, which suggests potential tendinopathy, were subclassified based on the following findings: circumferential fluid around the tendon, noncircumferential fluid around the tendon, thickening of the tendon, heterogeneity of the tendon, hyperemia within the tendon on color doppler US examination, calcification within the tendon, hyperechogenicity of the tendon, hypoechogenicity of the tendon, and anechogenicity of the tendon.
The group then convened to reevaluate and discuss any image that did not receive the same classification by all 3 physicians until a consensus was reached. A SANYO WXGA Projector displaying high-definition images at a wide XGA 1280 × 800 (16:10) resolution was used during the collaborative review.
Statistical Analysis
The US findings for each patient’s PLs and PBs were classified as either normal or abnormal for statistical analysis. Multivariable logistic regression (based on variables such as age, sex, body mass index [BMI], and ethnicity) was the primary mode of analysis. Standard variables (eg, mean, median, mode) were also calculated for these variables.
Results
A total of 170 participants who underwent US examination met inclusion criteria. Overall, 340 PLs and 340 PBs were assessed and included in this study. In addition, 53 (31.2%) participants were male and 117 (68.8%) were female; 99 patients (58.2%) were Caucasian, 65 (38.2%) were African American, and the ethnicity of the remaining 3.6% of participants was classified as other (Table 1).
Mean Age and BMI of Participants by Tendon Findings. a
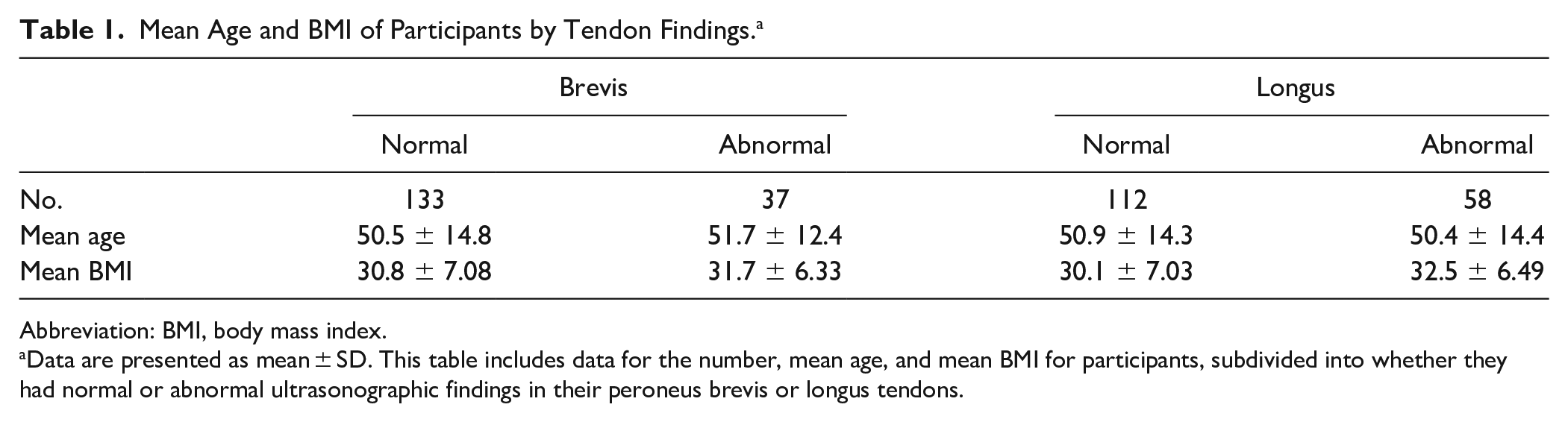
Abbreviation: BMI, body mass index.
Data are presented as mean ± SD. This table includes data for the number, mean age, and mean BMI for participants, subdivided into whether they had normal or abnormal ultrasonographic findings in their peroneus brevis or longus tendons.
From the 340 PLs and PBs scanned, 68 (20%) PLs and 41 (12.1%) PBs were noted to have ultrasonographic abnormalities (Table 2). Two-thirds (65.9%) had PLs that were considered normal bilaterally, and 78.2% had PBs that were both normal. PL abnormalities were found in 37.4% of Caucasian participants and 27.7% of African American participants. PB abnormalities were recorded for 23.2% of Caucasian patients and 18.5% of African American patients (Table 3).
Frequency of Ultrasonographic Findings in Assessed Tendons (n = 340). a

This table provides the frequency of each ultrasonographic finding in the peroneal tendons assessed.
Frequency of Ultrasonographic Findings in Participants (n = 170). a

This table provides the frequency of each ultrasonographic finding as the number of study participants it was observed in.
The most prevalent abnormality in PLs was heterogeneity, found in 32 participants (18.8%). Following heterogeneity, frequency of abnormal traits in PLs (in order of greatest to least) were as follows: tendon thickening (18.8%), circumferential fluid (12.4%), noncircumferential fluid (8.8%), hyperemia (5.9%), and calcification (0.6%).
In PBs, the most observed abnormality was circumferential fluid, seen in 19 (11.2%) participants. In order of prevalence, circumferential fluid in PBs was followed by heterogenicity (5.9%), noncircumferential fluid (5.3%), tendon thickening (3.5%), and hyperemia (1.2%).
Based on the results of multivariable logistic regression in this study population, male gender was shown to be a significant risk factor in Caucasian participants for the presence of abnormal US traits in PB tendons (P = .028; OR 9.32, 95% CI 1.27, 68.43) (Supplemental Table S2). However, this correlation of gender and abnormal traits was not shown to be significant for PL tendons or African American participants (Table 4) (Supplemental Table S1).
Results of Multivariable Logistic Regression Analysis. a

Abbreviation: BMI, body mass index.
This table lists the P values, odds ratios, and 95% CIs for the association between multiple exposures (male gender, increased BMI, increased age, and race) and the outcome of having abnormal ultrasonographic traits observed in the peroneal tendons on ultrasonography for all study participants.
Discussion
The underlying course through which patients develop clinically significant dysfunction of the PL and PB muscle tendon unit leading to symptomatic pathology is not yet fully elucidated. However, the progression of this disease is thought to develop from asymptomatic tendinopathy,1,7 which is apparent only through radiographic evidence of disease. As such, there may be clinical benefit to early detection of subclinical peroneal tendinopathy before it causes functional limitation. The PL seemed to have higher rates of heterogenicity, which may be a precursor to tendinopathy, whereas the PB had circumferential fluid, which could be a marker for future tendinitis. The etiology of the differential rates of findings in our study may be due to the types and amount of stress placed across these tendons. However, that is speculation and these findings may warrant future study.
Caucasian males were found to have increased odds of abnormal US findings of the PB tendon (P = .028). There was not statistical significance for the prevalence of abnormalities of the PL tendon in Caucasian males (P = .079). For African American participants, male gender was not seen to have an impact on the prevalence of abnormal US findings in either the PL or PB tendons (PL, P = .995; PB, P = .829).
Increasing BMI has been shown in other studies to correlate with the development of foot and ankle tendinopathy. Yet, for both the PL and PB tendons, increasing BMI was not statistically significant (PL, P = .137; PB, P = .359). When controlled for ethnicity, increasing BMI did not demonstrate significant differences in the presence of abnormal US findings for PB tendons in Caucasian participants (P = .083) compared to African American participants (P = .542). A similar study, which shared participants with the current study, focused on identifying the prevalence of US findings in posterior tibial tendons (PTTs). 14 Increased BMI was a significant risk factor for the prevalence of abnormal US findings of PTTs in African American participants, which is different from the findings of this study of the peroneal tendons. Also in this study, Caucasian participants were found to have almost 3 times higher odds of having abnormal US findings of the PTT. The current study was not able to reproduce this difference based on ethnicity (PL, P = .379; PB, P = .99) for peroneal tendons. Increasing age was not found to be a significant risk factor for abnormalities in either peroneal tendon (PL, P = 0.764; PB, P = 0.809).
There are limitations of this study. This study’s population was not followed longitudinally (after initial enrollment and US examination) to determine how many patients that presented with asymptomatic US findings eventually progressed to symptomatic peroneal tendinopathy. Also, 170 participants were included in the study, but when performing multiple analyses this number led to reduced statistical power when stratifying variables. All participants were patients presenting to one center, so these results may not be generalizable. Additionally, this study excluded participants who were actively symptomatic with peroneal tendinopathy. However, these were patients presenting to a foot and ankle clinic, so it is possible that some participants were included if they were not transparent about the extent of their symptoms. Because we excluded symptomatic patients, we were unable to correlate abnormal US traits with specific physical examination findings. Also, our US findings were not correlated with other imaging such as magnetic resonance imaging, even though the sensitivity and specificity of US have been shown to be comparable to that of magnetic resonance imaging. Finally, US is very operator dependent, and we did not study interexaminer variability.
This study adds to the limited data regarding image-diagnosed peroneal pathology in asymptomatic patients and establishes a baseline for prevalence of abnormal US findings in PL and PB tendons. This baseline will serve as a foundation for subsequent studies looking to correlate these findings with the development of symptomatic peroneal pathology and aid in the understanding of incidental abnormal ultrasonographic findings. The high rate of abnormal tendons identified in asymptomatic patients emphasizes the importance of performing a detailed history and physical in conjunction with diagnostic imaging in order to determine risks of progression and disease treatment.
Conclusion
In this population of 170 patients who had no complaints of associated symptoms we found that 20% of PLs and 12.1% of PBs displayed ultrasonographic abnormalities. For Caucasian participants, male gender showed a significant (P = .028) increase in frequencies of abnormal findings in the PBs. No other demographic metrics (age, gender, or BMI) showed significantly increased findings in the PLs or PBs for the rest of the study population.
Footnotes
Appendix
Results of Multivariable Logistic Regression Analysis for Caucasian Participants. a

| Brevis | Longus | |||||
|---|---|---|---|---|---|---|
| Risk factor | P value | Odds ratio | 95% CI | P value | Odds ratio | 95% CI |
| Male gender | .028 b | 9.32 | 1.27, 68.43 | .079 | 3.701 | 0.86, 15.92 |
| BMI | .083 | 1.16 | 0.981, 1.36 | .253 | 1.063 | 0.96, 1.18 |
| Age | .679 | 1.01 | 0.95, 1.08 | .411 | 0.979 | 0.93, 1.03 |
Abbreviations: BMI, body mass index.
This table lists the P values, odds ratios, and 95% CIs for the association between multiple exposures (male gender, increased BMI, increased age) and the outcome of having abnormal ultrasonographic traits observed in the peroneal tendons on ultrasonography for the Caucasian study participants.
Statistical significance defined as P ≤.05.
Ethical Approval
Ethical approval for this study obtained from the University of South Carolina Institutional Review Board (Pro00038618)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.