
Abstract
Background:
Manuscripts discussing return to play (RTP) following ankle surgery are common. However, the definition for RTP and the method by which it is determined remains unclear. The purpose of this scoping review was to clarify how RTP is defined following ankle surgery in physically active patients, to identify key factors informing RTP decision making (such as objective clinical measures), and make recommendations for future research.
Methods:
A scoping literature review was performed in April 2021 using PubMed, EMBASE, and Nursing and Allied Health databases. Thirty studies met inclusion criteria: original research following ankle surgery reporting at least 1 objective clinical test and documentation of RTP. Data were extracted for study methods and outcomes (RTP definition, RTP outcomes, and objective clinical tests).
Results:
The scoping review found studies on 5 ankle pathologies: Achilles tendon rupture, chronic lateral ankle instability, anterior ankle impingement, peroneal tendon dislocation, and ankle fracture. RTP criteria were not provided in the majority of studies (18/30 studies). In the studies that provided them, the RTP criteria were primarily based on time postsurgery (8/12) rather than validated criteria. Objective clinical outcome measures and patient-reported outcome measures (PROMs) were documented for each surgery when available. Both clinical outcomes and PROMs were typically measured >1 year postsurgery.
Conclusion:
In physically active patients who have had ankle surgery, RTP remains largely undefined and is not consistently based on prospective objective criteria nor PROMS. We recommend standardization of RTP terminology, adoption of prospective criteria for both clinical measures and PROMs to guide RTP decision making, and enhanced reporting of patient data at the time of RTP to develop normative values and determine when the decision to RTP is not safe.
Level of Evidence:
Level IV, scoping review.
Introduction
It is well documented that ankle injuries are common in sport.17,21 Of particular interest, severe ankle injuries requiring surgical intervention can have sweeping effects on the athlete, causing lost time in training and competition, lost opportunity, lost income, and incurred medical costs.5,44 Fortunately, surgical techniques have evolved greatly over the last 15 years and may offer improved clinical outcomes (such as faster return to sport, higher percentage of patients who are able to return to sport) to those who require surgery after failed conservative management. 36
Postoperatively, the goal of the medical team is to return the athlete to participation as quickly and safely as possible. This postoperative return to play (RTP) should take into account multiple factors, including, but not limited to, soft tissue healing timelines, rehabilitation progress defined by objective clinical measures (eg, full range of motion [ROM], strength 90% of uninjured limb), subjective patient-reported instruments, sport risk assessment, and psychological readiness.10,47 The decision should be made with contributions from within the medical team (eg, physician, physical therapist, athletic trainer) as well as the athlete’s performance support system (eg, sport coach, strength coach). Historically postsurgical RTP decisions were primarily influenced by the surgical procedure performed and soft-tissue healing time frames, whereas modern sources recommend inclusion of these factors into a more comprehensive approach.1,10,19,47 Data to support readiness for sport can be drawn from the results of validated subjective and objective outcomes measures, sport-specific testing, and psychological readiness tools.1,10,19,47 However, it does not appear that recommendations for criteria-based RTP decision making are being fully implemented after ankle injury. For example, one systematic review of nonoperative lateral ankle sprains failed to identify a single study that used a prospective, criteria-based RTP decision-making process. 47 A similar review of operative management of common ankle injuries has not been performed to date.
Furthermore, there is a lack of clarity and great variability in how RTP and return to sport (RTS) are defined. Is RTP the point at which the athlete participates in their first day of restricted training? Is it once the athlete can engage in unrestricted training? Or is it back to preinjury competitive levels? It has been proposed that the RTP process should be viewed as a continuum through several steps. 47 Tassignon et al 47 applied a set of operational definitions 1 for athlete status post ankle injury, providing a progression from (1) the time the athlete is still in rehabilitation but beginning to participate in their sport perhaps in a controlled environment, and at a level lower than his or her return to sport goal (return to participation [RTPa]), through (2) the time when the athlete is playing without restrictions but not at his or her desired performance (return to sport [RTS]), and finally (3) when the athlete is performing at or above his or her preinjury level (return to performance [RTPf]). In musculoskeletal injuries treated surgically, the surgeon typically provides orthopaedic clearance for the introduction of athletic activity (aligning with the concept of RTPa), identifying that it is safe to begin the process of return to athletic activity, whereas ongoing rehabilitation and the transition to RTS are commonly led by the physical therapist and/or athletic trainer. Resources and level of sport (eg, professional vs recreational) will affect the composition of the athlete’s medical team as they progress through RTPa, RTS, and RTPf. Although the definitions proposed by Tassignon et al 47 may be helpful in the future, current research often uses RTP or RTS interchangeably without specifying the exact stage in the continuum. We will use the term RTP where a more precise definition is lacking.
Scoping reviews are a relatively new concept in the research literature and aim to determine the coverage of the body of literature on a certain topic.32,48 They can be especially useful to clarify key concepts or definitions in the literature (eg, RTP) and to identify key characteristics or factors related to a concept (eg, RTP criteria or measurement). 32 In contrast, a systematic review typically focuses on the outcomes of the reviewed studies, which was not the focus of the current research question. 32 Therefore, a scoping review design was adopted. The purpose of this scoping review was to clarify how RTP is defined following ankle surgery in physically active patients, to identify key factors informing RTP decision making, and make recommendations for future research.
Methods
Literature Search
We conducted a scoping review, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for scoping reviews. 48 The search query was performed on April 12, 2021, in the following registries: PubMed, EMBASE, and Nursing and Allied Health Database. Studies were limited to the past 15 years (published between January 1, 2006, and April 2021). Results were restricted to peer-reviewed literature published in the English language. Key words were organized into 3 strings—string 1: ankle OR talocrural OR hindfoot OR rearfoot OR tibiotalar OR subtalar; string 2: surgery OR operative OR open repair OR arthroscopy; and string 3: return to sport OR return to play OR return to performance. Each string was connected in the search using the Boolean operator “AND.” A representative search strategy is shown in Figure 1.

Representative search strategy.
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (1) patients are adults (>18 years old) engaged in any level of physical activity or sport; (2) patients underwent surgery in the region of the ankle joint (eg, Achilles repair, lateral ligament repair or reconstruction, peroneal tendon repair, and fracture fixation); (3) the study reports at least 1 objective clinical test (eg, ROM, strength measure, balance test, and functional test); (4) the study reports RTP data regardless of how it was labeled, including RTS, RTPa, RTPf (eg, RTP criteria, time to RTP, or % RTP); and (5) the study is original research including randomized controlled trial, cohort, case-control, or case series in design.
Studies were excluded if they were (1) not in English, (2) not available as a full-text manuscript (eg, published abstract only), (3) not-peer reviewed, (4) did not report surgical outcomes, (5) were not published in the last 15 years, or (6) were a review, commentary, or case-study. We limited criteria to studies published in the last 15 years as surgical techniques and associated healing times are constantly evolving and we aimed to capture relatively recent trends. 36
Study Selection
The results of the search strategy were compiled into a spreadsheet. Duplicate entries and search results that were clearly not full-text articles (eg, published abstracts, conference proceedings) were removed. In the first round of screening, 2 independent reviewers with subject knowledge and research experience screened the title of all publications for relevance to the topic and appropriate article type (full-text, original research). Publications deemed irrelevant (not related to surgical outcomes at the ankle region), abstracts (not full-text), and review articles (not original research) by both reviewers after screening the title were removed from the search.
All remaining publications were retained for a second round of review. In the second round, the same 2 independent reviewers screened the title and abstract of all remaining publications for inclusion or exclusion eligibility criteria. Publications deemed ineligible by both reviewers after screening the title and abstract were removed from the review, and any disagreements were resolved by discussion. All remaining publications were retrieved for full-text review. After full-text review, publications deemed ineligible by both reviewers were removed from the review, and the reason for removal was documented. Any disagreements were resolved by discussion. All remaining publications were included in the review. Results are shown in Figure 2.

Systematic search and screening process.
Data Extraction
Following approval for inclusion, 2 independent investigators (CJW and ABJR) extracted the relevant data, including study design, pathology, patient characteristics, surgical procedures, criteria for patient to be released to RTP, time until RTP, percentage of cohort that RTP, name and type of objective clinical measures obtained, timing of objective clinical measures, and type of patient-reported outcome measures (PROMs) reported. Results were synthesized descriptively and utilizing frequency counts.
Evaluation of Study Quality
Study quality was assessed using one of 3 National Institute of Health quality assessment tools: (1) the tool for controlled intervention studies, (2) the tool for case-control studies, or (3) the tool for case series studies. 43 Study design dictated which tool was used. For all tools, higher scores indicated higher study quality.
Results
Characteristics of Included Studies
After applying the inclusion criteria, 30 studies were included in this scoping review (Figure 2). Study characteristics are detailed in Table 1, study methods are detailed in Tables 2 to 4. Although all ankle surgical procedures were eligible for inclusion, only 5 conditions were represented within the included studies: Achilles tendon rupture (16 articles),4,6 -8,12,20,26 -29,34,39,40,45,46,49 chronic ankle instability (9 articles),9,15,16,18,23,25,37,50,52 anterior ankle impingement (2 articles),14,30 peroneal tendon dislocation (1 article), 13 and ankle fracture (2 articles).31,42 There were 1442 patients across all studies, with individual studies averaging 48.1 ± 32.5 patients (range: 8-126). Surgical procedures varied by pathology. Study designs were most commonly cohort (19 studies) or case series (10 studies), with just 1 randomized controlled trial. Within the limitations of study design, study quality was typically moderate (average quality score 86.8% ± 11.4%, range 55-100; Supplemental Table).
Included Studies’ Characteristics.

Abbreviations: ATFL, anterior talofibular ligament; ♂, males; ♀, females.
Activity level was defined on a spectrum from recreational (lowest) to competitive to elite (highest). Not specified indicates the article omitted any information about level of activity in their methods or return to sport data.
Summary of Return to Play Criteria in Studies of Surgical Management of Achilles Tendon Rupture.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Score; ATRS, Achilles Tendon Rupture Score; FADI, Foot and Ankle Disability Index; po, postoperative; PROMs, patient-reported outcome measures; ROM, range of motion; RTP, return to play; VAS, visual analog scale; VISA-A, Victorian Institute of Sports Assessment–Achilles; VNRS, verbal numeric rating scale.
If data were available for multiple time points (eg, at 6 and 12 months), only data at last follow-up were included here.
Summary of Return to Play Criteria in Studies of Surgical Management of Chronic Ankle Instability.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Score; FAAM-ADL, Foot and Ankle Ability Measure–activities of daily living scale; FAAM-Sports, Foot and Ankle Ability Measure–sports scale; FAOS, Foot and Ankle Outcome Score; KAFS, Karlson Ankle Function Score; KSS, Knee Society Score; NWB, nonweightbearing; po, postoperative; PROMs, patient-reported outcome measures; ROM, range of motion; RTP, return to play; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Summary of Return to Play Criteria in Studies of Surgical Management of Other Ankle Pathologies.
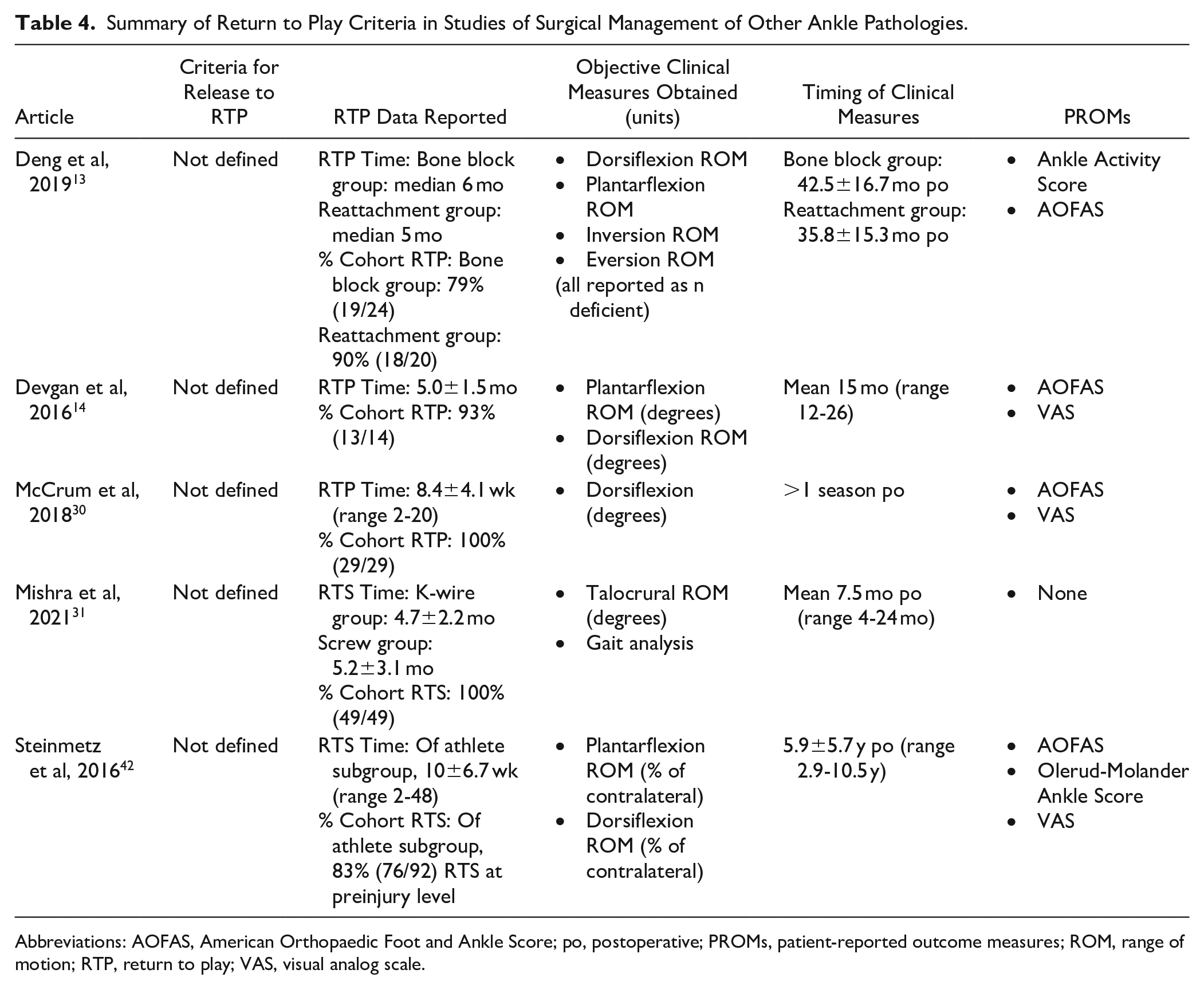
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Score; po, postoperative; PROMs, patient-reported outcome measures; ROM, range of motion; RTP, return to play; VAS, visual analog scale.
RTP Decision Making After Surgery for Achilles Tendon Rupture
Criteria for release to RTP
There were 16 studies in the Achilles tendon rupture subgroup. Criteria for release to RTP was provided in 5 of the 16 studies (Table 2).6,7,26,34,46 Specifically, 3 studies provided purely time-based criteria for allowing RTP, each with a different time interval (ranging from 3 to 6 months).7,34,46 One study allowed RTP if both time and a clinical measure were met (eg, >6 months as strength allowed). 26 Another study allowed RTP if both time and a subjective criterion were met (eg, >3 months then based on patient comfort). 6 The time until RTP was reported in 11 studies.4,8,12,26,27,34,39,40,45,46,49 The percentage of the cohort to return to sport was reported in 14 studies.4,6,7,12,20,26 -29,39,40,45,46,49 Of these 14 studies, 8 specified that the RTP was at preinjury levels,6,7,12,20,27,28,39,45 whereas 6 did not specify the level at which patients RTP.4,26,29,40,46,49
Objective clinical measures obtained
The most common objective clinical measurements were calf circumference (n = 11), strength (n = 9), heel rise test or height (n = 8), ROM (n = 8), jump or hop test (n = 3), and the Achilles tendon resting angle (n = 2). All other measures were used in a single study, including Matles test, 28 ultrasonographic depth and length of tendon, 29 3-dimensional gait analysis, 46 and Achilles Tendon Performance Test. 46
PROMs
The most common PROM utilized was the American Orthopaedic Foot & Ankle Society Score (AOFAS, n = 10),4,8,28,29,34,39,40,45,46,49 Achilles Tendon Rupture Score (ATRS, n = 10),4,6 -8,12,26,29,34,45,49 Tegner activity scale (n = 4),6,7,20,28 visual analog scale (VAS, n = 4),12,28,34,40 and Victorian Institute of Sports Assessment–Achilles (n = 2).27,29 All other PROMs were used in a single study, including Trillat, 46 Halasi, 7 patient perception of performance, 7 Physical Activity Score, 7 Arner-Lindholm, 39 Foot and Ankle Disability Index, 40 patient satisfaction. 45
Timing of clinical measurements
Objective clinical measures and PROMs were commonly collected 1-2 years postoperatively (range 6 weeks–10 years).
RTP decision making after surgery for chronic ankle instability
Criteria for release to RTP
There were 9 studies in the chronic ankle instability subgroup.9,15,16,18,23,25,37,50,52 Criteria for release to RTP was provided in 7 of the 9 studies (Table 3).15,16,18,23,37,50,52 Specifically, 3 studies provided clinical criteria for allowing (eg, start RTP when no swelling present with jogging, full-ankle ROM and strength, >90% strength).18,23,37 Four studies provided purely time-based criteria for allowing RTP (eg, postoperative week 8, after 3 months).15,16,50,52 The time until RTP was reported in 6 of the 9 studies.9,15,16,18,23,50 Eight of 9 reported the percentage of the cohort to return to sport,15,16,18,23,25,37,50,52 with 2 of these specifying that the RTP was at preinjury levels.
Objective clinical measures obtained
The most common objective clinical measurements were laxity (n = 7) and ROM assessment (n = 4). Other less common objective clinical measurements included joint position sense, hop test, and calf girth.
PROMs
The most common PROMs utilized were the AOFAS (n = 6),9,15,16,25,50,52 VAS (n = 4),9,15,16,50 and Karlsson Ankle Function Score (n = 3),15,16,25 and the Foot and Ankle Outcome Score (n = 2).23,37 Other less common objective clinical measurements included Tegner, 25 Foot and Ankle Ability Measure (FAAM), 9 Japanese Society for Surgery of the Foot score, 18 Kaikkonen total score, 23 and Knee Society Score 18 (each utilized in n = 1 studies).
Timing of clinical measurements
Objective clinical measures and PROMs were most commonly collected 1-2 years postoperatively (range 12 weeks to 4 years).
RTP decision making after surgery for other ankle pathologies
Criteria for release to RTP
There were 5 studies in this category, which included pathologies such as anterior ankle impingement (2 studies),14,30 peroneal tendon dislocation (1 study), 13 and ankle fracture (2 studies).31,42 Criteria for release to RTP was not provided in any of the articles in this category (Table 4). The time until RTP and percentage of the cohort to RTP were reported in all studies (n = 5).
Objective clinical measures obtained
All articles reported measuring ankle ROM (n = 5).13,14,30,31,42 Only 1 article reported additional clinical measures, and they reported gait analysis. 31
PROMs
The most common PROMs were AOFAS (n = 4),13,14,30,42 then VAS (n = 3).14,30,42 The Ankle Activity Score 13 and Olerud-Molander Ankle Score 42 were each used once.
Timing of clinical measurements
Objective clinical measures and PROMs were all collected 4 months to 10.5 years postoperatively.
Discussion
The purpose of this scoping review was to clarify how RTP is defined following ankle surgery in physically active patients, to identify key factors informing RTP decision making, and make recommendations for future research. Overall, the review found no definitions of RTP, few provided prospective RTP criteria, and there was inconsistent use of objective clinical outcome measures. Our findings suggest that gaps in the literature may impact RTP decision making and the ability to provide accurate postoperative expectations after injury.
Definition of RTP in Ankle Surgical Literature
Past research has found variability in the literature relative to the definition (or lack thereof) of the term RTS or RTP. None of the 30 studies included in this review defined RTP, so it is unknown if the studies were using the term RTP to refer to the stage in the athlete’s progression when they reached RTPa, RTS, or RTPf (using the classification system proposed by Tassignon et al 47 ). This can cause unequal comparisons. For example, in a prior meta-analysis of RTP after Achilles rupture, Zellers et al 53 found that studies that did not use criteria to determine or define RTP reported an 11% higher RTP among their cohort than studies who did use criteria. This may indicate that it was easier to classify a patient as fully RTP when not held to prospectively defined criteria or definitions. Future research should utilize more precise terms. We (the 3 orthopaedic surgeon authors) prefer to use the term “orthopaedically cleared” at time of RTPa when releasing a postoperative patient to their physical therapist or athletic trainer’s care.
Criteria for Release to RTP in Ankle Surgical Literature
In Achilles repair literature, only 6 studies (33%) reported prospective criteria for release to RTP. Criteria included time alone,7,34,46 time and strength (although no objective strength target was specified), 26 and time and patient comfort. 6 In contrast, most chronic ankle instability surgical outcomes studies (n = 7, 78%) reported prospective criteria for release to RTP.15,16,18,23,37,50,52 Again, most studies reporting criteria included time,13,15,16,18,23,52 although some additionally included criteria such as full ROM, ≥90% ankle strength, and/or functional tests.15,18,23,37 None of the ankle impingement, peroneal tendon, or ankle fracture studies reported criteria for RTP clearance.13,14,30
Even for studies in which criteria for RTP included objective clinical measures or PROMs, no data were provided at the time of RTP. For example, if strength were a criteria, the study might report an objective clinical measure of strength an average of 72 months postoperatively, whereas RTP occurred at approximately 5 months postoperatively. 26 Only a minority of studies (n = 6, 20%) reported objective clinical data or PROMs in a time frame that may have corresponded to RTP (eg, at 6 weeks, 3 months, or 6 months).6 -8,29,34,52 Although their data offer clinically useful information closer to the likely time of RTP, it would be preferred if these type of data were reported at the actual time of RTP.
None of the included studies included objective data on workload from tools such as global positioning system (GPS) or other activity monitoring systems that are increasingly being used in elite sports. Utilizing GPS technology to capture workloads and translate the understanding of sport demands to enhancing RTP has been a topic in recent literature.24,38 We believe GPS technology or other activity monitoring systems could provide valuable information toward safe and effective RTP progression, and should be included in future research.
Objective Clinical Tests Used in Ankle Postsurgical Outcomes Studies
The objective clinical tests reported trended toward reflecting the unique aspects of each pathology and subsequent surgical procedure. For example, surgical management of Achilles rupture requires rehabilitation to minimize tendon elongation and maximize plantarflexion strength to withstand the demands of load required in sport.3,51,54 As such, it is no surprise that the 3 most common objective clinical tests were calf circumference (a measure of atrophy), strength measures, and the heel rise test. Similarly, the most common objective clinical tests used in the chronic ankle instability literature were laxity and ROM, likely reflecting the primary goal of these procedures to restore joint stability. Surgical interventions of anterior ankle impingement and ankle fracture also focused on ROM, which fits with the surgical indications. However, the only objective clinical measure reported following peroneal tendon dislocation was ROM (not peroneal strength). Thus, although the objective clinical tests reported trended toward reflecting the unique aspects of each pathology, the trend was not consistent across all reports.
PROMs Used in Ankle Postsurgical Outcomes Studies
All but 1 study 31 used at least 1 PROM. Across all conditions, the 4 most common PROMs were the AOFAS22,33 (n = 20), ATRS 35 (n = 10), VAS (n = 11), and Tegner activity scale (n = 6). Although the AOFAS was the most commonly used PROM, it has several issues—including validation and a noted ceiling effect.11,33 If using validated instruments, PROMs should be a helpful tool to identify patient status at the time of RTP. Future research should identify PROMs that provide the clinician tasked with evaluating readiness to RTP with valuable data to inform decision making. The ideal PROM will be validated for a specific injury or body region and be able to capture the highest level of function that meets the athlete’s goals. Additionally, evidence suggests that PROMs are also important in evaluating psychological factors that may affect athletes’ confidence to RTP.2,41 However, psychological readiness instruments were not used in any of the studies in this review.
Limitations
Our scoping review was limited to studies reporting postoperative RTP, excluding conditions that may be managed conservatively. Additionally, our search was limited to English-language articles that may induce bias. The study quality was varied, which may impact results. However, the impact of study quality is limited by our study design, as we were not analyzing surgical outcomes directly but rather analyzing RTP criteria and objective clinical outcomes measures.
Conclusions
In physically active patients post ankle surgery, RTP remains largely undefined and is not based on prospective objective criteria. Additionally, there is large variation in selection and timing of clinical measures and PROMs. We recommend that future research provide prospective RTP criteria that uses both objective clinical measures and validated PROMs obtained at the time of RTP decision making to evaluate readiness to RTP.
Footnotes
Appendix
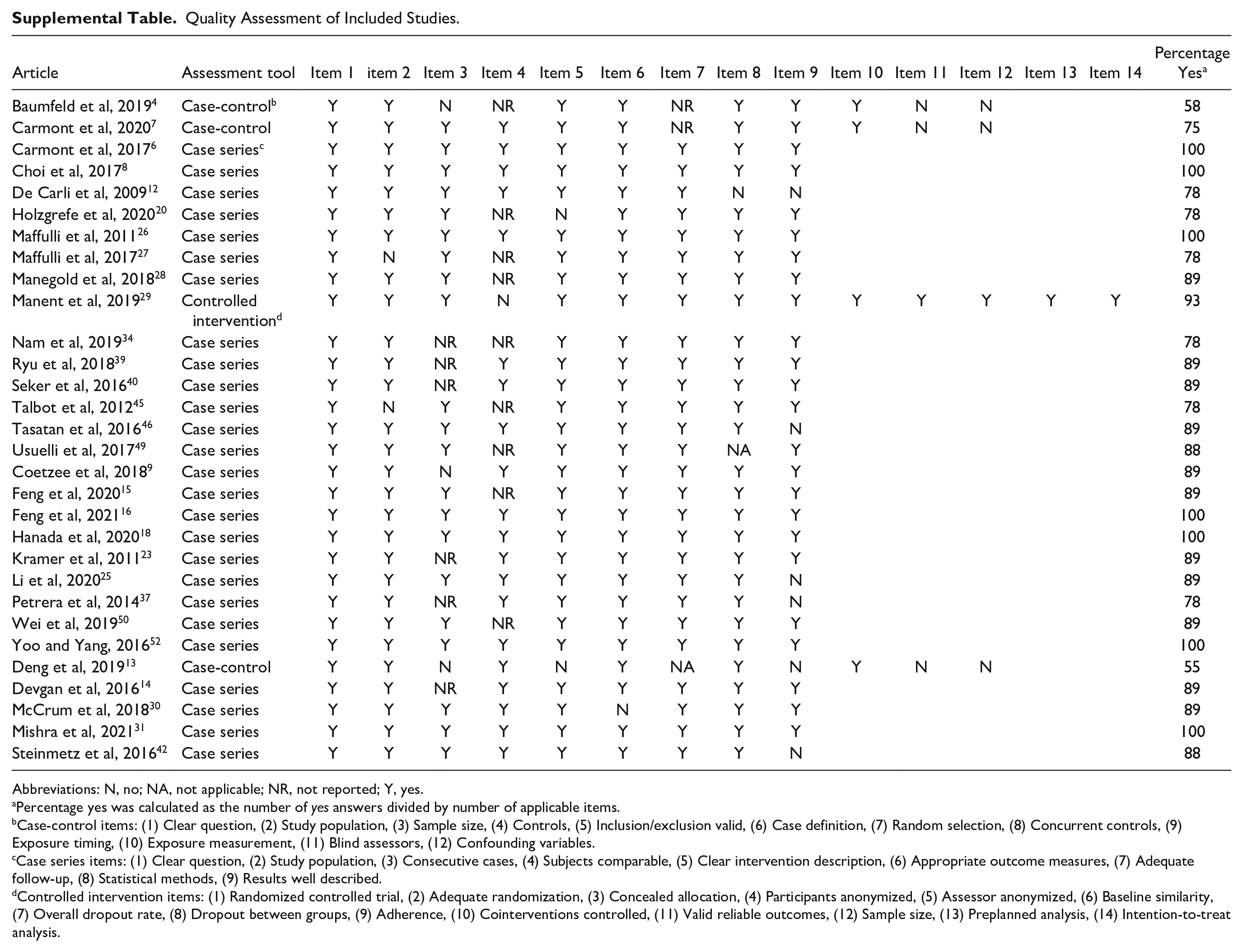
Quality Assessment of Included Studies.
| Article | Assessment tool | Item 1 | item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Item 12 | Item 13 | Item 14 | Percentage Yes a |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baumfeld et al, 20194 | Case-control b | Y | Y | N | NR | Y | Y | NR | Y | Y | Y | N | N | 58 | ||
| Carmont et al, 20207 | Case-control | Y | Y | Y | Y | Y | Y | NR | Y | Y | Y | N | N | 75 | ||
| Carmont et al, 20176 | Case series c | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Choi et al, 20178 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| De Carli et al, 200912 | Case series | Y | Y | Y | Y | Y | Y | Y | N | N | 78 | |||||
| Holzgrefe et al, 202020 | Case series | Y | Y | Y | NR | N | Y | Y | Y | Y | 78 | |||||
| Maffulli et al, 201126 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Maffulli et al, 201727 | Case series | Y | N | Y | NR | Y | Y | Y | Y | Y | 78 | |||||
| Manegold et al, 201828 | Case series | Y | Y | Y | NR | Y | Y | Y | Y | Y | 89 | |||||
| Manent et al, 201929 | Controlled intervention d | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 93 |
| Nam et al, 201934 | Case series | Y | Y | NR | NR | Y | Y | Y | Y | Y | 78 | |||||
| Ryu et al, 201839 | Case series | Y | Y | NR | Y | Y | Y | Y | Y | Y | 89 | |||||
| Seker et al, 201640 | Case series | Y | Y | NR | Y | Y | Y | Y | Y | Y | 89 | |||||
| Talbot et al, 201245 | Case series | Y | N | Y | NR | Y | Y | Y | Y | Y | 78 | |||||
| Tasatan et al, 201646 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | N | 89 | |||||
| Usuelli et al, 201749 | Case series | Y | Y | Y | NR | Y | Y | Y | NA | Y | 88 | |||||
| Coetzee et al, 20189 | Case series | Y | Y | N | Y | Y | Y | Y | Y | Y | 89 | |||||
| Feng et al, 202015 | Case series | Y | Y | Y | NR | Y | Y | Y | Y | Y | 89 | |||||
| Feng et al, 202116 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Hanada et al, 202018 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Kramer et al, 201123 | Case series | Y | Y | NR | Y | Y | Y | Y | Y | Y | 89 | |||||
| Li et al, 202025 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | N | 89 | |||||
| Petrera et al, 201437 | Case series | Y | Y | NR | Y | Y | Y | Y | Y | N | 78 | |||||
| Wei et al, 201950 | Case series | Y | Y | Y | NR | Y | Y | Y | Y | Y | 89 | |||||
| Yoo and Yang, 201652 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Deng et al, 201913 | Case-control | Y | Y | N | Y | N | Y | NA | Y | N | Y | N | N | 55 | ||
| Devgan et al, 201614 | Case series | Y | Y | NR | Y | Y | Y | Y | Y | Y | 89 | |||||
| McCrum et al, 201830 | Case series | Y | Y | Y | Y | Y | N | Y | Y | Y | 89 | |||||
| Mishra et al, 202131 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100 | |||||
| Steinmetz et al, 201642 | Case series | Y | Y | Y | Y | Y | Y | Y | Y | N | 88 |
Abbreviations: N, no; NA, not applicable; NR, not reported; Y, yes.
Percentage yes was calculated as the number of yes answers divided by number of applicable items.
Case-control items: (1) Clear question, (2) Study population, (3) Sample size, (4) Controls, (5) Inclusion/exclusion valid, (6) Case definition, (7) Random selection, (8) Concurrent controls, (9) Exposure timing, (10) Exposure measurement, (11) Blind assessors, (12) Confounding variables.
Case series items: (1) Clear question, (2) Study population, (3) Consecutive cases, (4) Subjects comparable, (5) Clear intervention description, (6) Appropriate outcome measures, (7) Adequate follow-up, (8) Statistical methods, (9) Results well described.
Controlled intervention items: (1) Randomized controlled trial, (2) Adequate randomization, (3) Concealed allocation, (4) Participants anonymized, (5) Assessor anonymized, (6) Baseline similarity, (7) Overall dropout rate, (8) Dropout between groups, (9) Adherence, (10) Cointerventions controlled, (11) Valid reliable outcomes, (12) Sample size, (13) Preplanned analysis, (14) Intention-to-treat analysis.
Ethical Approval
Ethical approval was not sought for the present manuscript because it is a scoping review, and thus ethical approval is not needed. No new patient/participant data were collected; rather all data were obtained from previously published studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.